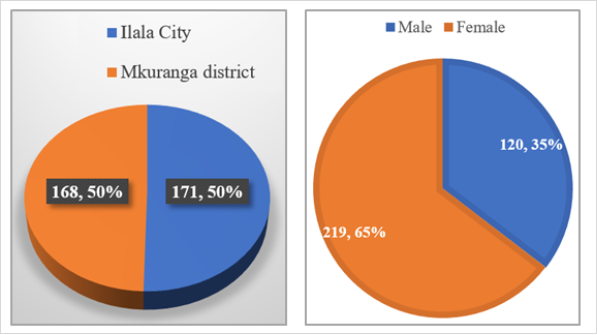
Introduction: Overweight and obesity are significant global public health challenges associated with adverse burdens on the quality of life and mortality due to their association with non-communicable diseases. Early identification and control of these conditions are vital to mitigating their impact. Methods: A cross-sectional study was conducted among 339 respondents in Ilala City (urban) and Mkuranga district (rural) to assess the prevalence and determinants of overweight and obesity among adults. Data were collected on lifestyle, nutrition and demographic characteristics, and anthropometric measurements of height, weight, fat mass%, and waist and hip circumference were measured. Statistical analysis was conducted using SPSS version 27. Results: The overall prevalence of overweight and obesity was 26% and 18.9% respectively. In Ilala City, 61.1% of respondents was either overweight (32.2% or obese (28.7%), and in Mkuranga district, the prevalence of overweight was 19.2% and that of obesity was 8.3%. Key factors negatively associated with overweight and obesity included rural residence (AOR = 0.25; 95%CI (0.14 – 0.47); P = 0.000), income (AOR = 0.2; 95%CI (0.1 – 0.5); P = 0.001), Vigorous physical activities (COR = 0.5; 95%CI (0.3 – 0.7); P =0.002), and consumption of pulses (legumes, nuts and oil seeds) (AOR = 0.1:95%CI (0.01 – 0.2); P = 0.026), and positively associated with sex (AOR = 3.65; 95%CI (2.1 – 6.3); P = 0.000), where by female respondents were more overweight or obese than males, low education (AOR = 7.6; 95%CI (1.2 – 48.5); P = 0.03) in which primary school education were at higher risk of being overweight or obese, and spending less than 75 minutes per week for vigorous physical activities (COR = 2.6; 95%CI (1.7 – 4.12); P = 0.000) were by respondents with sedentary lifestyle are at higher risk of being overweight or obese. Conclusion: The findings suggest that urbanization, sex, education level, physical activity, and dietary habits are significant predictors of overweight and obesity. This serves as a benchmark for planning further studies aiming at reducing the prevalence of overweight and obesity among the adult population through well-designed interventions.
| Published in | Journal of Food and Nutrition Sciences (Volume 13, Issue 4) |
| DOI | 10.11648/j.jfns.20251304.11 |
| Page(s) | 201-216 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2025. Published by Science Publishing Group |
Overweight and Obesity, Lifestyle Factors, Dietary Habits, Ilala City, Mkuranga District, Adults
Total | Ilala city | Mkuranga district | ||||
|---|---|---|---|---|---|---|
Variables | Mean (SD) | IQR | Mean (SD) | IQR | Mean (SD) | IQR |
Weight (kg) | 60.3 ±18.5 | 37-114 | 66.5 ±16.8 | 43-114 | 54 ±18 | 37.2-94 |
Height (cm) | 151 ±34.6 | 141-185 | 155 ±25.3 | 141-185 | 147.6 ±41.8 | 143-184 |
Age (years) | 39.6 ±11 | 18-80 | 38 ±8.4 | 18-63 | 41 ±12.5 | 20-80 |
Fat Mass% (Female) | 20.5 ±17.3 | 9.8-56 | 23.6 ±18.4 | 21.3-56 | 17.3 ±15.4 | 9.8-45 |
Fat Mass% (Male) | 7 ±10 | 5.5-35.3 | 7 ±10.7 | 14.7-31.7 | 6.7 ±9.5 | 5.5-35.3 |
Waist circumference (cm) (female) | 48.9 ±44 | 39-135 | 54.3 ±46.4 | 39-135 | 43.4 ±40.4 | 57-110 |
Hip circumference (cm) (female) | 58 ±52 | 44-141 | 64 ±53 | 44-141 | 53 ±49 | 76-117 |
Waist circumference (cm) (male) | 21 ±35 | 58-109 | 19.9 ±36 | 58-109 | 22.8 ±34 | 58-103 |
Hip circumference (cm) (male) | 24 ±39.7 | 65-115 | 22.3 ±40.3 | 65-115 | 26 ±39 | 65-98 |
SD = Standard deviation, IQR = Interquartile range | ||||||
Variables | Ilala City | Mkuranga district | Total | P - value | |||
|---|---|---|---|---|---|---|---|
n | % | n | % | n | % | ||
Smoking status | |||||||
Smokers | 11 | 6.4 | 17 | 10.1 | 28 | 8.3 | 0.657 |
Non-smokers | 160 | 93.6 | 151 | 89.9 | 311 | 91.7 | |
Smoking pattern | |||||||
Daily smokers | 5 | 45.5 | 4 | 23.5 | 9 | 32.1 | 0.000 |
Weekly smokers | 6 | 54.5 | 13 | 76.5 | 19 | 67.9 | |
Consumption of alcohol | |||||||
Alcohol consumers | 48 | 28.1 | 41 | 24.4 | 89 | 26.3 | 0.211 |
Non-alcohol consumers | 123 | 71.9 | 127 | 75.6 | 250 | 73.7 | |
Alcohol consumption pattern | |||||||
3-4 days per week | 8 | 16.7 | 12 | 29.3 | 20 | 22.5 | 0.235 |
1-2 days per week | 23 | 47.9 | 17 | 41.5 | 40 | 44.9 | |
less than once a month | 8 | 16.7 | 7 | 17.1 | 15 | 16.9 | |
Vigorous intensity activities | |||||||
Yes | 58 | 33.9 | 141 | 83.9 | 199 | 58.7 | 0.000 |
No | 113 | 66.1 | 27 | 16.1 | 140 | 41.3 | |
Moderate intensity activities | |||||||
Yes | 33 | 19.3 | 24 | 14.3 | 57 | 16.8 | 0.305 |
No | 138 | 80.7 | 144 | 85.7 | 282 | 83.2 | |
Walk or use a bicycle for at least 10 minutes continuously | |||||||
Yes | 137 | 80.1 | 119 | 70.8 | 256 | 75.5 | 0.078 |
No | 34 | 19.1 | 49 | 29.2 | 83 | 24.5 | |
Meantime used (minutes) | n | Mean (SD) | n | Mean (SD) | n | Mean (SD) | |
Vigorous intensity activities | 171 | 34.7 ±86.2 | 168 | 136 ±91.9 | 339 | 229.2±227.8 | |
Moderate intensity activities | 171 | 148.6±634 | 168 | 51.6±240.7 | 339 | 100.5±482.9 | |
vigorous-intensity activities are those activities that increase the heart rate between 70% to 85% of your maximum heart rate, Moderate-intensity activities refer to activities that cause the heart rate to increase between 50% and 70%, Walk or using a bicycle for at least 10 minutes continuously means to either walk briskly or ride a Bicycle for a minimum of 10 minutes without stopping, essentially encouraging a short burst of moderate-intensity activities | |||||||
Ilala city | Mkuranga district | Total | ||||||
|---|---|---|---|---|---|---|---|---|
Overweight and obesity | Overweight and obesity | Overweight and obesity | ||||||
Food group | Consumption category | n | % | n | % | n | % | P-value |
Fruit | More than 5 days per week | 7 | 31.8 | 0 | 0 | 7 | 14.9 | 0.449 |
Less than 5 days per week | 41 | 28.3 | 13 | 9.9 | 54 | 19.6 | ||
More than 280g per day | 3 | 25 | 2 | 13.3 | 5 | 18.5 | 0.959 | |
Less than 280g per day | 45 | 29 | 11 | 7.8 | 56 | 19 | ||
Vegetable | More than 5 days per week | 26 | 36.1 | 8 | 9 | 31 | 22.3 | 0.173 |
Less than 5 days per week | 22 | 23.2 | 5 | 7.5 | 30 | 16.3 | ||
More than 280g per day | 10 | 40 | 8 | 18.6 | 18 | 26.5 | 0.072 | |
Less than 280g per day | 38 | 26.8 | 5 | 4.4 | 42 | 16.9 | ||
Added sugars | More than 5 days per week | 10 | 27.8 | 13 | 8.4 | 10 | 27 | 0.179 |
Less than 5 days per week | 38 | 29 | 0 | 0 | 51 | 17.8 | ||
More than 30g per day | 15 | 30.6 | 1 | 7.7 | 16 | 25.8 | 0.121 | |
Less than 30g per day | 33 | 20 | 12 | 8.4 | 45 | 17.2 | ||
Meat/fish | More than 5 days per week | 5 | 50 | 0 | 0 | 5 | 35.7 | 0.1 |
Less than 5 days per week | 43 | 27.4 | 13 | 8.6 | 56 | 18.1 | ||
More than 120g per day | 28 | 30.1 | 7 | 7.1 | 35 | 18.2 | 0.715 | |
Less than 120g per day | 20 | 27 | 6 | 10.5 | 26 | 19.8 | ||
Energy-dense foods | More than 5 days per week | 36 | 28.6 | 8 | 6.3 | 44 | 17.5 | 0.218 |
Less than 5 days per week | 12 | 29.3 | 5 | 16.7 | 17 | 23.9 | ||
More than 580g per day | 11 | 32.4 | 3 | 9.7 | 14 | 21.5 | 0.541 | |
Less than 580g per day | 37 | 27.8 | 10 | 8 | 47 | 18.2 | ||
Pulses | More than 5 days per week | 38 | 29.7 | 12 | 8.5 | 50 | 18.5 | 0.704 |
Less than 5 days per week | 10 | 25.6 | 1 | 7.1 | 11 | 20.8 | ||
More than 290g per day | 9 | 21.4 | 3 | 5.4 | 12 | 12.2 | 0.044 | |
Less than 290g per day | 39 | 31.2 | 10 | 10 | 49 | 21.8 | ||
Variables | Ilala City | Mkuranga district | Total | df | P-value | ||||
|---|---|---|---|---|---|---|---|---|---|
Overweight+Obesity | Overweight+ Obesity | Overweight+ Obesity | |||||||
n | % | n | % | N | % | x2 | |||
Smoking status | |||||||||
Smokers | 6 | 50 | 3 | 18.8 | 9 | 33.3 | 1.591a | 1 | 0.207 |
Non smokers | 97 | 62.2 | 40 | 28.6 | 136 | 45.9 | |||
Alcohol consumption status | |||||||||
Alcohol consumers | 31 | 72.1 | 12 | 30.8 | 44 | 52.4 | 2.574a | 1 | 0.109 |
Non-Alcohol consumers | 71 | 57.3 | 31 | 26.5 | 101 | 42.3 | |||
Place of residence | 102 | 61.1 | 43 | 27.6 | 145 | 44.9 | 36.619a | 1 | 0.000 |
Sex | |||||||||
Female | 78 | 68.4 | 38 | 39.2 | 116 | 55 | 25.015a | 1 | 0.000 |
Male | 24 | 45.3 | 5 | 8.5 | 29 | 25.9 | |||
Vigorous activity | |||||||||
Yes | 35 | 60.3 | 36 | 27.3 | 71 | 35.7 | 9.905a | 2 | 0.007 |
No | 66 | 61.1 | 7 | 29.2 | 73 | 55.3 | |||
Mean time spent for vigorous activity | |||||||||
˂75 minutes | 26 | 54.2 | 33 | 26.2 | 59 | 33.5 | 20.205a | 1 | 0.000 |
≥75 minutes | 76 | 63.9 | 10 | 33.3 | 86 | 58.5 | |||
Moderate activity | |||||||||
Yes | 20 | 62.5 | 8 | 27.3 | 26 | 48.1 | 2.326a | 3 | 0.508 |
No | 81 | 60.9 | 37 | 27.6 | 118 | 44.2 | |||
Mean time spent for moderate activity | |||||||||
˂150 minutes | 90 | 62.1 | 42 | 29 | 132 | 45.5 | 0.449a | 1 | 0.503 |
≥150 minutes | 12 | 54.5 | 1 | 9.1 | 39.4 | ||||
Marital Status | |||||||||
Married | 7 | 58.3 | 2 | 25 | 9 | 45 | 11.894a | 6 | 0.064 |
Not married | 69 | 60.5 | 35 | 26.7 | 104 | 42.4 | |||
Level of education | |||||||||
No formal schooling | 8 | 61.5 | 13 | 21.7 | 21 | 28.8 | 11.907a | 4 | 0.018 |
Primary school | 69 | 67.6 | 23 | 29.9 | 92 | 51.4 | |||
Secondary school | 20 | 50 | 7 | 41.2 | 27 | 47.4 | |||
College/university | 5 | 45.5 | 5 | 38.5 | |||||
Income (TZS) | |||||||||
100,000≤ 500,000 | 8 | 61.5 | 20 | 32.8 | 28 | 36.4 | 25.620a | 5 | 0.000 |
500,000≤ 1,000,000 | 21 | 46.7 | 8 | 13.6 | 29 | 25.9 | |||
1,000,000≤ 5,000,000 | 41 | 63.1 | 10 | 45.5 | 51 | 56.7 | |||
≥5,000,000 | 28 | 73.7 | 4 | 40 | 32 | 66.7 | |||
Variables | Group or category | COR | 95%CI | p-Value | AOR | 95%CI | p-Value |
|---|---|---|---|---|---|---|---|
Place of residence | Mkuranga district | 0.24 | 0.2-0.4 | 0.000 | 0.25 | 0.1-0.5 | 0.000 |
Ilala City | 1 | 1 | |||||
Sex | Female | 3.5 | 2.1-5.7 | 0.000 | 3.6 | 2.1-6.3 | 0.000 |
Male | 1 | 1 | |||||
vigorous activities | Yes | 0.5 | 0.3-0.7 | 0.002 | 1.49 | 0.7-3.3 | 0.3 |
No | 1 | 1 | |||||
Mean time spent on vigorous activities | ˂75 minutes | 2.6 | 1.7-4.12 | 0.000 | 0.6 | 0.3-1.4 | 0.3 |
≥75 minutes | 1 | 1 | |||||
Marital Status | Married | 1.3 | 1.01-1.6 | 0.04 | 1.12 | 0.9-1.4 | 0.4 |
Not married | 1 | 1 | |||||
Level of education | No formal schooling | 0.73 | 0.2-3.3 | 0.7 | 5.4 | 0.8-38.7 | 0.09 |
Primary school | 1.67 | 0.387-7.18 | 0.49 | 7.6 | 1.2-48.5 | 0.03 | |
Secondary school | 1.47 | 0.32-6.67 | 0.62 | 5.4 | 0.8-35.8 | 0.08 | |
College/university | 1 | 1 | |||||
Income (TZS) | ˂100000 | 1 | 1 | ||||
100,000 ≤ 500,000 | 0.28 | 0.13-0.6 | 0.001 | 0.58 | 0.2-1.6 | 0.29 | |
500,000 ≤ 1,000,000 | 0.17 | 0.1-0.3 | 0.000 | 0.2 | 0.1-0.5 | 0.001 | |
1,000,000 ≤ 5,000,000 | 0.67 | 0.3-1.4 | 0.27 | 0.56 | 0.2-1.4 | 0.2 | |
≥ 5,000,000 | 1 | 1 | |||||
Pulses | ≥290g per day | 1.2-1.4 | 0.000 | 0.1 | 0.01-0.2 | 0.026 | |
˂290g per day | 1 | ||||||
BMI | Body Mass Index |
DHS-MIS | Demographic Health Survey and Malaria Indicator Survey |
FM | Fat Mass |
WHR | Waist Hip Ratio |
NCDs | Non-communicable Diseases |
WHO | World Health Organization |
| [1] | Horn, C., Laupsa-Borge, J. Andersen, A. I., Dyer, L., Revheim, I., Leikanger, T & Dankel, S. N. (2022). Meal patterns associated with energy intake in people with obesity. British Journal of Nutrition, 128(2), 334-344. |
| [2] | Makbel, K., Mwanri, A., & Ramaiya, K. (2022). Total body fat is associated with increased risk for pre-diabetes and hypertension among secondary school adolescents in Morogoro Region, Tanzania; Volume. 13. |
| [3] | Das, M., Sauceda, C., & Webster, N. J. (2021). Mitochondrial dysfunction in obesity and reproduction. Endocrinology, 162(1), bqaa 158. |
| [4] | Castro-Porras, L. V., Rojas-Russell, M. E., Villanueva-Sánchez, J., & López-Cervantes, M. (2019). An anthropometry-based equation of fat mass percentage as a valid discriminator of obesity. Public health nutrition, 22(7), 1250-1258. |
| [5] | World Health Organization. (2011). Waist circumference and waist-hip ratio: report of a WHO expert consultation, Geneva, December 2008. Page 27. |
| [6] | Mamdouh, H., Hussain, H. Y., Ibrahim, G. M., Alawadi, F., Hassanein, M., Al Zarooni, A. & Alnakhi, W. K. (2023). Prevalence and associated risk factors of overweight and obesity among adult population in Dubai: A population-based cross-sectional survey in Dubai, the United Arab Emirates. BMJ open, 13(1), e062053. |
| [7] |
Tim Lobstein, Rachel Jackson-Leach. Jaynaide Powis, Hannah Brinsden and Maggie Gray (2023) World_Obesity_Atlas_2023.
https://data.worldobesity.org/publications/WOF-Obesity-Atlas-V5.pdf |
| [8] | Zubery, D., Kimiywe, J., & Martin, H. D. (2021). Prevalence of overweight and obesity, and its associated factors among health-care workers, teachers, and bankers in Arusha City, Tanzania. Diabetes, Metabolic Syndrome and Obesity, 455-465. |
| [9] | Ministry of Health (MoH) [Tanzania Mainland], Ministry of Health (MoH) [Zanzibar], National Bureau of Statistics (NBS), Ofice of the Chief Government Statistician (OCGS), and ICF. Tanzania Demographic and Health Survey and Malaria Indicator Survey 2022 Final Report. Dodoma, Tanzania, and Rockville, Maryland, USA: MoH, NBS, OCGS, and ICF; 2023. |
| [10] | Yang, H., An, R., Clarke, C. V., & Shen, J. (2023). Impact of economic growth on physical activity and sedentary behaviors: a Systematic Review. Public Health, 215, 17-26. |
| [11] | Ignowski, L., Belton, B., Tran, N., & Ameye, H. (2023). Dietary inadequacy in Tanzania is linked to the rising cost of nutritious foods and consumption of food-away-from-home. Global Food Security, 37, 100679. Page 2-4. |
| [12] | Pallangyo, P., Mkojera, Z. S., Hemed, N. R., Swai, H. J., Misidai, N., Mgopa, L., & Janabi, M. (2020). Obesity epidemic in urban Tanzania: a public health calamity in an already overwhelmed and fragmented health system. BMC Endocrine Disorders, 20(1). |
| [13] | Massawe, E. S., & Msollo, S. S. (2023). Knowledge and Perceptions on Overweight and Obesity among Adults in Same District, Tanzania. East African Journal of Science, Technology and Innovation, 4. |
| [14] | Alemi, S., Nakamura, K., Arab, A. S., Mashal, M. O., Tashiro, Y., Seino, K., & Hemat, S. (2023). Prevalence, determinants, and association of overweight/obesity with non-communicable disease-related biomedical indicators: A cross-sectional study in schoolteachers in Kabul, Afghanistan. PLOS Global Public Health, 3(3), e0001676. |
| [15] | Charan, J., & Biswas, T. (2013). How to calculate sample size for different study designs in medical research? Indian journal of psychological medicine, 35(2), 121-126. |
| [16] | Riley, L., Guthold, R., Cowan, M., Savin, S., Bhatti, L., Armstrong, T., & Bonita, R. (2016). The World Health Organization STEPwise approach to non-communicable disease risk-factor surveillance: methods, challenges, and opportunities. American Journal of Public Health, 106 (1), 74-78. |
| [17] | Consultation, W. E. (2008). Waist circumference and waist-hip ratio. Report of a WHO Expert Consultation. Geneva: World Health Organization, 2008, 8-11. |
| [18] | Bull, F. C., Al-Ansari, S. S., Biddle, S., Borodulin, K., Buman, M. P., Cardon, G., & Willumsen, J. F. (2020). World Health Organization 2020 guidelines on physical activity and sedentary behaviour. British journal of sports medicine, 54(24), page 1456. |
| [19] | Ministry of Health of the united Republic of Tanzania (MoH). Tanzania Mainland Food-Based Dietary Guidelines for a Healthy Population: Technical Recommendations. Ministry of Health: Dodoma, Tanzania; 2023. |
| [20] | World Health Organization. (2019). Sustainable healthy diets: Guiding principles. Food & Agriculture Org. Page 17. |
| [21] | Kagaruki, G. B., Mahande, M. J., Kimaro, G. D., Ngadaya, E. S., Mayige T, M., Selemani, M., & Bonfoh, B. (2021). Prevalence and Correlates of Cardio-Metabolic Risk Factors Among Regular Street Food Consumers in Dar es Salaam, Tanzania. Diabetes, Metabolic Syndrome and Obesity, 1011-1024. |
| [22] | Msollo, S. S., Shausi, G. L., & Mwanri, A. W. (2024). Prevalence, knowledge and practices on prevention and management of overweight and obesity among adults in Dodoma City, Tanzania. Plos one, 19(1), e0297665. |
| [23] | Mekonnen, T., Animaw, W., & Seyum, Y. (2018). Overweight/obesity among adults in North-Western Ethiopia: a community-based cross-sectional study. Archives of public health, 76, 1-6. |
| [24] | Gupta, R. D., Frank, H. A., Akonde, M., Mazumder, A., Siddika, N., Apu, E. H., & Chakraborty, P. A. (2023). Rural-Urban Differences in Prevalence and Associated Factors of Underweight and Overweight/Obesity among Bangladeshi Adults: Evidence from Bangladesh Demographic and Health Survey 2017–2018. Epidemiologia, 4(4), 505-520. |
| [25] | Holmes, C. J., & Racette, S. B. (2021). The utility of body composition assessment in nutrition and clinical practice: an overview of current methodology. Nutrients, 13(8), 2493 Page 4-5. |
| [26] | Zhu, Q., Huang, B., Li, Q., Huang, L., Shu, W., Xu, L., & Liu, P. (2020). Body mass index and waist-to-hip ratio misclassification of overweight and obesity in Chinese military personnel. Journal of physiological anthropology, 39. |
| [27] | Khamis, A. G., Ntwenya, J. E., Senkoro, M., Mfinanga, S. G., Kreppel, K., Mwanri, A. W., & Kwesigabo, G. (2021). Association between dietary diversity with overweight and obesity: A cross-sectional study conducted among pastoralists in Monduli District in Tanzania. Plos one, 16(1), e0244813. |
| [28] | Sigei, E. C., Okinyi, V. P., Kariuki, P. K., Kariuki, L., & Kimani, J. (2018). Prevalence of Overweight/Obesity and Some Associated Factors among Rural/Urbanites of Uasin-Gishu County, Kenya: A Cross-Sectional Study. Journal of Nutritional Sciences and Dietetics, 109-116. |
| [29] | George, J. M., Mpogole, Z., Mgongo, M., Mamseri, R., Leyaro, B. J., Mauka, W., & Msuya, S. E. (2021). Prevalence and Factors Associated with Overweight or Obesity Among Primary and Secondary School Teachers in Moshi Municipality, Kilimanjaro, Tanzania. |
| [30] | Clark, T. D., Reichelt, A. C., Ghosh-Swaby, O., Simpson, S. J., & Crean, A. J. (2022). Nutrition, anxiety and hormones. Why sex differences matter in the link between obesity and behavior. Physiology & Behavior, 247, 113713. |
| [31] | Zhang Jiao, Z. J., Xu LingZhong, X. L., Li JiaJia, L. J., Sun Long, S. L., Qin WenZhe, Q. W., Ding Gan, D. G., & Zhou ChengChao, Z. C. (2019). Gender differences in the association between body mass index and health-related quality of life among adults: a cross-sectional study in Shandong, China. |
| [32] | Shah, B., Cost, K. T., Fuller, A., Birken, C. S., & Anderson, L. N. (2020). Sex and gender differences in childhood obesity: contributing to the research agenda. BMJ Nutrition, Prevention & Health, 3(2), 387. |
| [33] | Younis, J., Jiang, H., Fan, Y., Wang, L., Li, Z., Jebril, M., & Hui, Z. (2023). Prevalence of overweight, obesity, and associated factors among healthcare workers in the Gaza Strip, Palestine: A cross-sectional study. Frontiers in Public Health, 11, 1129797. |
| [34] | Mosha, D., Paulo, H. A., Mwanyika-Sando, M., Mboya, I. B., Madzorera, I., Leyna, G. H., & Fawzi, W. W. (2021). Risk factors for overweight and obesity among women of reproductive age in Dar es Salaam, Tanzania. BMC nutrition, 7, 1-10. |
| [35] | Ogden, C. L. (2017). Prevalence of obesity among adults, by household income and education—United States, 2011–2014. MMWR. Morbidity and mortality weekly report, 66. |
| [36] | Mosli, H. H., Kutbi, H. A., Alhasan, A. H., & Mosli, R. H. (2020). Understanding the interrelationship between education, income, and obesity among adults in Saudi Arabia. Obesity facts, 13(1), 77-85. |
| [37] | Ahmed, K. Y., Rwabilimbo, A. G., Abrha, S., Page, A., Arora, A., Tadese, F., & Global Maternal and Child Health Research collaboration (GloMACH). (2020). Factors associated with underweight, overweight, and obesity in reproductive age Tanzanian women. PloS one, 15(8), e0237720. |
| [38] | Mangemba, N. T., & San Sebastian, M. (2020). Societal risk factors for overweight and obesity in women in Zimbabwe: a cross-sectional study. BMC public health, 20, 1-8. |
| [39] | Oppert, J. M., Bellicha, A., van Baak, M. A., Battista, F., Beaulieu, K., Blundell, J. E, & Busetto, L. (2021). Exercise training in the management of overweight and obesity in adults: Synthesis of the evidence and recommendations from the European Association for the Study of Obesity Physical Activity Working Group. Obesity reviews, 22, e13273. |
| [40] | Mandefro, M., Shore, H., Hailu, S., Ayele, F., Tekola, A., Shawel, S., & Gebremichael, B. (2024). Overweight and obesity and associated factors among public and private secondary school adolescent students in Harar city, Eastern Ethiopia: A comparative cross-sectional study. Medicine, 103(21), e38271. |
| [41] | Garber, C. E. (2019). The health benefits of exercise in overweight and obese patients. Current sports medicine reports, 18(8), 287-291. |
| [42] | Koolhaas, C. M., Dhana, K., Schoufour, J. D., Ikram, M. A., Kavousi, M., & Franco, O. H. (2017). Impact of physical activity on the association of overweight and obesity with cardiovascular disease: The Rotterdam Study. European journal of preventive cardiology, 24(9), 934-941. |
| [43] | Didinger, C., & Thompson, H. J. (2022). The role of pulses in improving human health: A review. Legume Science, 4(4), e147. |
| [44] | Zerón-Rugerio, M. F., & Izquierdo-Pulido, M. (2019). Legumes and Obesity. |
| [45] | Ferreira, H., Vasconcelos, M., Gil, A. M., & Pinto, E. (2021). Benefits of pulse consumption on metabolism and health: A systematic review of randomized controlled trials. Critical reviews in food science and nutrition, 61(1), 85-96. |
| [46] | Fernández-Fígares Jiménez, M. D. C. (2024). A Whole Plant–Foods Diet in the Prevention and Treatment of Overweight and Obesity: From Empirical Evidence to Potential Mechanisms. Journal of the American Nutrition Association, 1-19. |
| [47] | Grdeń, P., & Jakubczyk, A. (2023). Health benefits of legume seeds. Journal of the Science of Food and Agriculture, 103(11), 5213-5220. |
APA Style
Fransisco, C. C., Kinabo, J., Pacific, R. (2025). A Prevalence of Overweight and Obesity and Associated Lifestyle Patterns Among Adults in Ilala City and Mkuranga District, Tanzania. Journal of Food and Nutrition Sciences, 13(4), 201-216. https://doi.org/10.11648/j.jfns.20251304.11
ACS Style
Fransisco, C. C.; Kinabo, J.; Pacific, R. A Prevalence of Overweight and Obesity and Associated Lifestyle Patterns Among Adults in Ilala City and Mkuranga District, Tanzania. J. Food Nutr. Sci. 2025, 13(4), 201-216. doi: 10.11648/j.jfns.20251304.11
@article{10.11648/j.jfns.20251304.11,
author = {Chrispin Clavery Fransisco and Joyce Kinabo and Renatha Pacific},
title = {A Prevalence of Overweight and Obesity and Associated Lifestyle Patterns Among Adults in Ilala City and Mkuranga District, Tanzania},
journal = {Journal of Food and Nutrition Sciences},
volume = {13},
number = {4},
pages = {201-216},
doi = {10.11648/j.jfns.20251304.11},
url = {https://doi.org/10.11648/j.jfns.20251304.11},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.jfns.20251304.11},
abstract = {Introduction: Overweight and obesity are significant global public health challenges associated with adverse burdens on the quality of life and mortality due to their association with non-communicable diseases. Early identification and control of these conditions are vital to mitigating their impact. Methods: A cross-sectional study was conducted among 339 respondents in Ilala City (urban) and Mkuranga district (rural) to assess the prevalence and determinants of overweight and obesity among adults. Data were collected on lifestyle, nutrition and demographic characteristics, and anthropometric measurements of height, weight, fat mass%, and waist and hip circumference were measured. Statistical analysis was conducted using SPSS version 27. Results: The overall prevalence of overweight and obesity was 26% and 18.9% respectively. In Ilala City, 61.1% of respondents was either overweight (32.2% or obese (28.7%), and in Mkuranga district, the prevalence of overweight was 19.2% and that of obesity was 8.3%. Key factors negatively associated with overweight and obesity included rural residence (AOR = 0.25; 95%CI (0.14 – 0.47); P = 0.000), income (AOR = 0.2; 95%CI (0.1 – 0.5); P = 0.001), Vigorous physical activities (COR = 0.5; 95%CI (0.3 – 0.7); P =0.002), and consumption of pulses (legumes, nuts and oil seeds) (AOR = 0.1:95%CI (0.01 – 0.2); P = 0.026), and positively associated with sex (AOR = 3.65; 95%CI (2.1 – 6.3); P = 0.000), where by female respondents were more overweight or obese than males, low education (AOR = 7.6; 95%CI (1.2 – 48.5); P = 0.03) in which primary school education were at higher risk of being overweight or obese, and spending less than 75 minutes per week for vigorous physical activities (COR = 2.6; 95%CI (1.7 – 4.12); P = 0.000) were by respondents with sedentary lifestyle are at higher risk of being overweight or obese. Conclusion: The findings suggest that urbanization, sex, education level, physical activity, and dietary habits are significant predictors of overweight and obesity. This serves as a benchmark for planning further studies aiming at reducing the prevalence of overweight and obesity among the adult population through well-designed interventions.},
year = {2025}
}
TY - JOUR T1 - A Prevalence of Overweight and Obesity and Associated Lifestyle Patterns Among Adults in Ilala City and Mkuranga District, Tanzania AU - Chrispin Clavery Fransisco AU - Joyce Kinabo AU - Renatha Pacific Y1 - 2025/07/08 PY - 2025 N1 - https://doi.org/10.11648/j.jfns.20251304.11 DO - 10.11648/j.jfns.20251304.11 T2 - Journal of Food and Nutrition Sciences JF - Journal of Food and Nutrition Sciences JO - Journal of Food and Nutrition Sciences SP - 201 EP - 216 PB - Science Publishing Group SN - 2330-7293 UR - https://doi.org/10.11648/j.jfns.20251304.11 AB - Introduction: Overweight and obesity are significant global public health challenges associated with adverse burdens on the quality of life and mortality due to their association with non-communicable diseases. Early identification and control of these conditions are vital to mitigating their impact. Methods: A cross-sectional study was conducted among 339 respondents in Ilala City (urban) and Mkuranga district (rural) to assess the prevalence and determinants of overweight and obesity among adults. Data were collected on lifestyle, nutrition and demographic characteristics, and anthropometric measurements of height, weight, fat mass%, and waist and hip circumference were measured. Statistical analysis was conducted using SPSS version 27. Results: The overall prevalence of overweight and obesity was 26% and 18.9% respectively. In Ilala City, 61.1% of respondents was either overweight (32.2% or obese (28.7%), and in Mkuranga district, the prevalence of overweight was 19.2% and that of obesity was 8.3%. Key factors negatively associated with overweight and obesity included rural residence (AOR = 0.25; 95%CI (0.14 – 0.47); P = 0.000), income (AOR = 0.2; 95%CI (0.1 – 0.5); P = 0.001), Vigorous physical activities (COR = 0.5; 95%CI (0.3 – 0.7); P =0.002), and consumption of pulses (legumes, nuts and oil seeds) (AOR = 0.1:95%CI (0.01 – 0.2); P = 0.026), and positively associated with sex (AOR = 3.65; 95%CI (2.1 – 6.3); P = 0.000), where by female respondents were more overweight or obese than males, low education (AOR = 7.6; 95%CI (1.2 – 48.5); P = 0.03) in which primary school education were at higher risk of being overweight or obese, and spending less than 75 minutes per week for vigorous physical activities (COR = 2.6; 95%CI (1.7 – 4.12); P = 0.000) were by respondents with sedentary lifestyle are at higher risk of being overweight or obese. Conclusion: The findings suggest that urbanization, sex, education level, physical activity, and dietary habits are significant predictors of overweight and obesity. This serves as a benchmark for planning further studies aiming at reducing the prevalence of overweight and obesity among the adult population through well-designed interventions. VL - 13 IS - 4 ER -
Department of Human Nutrition and Consumer Sciences, Sokoine University of Agriculture, Morogoro, Tanzania
Department of Human Nutrition and Consumer Sciences, Sokoine University of Agriculture, Morogoro, Tanzania
Department of Human Nutrition and Consumer Sciences, Sokoine University of Agriculture, Morogoro, Tanzania
Information