Abstract
Introduction: Otologic surgery is particularly suitable for outpatient surgery, which accounts for more than 50% of all surgeries performed in North America. Our aim was to report our experience to identify the benefits and limitations of outpatient otologic surgery in our context. Materials and methods: We conducted an observational, descriptive and retrospective study from January 2022 to December 2023, including 41 patients at the Gabriel Toure University Hospital in Bamako. We included cases of myringoplasty and antro-atticotomies. Results: The extreme ages of our patients are between 02 and 60 years old with an average of 29.5 years. Males accounted for 37.5% and 62.5% females. Myringoplasty affected the left and right sides in the same proportion (28.1%) and was bilateral in 14 cases (43.8%). As for antro-atticotomy, it concerned the right side in 06 cases and the left side in 03 cases. The average operating time was 30 minutes for myringoplasty and 50 minutes for antro-atticotomy. The main complications recorded were dizziness and vomiting in the immediate postoperative period and were encountered in 03 patients. All our patients were discharged the same day with a monitoring time of between 03 and 6 hours. No readmission has been carried out. Conclusion: when the selection criteria are met, outpatient otological surgery could be an essential element for an effective use of fairly limited resources in our context.
Keywords
Otological, Ambulatory, Myringoplasty, Antro-Atticotomy
1. Introduction
Outpatient surgery or "day surgery" is defined as "surgical procedures that are generally scheduled, performed under technical conditions that imperatively require the safety of an operating room, under variable modes of anesthesia and followed by postoperative follow-up allowing the patient to be discharged on the same day of the operation without additional risk
| [1] | Florian Roux. Evolution of the outpatient otologic surgery activity from 2010 to 2015. Doctoral thesis in medicine. Brest: University of Western Brittany, 2017. |
| [2] | A. Uziel. outpatient otological surgery. European Annals of Otorhinolaryngology and Head and Neck Diseases 134 (2017) 249–25: http://dx.doi.org/10.1016/j.anorl.2016.11.008 |
[1, 2]
. The clinical, economic, and social benefits associated with excellent safety and low morbidity rates have popularized outpatient surgery in many countries
| [1] | Florian Roux. Evolution of the outpatient otologic surgery activity from 2010 to 2015. Doctoral thesis in medicine. Brest: University of Western Brittany, 2017. |
| [3] | P. Lemos et al. Patient satisfaction after outpatient surgery. Journal of Clinical Anesthesia (2009) 21, 200–205:
https://doi.org/10.1016/j.jclinane.2008.08.016 |
[1, 3]
. It accounts for more than 50% of all surgeries performed in many countries in North America, Europe, and Oceania
. ENT surgery and otologic surgery in particular are particularly suitable for outpatient surgery. Classically, a distinction is made between minor surgical procedures, such as the placement of a tympanostomy aerator or myringoplasty without elevation of the tympanomeatal flap, and major surgical procedures, such as tympanoplasty with mastoidectomy or ossicle surgery
| [4] | DS Lazard, F. Donne, JB Lecanu. Outpatient surgery in otology: impact study of a dedicated organizational model. European Annals of Otorhinolaryngology and Head and Neck Diseases 136 (2019) 465-468. |
| [5] | S. Bonnafousun, R. Hermannb, S. Zaoucheun, S. Tringaliun, M. Fieuxun. Evolution and safety of ambulatory surgery of the major ear. European Annals of Otorhinolaryngology and Head and Neck Diseases 138 (2021) 141–145. |
[4, 5]
.
Our study was motivated by the fact that the activity of conventional surgery has been significantly reduced due to the coronavirus pandemic. We have therefore initiated this approach in order to offer patients care in the best conditions without having to stay in hospitals for a long time with all the risks that this entails. To allow these patients to resume their normal activities. Our aim was to report our experience to identify the benefits and limitations of outpatient otologic surgery in our context.
2. Materials and Methods
2.1. Study Design
We conducted an observational, descriptive and retrospective study from January 2022 to December 2023, including 41 patients at the Gabriel TourE University Hospital in Bamako.
2.2. Study Setting and Population
The Gabriel Hospital is the hospital that houses the largest ENT department in Mali. These were patients with otologic disorders.
2.3. Population
The study population was defined as any patient who had presented with an ear condition and had not undergone outpatient surgery. The sampling was conducted exhaustively.
We included cases of myringoplasties and mastoidectomies (antro-atticotomies) that met our inclusion criteria, which were: living close to a hospital; Having a telephone contact is not being alone at home.
All patients classified as unstable or A.S.A 4 and at risk of hemorrhage, thrombosis or neurological aggravation, with a particular history (cardiovascular, pleuropulmonary; diabetes, sickle cell anemia) were excluded.
2.4. Surgical Procedure
For all patients, we premedicated with midazolam (0.2 to 0.3 mg/kg IVL), dexamethasone (1 amperage of 4 mg IVL), paracetamol (60 mg/kg) and nefopam 20 mg (1 amp IVL, except for children). Antibiotic prophylaxis was based on ceftriaxone (2 g IVL and 80 mg/kg for children) 30 minutes before incision. Antro-atticotomies were performed under general anesthesia with the retroauricular approach; and myringoplasty under local anesthesia with lidocaine 2% adrenaline (1 ml at 12 h, at 6 o'clock and on the posterior wall of the external ear canal) by transmeatal route.
2.5. Criteria for Discharge from the Clinic and Post-operative Follow-up
Discharge was allowed after a maximum of 6 hours for all patients and telephone contact was made every 6 hours for follow-up of pain and other complications such as bleeding, vomiting and dizziness.
The first appointment was scheduled after 5 days when the bandage and strands of the external ear canal were removed and the patient was not put on ear drops with antibiotics and corticosteroids. Patients were seen weekly for 1 month and monthly for 6 months, and then one year after.
2.6. Variables
Age, sex, Clinical aspect: hypoacusis, otorrhea, the type of tympanic membrane perforation and laterality. The tympanic membrane perforation is defined as any discontinuity of the tympanic membrane that communicates the middle ear with the external auditory canal. It includes subtotal, total, and marginal perforations. The type of otological condition, the mode of local or general anesthesia, and the medication administered prior to the procedure. Audiometric data, post-operative complications: nausea, vomiting, facial paralysis, pain. The duration of the surgery, post-operative follow up over two years: Graft in place, recurrence of otological conditions infections at the surgical sitepost-operative monitoring time of 0 - 6 hours’ patient satisfaction/pain.
2.7. Data Ressources
Collection Tools: We designed questionnaires that allowed us to gather the information contained in the patients' records.
Technique: We collected the records of patients who met our selection criteria.
Support for data collection: A complete ENT examination was performed on all patients. The data were recorded on a survey form designed for this purpose.
2.8. Sample Size
The sample size was calculated using a unique proportion of patients who underwent tympanoplasty and mastoidectomy on an outpatient basis. It was exhaustive. The sample was set at 41 patients.
2.9. Ethical Considerations
Informed consent from patients was obtained verbally and ethics commission approval was obtained.
2.10. Analysis and Data Entry
Data entry was performed by Microsoft Office Word 2016, graphs by Excel 2016 and exported to SPSS (Statistical Package for Social Sciences) version 22.0 for analytical study.
3. Results
3.1. Demographic Characteristics of the Participants
We recorded 41 patients in this study. The age of our patients ranged from 02 to 60 years with an average age of 29.5 years. The majority of women (62.5%) with a sex ratio (M/F) of 0.6 (
Table 1). The mastoidectomy was performed in 55.6% on the male subject. The myringoplasty was performed in 63.5% on the female subject (Table
1). Local anesthesia was performed in cases of myringoplasties. All cases of mastoidectomy were performed under general anesthesia.
Table 1. Sociodemographic aspects of patients, recruited in ENT hospitalization at the university hospital of Gabriel Toure of Bamako City(Mali) from January 2022 to December 2023.
| Average age | Male | Female |
Mastoidectomy | 30.8 years | 55,6% | 44,4% |
Myringoplasty | 29.2 years | 37,5% | 63,5% |
Total Study | 29.5 years | 41,5% | 58,5% |
3.2. Clinical Characteristics of Participants
Hearing loss and otorrhea were the main reasons for consultation in 100%. Perforation was subtotal in 23 cases (56.1%), total in 17 cases (41.5%) and marginal in 1 case (2.4%) (
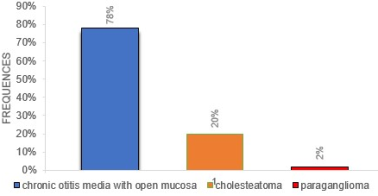
Table 3). Our surgical indications were mainly open mucosal otitis in 78.1% of cases (all myringoplasties) and cholesteatoma in 19.5% with one case of tympanojugular paraganglioma (
Figure 1). Myringoplasty involved the left and right sides in the same proportion (28.1% each) and it was bilateral in 14 cases (43.8%). As for the mastoidectomy, it concerned the right side in 06 cases or 66.7% and the left side in 03 cases or 33.3%. (
Table 2). The duration of the operation ranged from 25 to 30 minutes for myringoplasty and from 45 minutes to 1 hour and 20 minutes for mastoidectomy. Tone audiometry was available in all cases where it was possible with an average hearing loss ranging from 25 to 40 dB.
Figure 1. The different surgical indications found in patients.
Table 2. Distribution of patients by side operated, recruited in ENT hospitalization at the university hospital of Gabriel Toure of Bamako City(Mali) from January 2022 to December 2023.
| Right Side | Left | Bilateral |
Mastoidectomy | 66,7% | 33,3% | 00% |
Myringoplasty | 28,1% | 28,1% | 43,8% |
Total | 36,6% | 29,3% | 34,1% |
Table 3. Clinical aspects and operative indications of patients, recruited in ENT hospitalization at the university hospital of Gabriel Toure of Bamako City(Mali) from January 2022 to December 2023.
| Reason for consultation | Perforation Type | Otology affections |
Hypoacusis/otorrhea | Subtotal | Total | Marginal | OMO | Paragangliomas | Cholesteatoma |
Mastoidectomy | 100% | 00% | 100% | 00% | 00% | 11,1% | 88,9% |
Myringoplasty | 100% | 71,2% | 25% | 3,1% | 100% | 00% | 00% |
Total Study | 100% | 56,1% | 41,5% | 2,4% | 78,1% | 2,4% | 19,5% |
3.3. Post-operative Outcome of the Study Participants
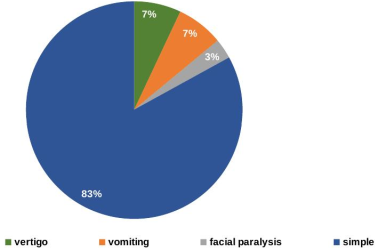
The discharge of all our patients was authorized after six hours.The discharge prescription was made based on paracetamol.No patient has complained of pain and no readmissions have occurred. These complications occurred within the first two hours of the surgery and resolved spontaneously. The complications, or rather adverse effects experienced after myringoplasty. were vomiting and dizziness in 3 cases (9.4%) and one case of transient peripheral facial paralysis (
Figure 2). For antro-atticotomies, no complications or adverse effects were observed. The postoperative follow-up has been established for a duration of two years. The anatomical result was satisfactory in 95% after one year of follow-up for myringoplasty. We had a case of recurrence after 2 years after a mastoidectomy with otorrhea and evaluation is ongoing.
Figure 2. Signs found in the first postoperative hour.
4. Discussion
All major middle ear surgeries can be safely performed on an outpatient basis, from simple tympanoplasty with or without ossiculoplasty to cholesteatoma surgery
| [5] | S. Bonnafousun, R. Hermannb, S. Zaoucheun, S. Tringaliun, M. Fieuxun. Evolution and safety of ambulatory surgery of the major ear. European Annals of Otorhinolaryngology and Head and Neck Diseases 138 (2021) 141–145. |
[5]
. Due to the limited technical platform and the absence of a unit dedicated to outpatient surgery, we limited ourselves to cases of myringoplasties and antro-atticotomies under general anesthesia.
In our study, the mean age was 29.5 years and this value is close to that found by F. Troux and lower than that of S. Bonnafous et al. With 28.5 and 45 years old respectively.
In the literature, we did not find an upper age limit
| [5] | S. Bonnafousun, R. Hermannb, S. Zaoucheun, S. Tringaliun, M. Fieuxun. Evolution and safety of ambulatory surgery of the major ear. European Annals of Otorhinolaryngology and Head and Neck Diseases 138 (2021) 141–145. |
| [6] | Anesthetic management of patients in outpatient hospitalization. Ann Fr Anesth Reanim 2010; 29: 67–72. |
[5, 6]
, although a minimum age of 1 year is recommended due to the particularly high risk of sudden death in this group
. In our study, the minimum age was 02 years. The female sex was in the majority with 58.5%, this result is consistent with those found by P. Lemos et al and S. Bonnafous et al.
| [3] | P. Lemos et al. Patient satisfaction after outpatient surgery. Journal of Clinical Anesthesia (2009) 21, 200–205:
https://doi.org/10.1016/j.jclinane.2008.08.016 |
| [5] | S. Bonnafousun, R. Hermannb, S. Zaoucheun, S. Tringaliun, M. Fieuxun. Evolution and safety of ambulatory surgery of the major ear. European Annals of Otorhinolaryngology and Head and Neck Diseases 138 (2021) 141–145. |
[3, 5]
which had a percentage of females with 56.5% and 52.5% respectively. We did not find a relationship between outpatient surgery in otology and female sex.
The use of midazolam as a premedication reduces not only preoperative anxiety, but also postoperative pain; It also facilitates the process of patient release by reducing adverse effects
. Analgesics used in outpatient surgery should be such that they increase patient comfort with adequate pain control and do not cause postoperative sedation or nausea/vomiting
| [7] | Khan MM, Parab SR. Day care ear surgery: our experience of 4 years. Indian J Otolaryngol Head Neck Surg. 2012 Sep; 64(3): 280-4. https://doi.org/10.1007/s12070-011-0303-x |
| [8] | R. D. Miller, "Miller's Anesthesia," sixth edition, Elsevier Churchill Livingstone, pp. 1227-1264, 2005. |
| [9] | Heilbronn, Cameron et al. Adult outpatient otological surgery: Unexpected revisits and complications. The laryngoscope,7(2020): 1788-1791. https://doi.org/10.1002/lary.28346 |
[7-9]
. The most recent guidelines have found medical contraindications (unstable ASA 3 or ASA 4 score, morbid obesity and obstructive sleep apnea syndrome treated with a continuous positive airway pressure machine) and social contraindications (not understanding postoperative instructions and being alone on the first postoperative night) to outpatient surgery.
Most otologic surgery procedures can be performed with a very low risk of bleeding and excellent postoperative pain management, so for Uziel, 70% of patients could reasonably be operated on an outpatient basis
. According to the Royal College of Surgeons of England, the readmission rate after outpatient surgery is between 2 and 3%
| [5] | S. Bonnafousun, R. Hermannb, S. Zaoucheun, S. Tringaliun, M. Fieuxun. Evolution and safety of ambulatory surgery of the major ear. European Annals of Otorhinolaryngology and Head and Neck Diseases 138 (2021) 141–145. |
[5]
. Heilbronn C et al found a readmission rate of 5.2% after the first 30 days of surgery and among the causes of these readmissions were: urinary infection and/or retention in 93 cases, otalgia in 85 cases, dizziness in 80 cases, nausea/vomiting in 69 cases, bleeding and/or infection of the surgical site in 14 cases and facial paralysis in less than 10 cases for a total of 16709 patients operated on an outpatient basis
| [10] | Bawazeer N. Office-Based Middle Ear Surgery Under Local Anesthesia: A Contemporary Review. J Clin Med Res. 2025 Jul 31; 17(7): 365-374. https://doi.org/10.14740/jocmr6279 |
[10]
. In 93% of cases, pediatric otologic surgery was performed on an outpatient basis in the series of Pezier
| [11] | Pézier T, Stimpson P, Kanegaonkar RG, Bowdler DA. Ear, nose and throat day-case surgery at a district general hospital. Ann R Coll Surg Engl. 2009 Mar; 91(2): 147-51.
https://doi.org/10.1308/003588409X359358 |
[11]
. We did not readmit, however we encountered in the immediate postoperative period: 3 cases of nausea/vomiting, 3 cases of dizziness and 1 case of facial paralysis. No readmission was made as in the series of Singh
. These complications were treated with corticosteroids and antiemetics, and patients were able to go home within 6 hours of follow-up. In terms of satisfaction, all of our patients were satisfied with their care as in the case of hajjij
| [13] | Hajjij A, Elbouhmadi K, Gamali OE, Benjilali A, Benchikh S, Haoudar A, Anajar S, Taali L, Elkettani C, Snoussi K. Ambulatory pediatric cochlear implantation: safety, efficacy, and feasibility - first multicentric Moroccan study on 681 children. BMC Pediatr. 2025 Oct 6; 25(1): 774.
https://doi.org/10.1186/s12887-025-06169-4 |
[13]
. This is similar to the Khan M et al study with a satisfaction rate of 99.05%
.
5. Conclusion
When performed effectively with proper patient selection and meticulous surgical technique, outpatient otological surgery is a real step forward in patient care as it allows for an efficient use of resources and minimizes postoperative complications. As a result, it seems essential to have structures dedicated to outpatient surgery in order to develop this activity in complete safety. These dedicated units reassure the surgeon and increase patient satisfaction.
What is known about this topic
1) The advances in anesthesia and surgical techniques have led to the expansion of outpatient surgery in otology.
2) Overall reduction in the cost of otologic surgery
3) Decrease in the incidence of post-operative complications
What this study adds:
1) Transmeatal approach under anesthesia is a breakthrough for outpatient surgery.
2) Simultaneous bilateral myringoplasty under local anesthesia
3) Short operating time
4) Low readmission rate and post-operative complications.
Abbreviations
HU | University Hospital |
RHS | Reference Health Centre |
ORL-HNS | Otorhinolaryngology and Head and Neck Surgery |
ASA | American Society of Anesthesioloists |
Author Contributions
Kone Fatogoma Issa: Conceptualization, Investigation, Methodology, Project administration, Validation, Visualization, Writing – original draft, Writing – review & editing
Soumaoro Siaka: Conceptualization, Methodology, Validation, Visualization, Writing – review & editing
Ganaba Abdoulaye Modibo: Conceptualization, Investigation, Methodology, Project administration, Writing – original draft, Writing – review & editing
Dicko Ibrahim: Data curation
Haidara Abdoul Wahab: Data curation, Formal Analysis
Konate Oumar: Data curation, Formal Analysis
Toure Tata: Data curation, Formal Analysis
Aissata Ouane: Data curation, Formal Analysis
Assitan Kole Coulibaly: Data curation, Formal Analysis
Diarra Kassim: Formal Analysis
Neuilly Tafo: Software
Sidiki Dao: Data curation, Software
Konate N'faly: Software
Kalifa Coulibaly: Software
Sangare Mariam: Software
Ahmadou Dembélé: Software
Djibril Samake: Software
Traore Nouhoum: Resources, Software
Guindo Boubacary: Resources, Supervision
Singare Kadidiatou: Resources, Supervision
Keita Mohamed Amadou: Resources, Supervision, Validation
Funding
The authors state that they have not received specific funding for this work.
Conflicts of Interest
The authors declare that they have no conflict of interest in relation to this article.
References
| [1] |
Florian Roux. Evolution of the outpatient otologic surgery activity from 2010 to 2015. Doctoral thesis in medicine. Brest: University of Western Brittany, 2017.
|
| [2] |
A. Uziel. outpatient otological surgery. European Annals of Otorhinolaryngology and Head and Neck Diseases 134 (2017) 249–25:
http://dx.doi.org/10.1016/j.anorl.2016.11.008
|
| [3] |
P. Lemos et al. Patient satisfaction after outpatient surgery. Journal of Clinical Anesthesia (2009) 21, 200–205:
https://doi.org/10.1016/j.jclinane.2008.08.016
|
| [4] |
DS Lazard, F. Donne, JB Lecanu. Outpatient surgery in otology: impact study of a dedicated organizational model. European Annals of Otorhinolaryngology and Head and Neck Diseases 136 (2019) 465-468.
|
| [5] |
S. Bonnafousun, R. Hermannb, S. Zaoucheun, S. Tringaliun, M. Fieuxun. Evolution and safety of ambulatory surgery of the major ear. European Annals of Otorhinolaryngology and Head and Neck Diseases 138 (2021) 141–145.
|
| [6] |
Anesthetic management of patients in outpatient hospitalization. Ann Fr Anesth Reanim 2010; 29: 67–72.
|
| [7] |
Khan MM, Parab SR. Day care ear surgery: our experience of 4 years. Indian J Otolaryngol Head Neck Surg. 2012 Sep; 64(3): 280-4.
https://doi.org/10.1007/s12070-011-0303-x
|
| [8] |
R. D. Miller, "Miller's Anesthesia," sixth edition, Elsevier Churchill Livingstone, pp. 1227-1264, 2005.
|
| [9] |
Heilbronn, Cameron et al. Adult outpatient otological surgery: Unexpected revisits and complications. The laryngoscope,7(2020): 1788-1791.
https://doi.org/10.1002/lary.28346
|
| [10] |
Bawazeer N. Office-Based Middle Ear Surgery Under Local Anesthesia: A Contemporary Review. J Clin Med Res. 2025 Jul 31; 17(7): 365-374.
https://doi.org/10.14740/jocmr6279
|
| [11] |
Pézier T, Stimpson P, Kanegaonkar RG, Bowdler DA. Ear, nose and throat day-case surgery at a district general hospital. Ann R Coll Surg Engl. 2009 Mar; 91(2): 147-51.
https://doi.org/10.1308/003588409X359358
|
| [12] |
Singh VP, Kalra SP. Day Care Surgery in Otolaryngology: a three-year Prospective Study. Med J Armed Forces India. 2004 Jan; 60(1): 31-4.
https://doi.org/10.1016/S0377-1237(04)80154-0
|
| [13] |
Hajjij A, Elbouhmadi K, Gamali OE, Benjilali A, Benchikh S, Haoudar A, Anajar S, Taali L, Elkettani C, Snoussi K. Ambulatory pediatric cochlear implantation: safety, efficacy, and feasibility - first multicentric Moroccan study on 681 children. BMC Pediatr. 2025 Oct 6; 25(1): 774.
https://doi.org/10.1186/s12887-025-06169-4
|
Cite This Article
-
APA Style
Issa, K. F., Siaka, S., Modibo, G. A., Naouma, C., Ibrahim, D., et al. (2026). Evolution of the Outpatient Otologic Surgery Activity:
Our Experience. International Journal of Otorhinolaryngology, 12(1), 14-19. https://doi.org/10.11648/j.ijo.20261201.13
 Copy
|
Copy
|
 Download
Download
ACS Style
Issa, K. F.; Siaka, S.; Modibo, G. A.; Naouma, C.; Ibrahim, D., et al. Evolution of the Outpatient Otologic Surgery Activity:
Our Experience. Int. J. Otorhinolaryngol. 2026, 12(1), 14-19. doi: 10.11648/j.ijo.20261201.13
Copy
|
Download
AMA Style
Issa KF, Siaka S, Modibo GA, Naouma C, Ibrahim D, et al. Evolution of the Outpatient Otologic Surgery Activity:
Our Experience. Int J Otorhinolaryngol. 2026;12(1):14-19. doi: 10.11648/j.ijo.20261201.13
Copy
|
Download
-
@article{10.11648/j.ijo.20261201.13,
author = {Kone Fatogoma Issa and Soumaoro Siaka and Ganaba Abdoulaye Modibo and Cisse Naouma and Dicko Ibrahim and Haidara Abdoul Wahab and Konate Oumar and Toure Tata and Aissata Ouane and Assitan Kole Coulibaly and Diarra Kassim and Neuilly Tafo and Sidiki Dao and Konate N'faly and Kalifa Coulibaly and Sangare Mariam and Ahmadou Dembélé and Djibril Samake and Traore Nouhoum and Guindo Boubacary and Singare Kadidiatou and Keita Mohamed Amadou},
title = {Evolution of the Outpatient Otologic Surgery Activity:
Our Experience},
journal = {International Journal of Otorhinolaryngology},
volume = {12},
number = {1},
pages = {14-19},
doi = {10.11648/j.ijo.20261201.13},
url = {https://doi.org/10.11648/j.ijo.20261201.13},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ijo.20261201.13},
abstract = {Introduction: Otologic surgery is particularly suitable for outpatient surgery, which accounts for more than 50% of all surgeries performed in North America. Our aim was to report our experience to identify the benefits and limitations of outpatient otologic surgery in our context. Materials and methods: We conducted an observational, descriptive and retrospective study from January 2022 to December 2023, including 41 patients at the Gabriel Toure University Hospital in Bamako. We included cases of myringoplasty and antro-atticotomies. Results: The extreme ages of our patients are between 02 and 60 years old with an average of 29.5 years. Males accounted for 37.5% and 62.5% females. Myringoplasty affected the left and right sides in the same proportion (28.1%) and was bilateral in 14 cases (43.8%). As for antro-atticotomy, it concerned the right side in 06 cases and the left side in 03 cases. The average operating time was 30 minutes for myringoplasty and 50 minutes for antro-atticotomy. The main complications recorded were dizziness and vomiting in the immediate postoperative period and were encountered in 03 patients. All our patients were discharged the same day with a monitoring time of between 03 and 6 hours. No readmission has been carried out. Conclusion: when the selection criteria are met, outpatient otological surgery could be an essential element for an effective use of fairly limited resources in our context.},
year = {2026}
}
Copy
|
Download
-
TY - JOUR
T1 - Evolution of the Outpatient Otologic Surgery Activity:
Our Experience
AU - Kone Fatogoma Issa
AU - Soumaoro Siaka
AU - Ganaba Abdoulaye Modibo
AU - Cisse Naouma
AU - Dicko Ibrahim
AU - Haidara Abdoul Wahab
AU - Konate Oumar
AU - Toure Tata
AU - Aissata Ouane
AU - Assitan Kole Coulibaly
AU - Diarra Kassim
AU - Neuilly Tafo
AU - Sidiki Dao
AU - Konate N'faly
AU - Kalifa Coulibaly
AU - Sangare Mariam
AU - Ahmadou Dembélé
AU - Djibril Samake
AU - Traore Nouhoum
AU - Guindo Boubacary
AU - Singare Kadidiatou
AU - Keita Mohamed Amadou
Y1 - 2026/04/24
PY - 2026
N1 - https://doi.org/10.11648/j.ijo.20261201.13
DO - 10.11648/j.ijo.20261201.13
T2 - International Journal of Otorhinolaryngology
JF - International Journal of Otorhinolaryngology
JO - International Journal of Otorhinolaryngology
SP - 14
EP - 19
PB - Science Publishing Group
SN - 2472-2413
UR - https://doi.org/10.11648/j.ijo.20261201.13
AB - Introduction: Otologic surgery is particularly suitable for outpatient surgery, which accounts for more than 50% of all surgeries performed in North America. Our aim was to report our experience to identify the benefits and limitations of outpatient otologic surgery in our context. Materials and methods: We conducted an observational, descriptive and retrospective study from January 2022 to December 2023, including 41 patients at the Gabriel Toure University Hospital in Bamako. We included cases of myringoplasty and antro-atticotomies. Results: The extreme ages of our patients are between 02 and 60 years old with an average of 29.5 years. Males accounted for 37.5% and 62.5% females. Myringoplasty affected the left and right sides in the same proportion (28.1%) and was bilateral in 14 cases (43.8%). As for antro-atticotomy, it concerned the right side in 06 cases and the left side in 03 cases. The average operating time was 30 minutes for myringoplasty and 50 minutes for antro-atticotomy. The main complications recorded were dizziness and vomiting in the immediate postoperative period and were encountered in 03 patients. All our patients were discharged the same day with a monitoring time of between 03 and 6 hours. No readmission has been carried out. Conclusion: when the selection criteria are met, outpatient otological surgery could be an essential element for an effective use of fairly limited resources in our context.
VL - 12
IS - 1
ER -
Copy
|
Download