Abstract
Introduction: Multiple sclerosis (MS) can result in a range of disability, cognitive and ambulatory dysfunction, depression, fatigue, pain, and reduced quality of life. Hypertension has also been identified as a comorbidity for people living with MS. This case report investigated the impact of a six-week treadmill walking program combined with submaximal inspiratory exercise in a 39-year-old prehypertensive female living with MS. Case Description: The patient was referred for outpatient physical therapy to manage prehypertension and symptoms associated with MS. The patient completed a six-week treadmill walking program combined with submaximal inspiratory exercise. Outcomes included were systolic blood pressure (SBP), diastolic blood pressure (DBP), Numeric Pain Rating Scale (NPRS), Modified Fatigue Impact Scale (MFIS), and Lower Extremity Functional Scale (LEFS). Results: Following six weeks of intervention, the patient's resting SBP decreased from 128 mmHg to 122 mmHg and resting DBP decreased from 88 mmHg to 82 mmHg. The patient's fatigue level, measured with MFIS, improved from 57/84 to 35/84. LEFS increased from 26/80 to 39/80 with improvements in balance, walking, and stair-climbing activities. Discussion: A six-week treadmill walking program combined with submaximal inspiratory exercise effectively lowered resting blood pressure and MS-related symptoms, improving the patient's quality of life and functional capabilities.
Keywords
Multiple Sclerosis, Hypertension, Submaximal Inspiratory Exercise, Treadmill Walking
1. Introduction
1.1. Background
Multiple Sclerosis (MS) is an inflammatory autoimmune disorder that affects the central nervous system, with approximately 2.3 million people affected globally
| [1] | Browne P, Chandraratna D, Angood C, Tremlett H, Baker C, Taylor BV, et al. Atlas of multiple sclerosis 2013: A growing global problem with widespread inequity. Neurol. 2014; 83(11): 1022–1024. https://doi.org/10.1212/WNL.0000000000000768 |
[1]
. It can result in cognitive impairment, depression, fatigue, reduced quality of life, pain, mobility impairment, and disability
. MS can also lead to physiological deconditioning, including lower aerobic power and reduced exercise tolerance
| [3] | Klaren RE, Sandroff BM, Fernhall B, et al. Comprehensive profile of cardiopulmonary exercise testing in ambulatory persons with multiple sclerosis. Sports Med. 2016; 46(9): 1365-1379. https://doi.org/10.1007/s40279-016-0472-6 |
[3]
.
According to Lapierre et al.
| [4] | Lapierre Y, Hum S. Treating fatigue. Int MS J. 2007; 14(2): 64-71. |
[4]
,
fatigue is a prevalent symptom in people with MS, with 78 - 90% of individuals experiencing MS related fatigue. It is also the most disabling symptom in 28 - 40% of these individuals. Additionally, 40% of those who experienced fatigue reported experiencing it daily for over 30 days
| [4] | Lapierre Y, Hum S. Treating fatigue. Int MS J. 2007; 14(2): 64-71. |
[4]
.
While the exact cause of MS is unknown, it is widely accepted that it involves an aberrant immunological reaction in the central nervous system. The uneven distribution of demyelination (loss of myelin, which is a protective sheath around nerves) throughout the central nervous system can result in problems related to muscle strength and endurance, including those affecting the respiratory muscles
| [5] | Fry DK, Pfalzer LA, Chokshi AR, Wagner MT, Jackson ES. Randomized control trial of effects of a 10-week inspiratory muscle training program on measures of pulmonary function in persons with multiple sclerosis. Journal of Neurological Physical Therapy. 2007; 31(4): 162-172. https://doi.org/10.1097/NPT.0b013e31815ce136 |
| [6] | Smeltzer SC, Utell MJ, Rudick RA, Herndon RM. Pulmonary function and dysfunction in multiple sclerosis. Archives of Neurology. 1988; 45(11): 1245-1249. https://doi.org/10.1001/archneur.1988.00520350083020 |
[5, 6]
. MS is often linked to reduced physical activity, causing a decline in aerobic capacity, muscle strength, and balance, creating a cycle of inactivity
| [7] | Motl RW, Goldman MD, Benedict RH. Walking impairment in patients with multiple sclerosis: Exercise training as a treatment option. Neuropsychiatric Disease and Treatment. 2010; 6: 767–774. https://doi.org/10.2147/NDT.S10480 |
[7]
.
Hypertension is a comorbid condition that is prevalent among patients with MS
| [8] | Marrie RA, Yu BN, Leung S, et al. Rising prevalence of vascular comorbidities in multiple sclerosis: Validation of administrative definitions for diabetes, hypertension, and hyperlipidemia. Mult Scler. 2012; 18: 1310-1319. https://doi.org/10.1177/1352458512437814 |
[8]
. Hypertension is the third most common comorbidity in patients with MS
| [9] | Motl RW, Bollaert R. Sedentary behavior in persons with multiple sclerosis: Is the time ripe for targeting a new health behavior? Kinesiol Rev. 2022; 81: 63-69. https://doi.org/10.1123/kr.2018-0056 |
[9]
, affecting 17.1% to 30.1% of patients with MS in North America
| [9] | Motl RW, Bollaert R. Sedentary behavior in persons with multiple sclerosis: Is the time ripe for targeting a new health behavior? Kinesiol Rev. 2022; 81: 63-69. https://doi.org/10.1123/kr.2018-0056 |
[9]
. Pulse pressure, which is the difference between systolic and diastolic pressures, has been associated with ambulatory functioning in patients with MS
. It is evident from the literature that hypertension is a problematic condition for individuals living with MS
.
Recent research has demonstrated that regular exercise can have primary benefits such as improved balance and increased walking capacity
. Regular exercise reduces fatigue, enhances mood, improves quality of life, and decreases perceived disability; with these benefits having been observed immediately following an 8-week strength-training program
| [12] | Cakt BD, Nacir B, Genc H, et al. Cycling progressive resistance training for people with multiple sclerosis: A randomized controlled study. Am J Phys Med Rehabil. 2010; 89: 446–457. https://doi.org/10.1097/PHM.0b013e3181d3e71f |
[12]
and aerobic exercise intervention
| [13] | Rampello A, Franceschini M, Piepoli M, et al. Effect of aerobic training on walking capacity and maximal exercise tolerance in patients with multiple sclerosis: A randomized crossover-controlled study. Phys Ther. 2007; 87: 545–555. https://doi.org/10.2522/ptj.20060085 |
| [14] | Castellano V, Patel DI, White LJ. Cytokine responses to acute and chronic exercise in multiple sclerosis. J Appl Physiol. 2008; 104: 1697–1702. https://doi.org/10.1152/japplphysiol.00954.2007 |
[13, 14]
.
Aerobic treadmill training can improve walking ability, fitness, and quality of life due to the high volume of task-specific practice it provides
| [15] | Devasahayam AJ, Downer MB, Ploughman M. The effects of aerobic exercise on the recovery of walking ability and neuroplasticity in people with multiple sclerosis: A systematic review of animal and clinical studies. Mult Scler Int. 2017: 2017: 4815958. https://doi.org/10.1155/2017/4815958 |
| [16] | Schulz KH, Gold SM, Witte J, Bartsch K, Lang UE, Hellweg R, et al. Impact of aerobic training on immune-endocrine parameters, neurotrophic factors, quality of life and coordinative function in multiple sclerosis. J Neurol Sci. 2004; 225(1–2): 11–18. https://doi.org/10.1016/j.jns.2004.06.009 |
| [17] | Ploughman M. A new era of multiple sclerosis rehabilitation: Lessons from stroke. Lancet Neurol. 2017; 16(10): 768–769. https://doi.org/10.1016/S1474-4422(17)30301-0 |
[15-17]
.
Respiratory muscle training (RMT) strengthens the respiratory muscles by adding a significant load
| [18] | Ghannadi S, Noormohammadpour P, Mazaheri R, et al. Effect of eight weeks respiratory muscle training on respiratory capacity, functional capacity, and quality of life on subjects with mild to moderate relapsing-remitting multiple sclerosis: A single-blinded randomized controlled trial. Mult Scler Relat Disord. 2022; 68: 104208. https://doi.org/10.1016/j.msard.2022.104208 |
[18]
. Several recent studies have investigated the effects of inspiratory muscle training (IMT) in individuals with asthma, chronic obstructive pulmonary disease (COPD), bronchiectasis, acute stroke, MS, and airflow limitation
| [18] | Ghannadi S, Noormohammadpour P, Mazaheri R, et al. Effect of eight weeks respiratory muscle training on respiratory capacity, functional capacity, and quality of life on subjects with mild to moderate relapsing-remitting multiple sclerosis: A single-blinded randomized controlled trial. Mult Scler Relat Disord. 2022; 68: 104208. https://doi.org/10.1016/j.msard.2022.104208 |
| [19] | Ray AD, Udhoji S, Mashtare TL, Fisher NM. A combined inspiratory and expiratory muscle training program improves respiratory muscle strength and fatigue in multiple sclerosis. Arch Phys Med Rehabil. 2013; 94(10): 1964–1970. https://doi.org/10.1016/j.apmr.2013.05.005 |
| [20] | Gosselink R, Kovacs L, Ketelaer P, Carton H, Decramer M. Respiratory muscle weakness and respiratory muscle training in severely disabled multiple sclerosis patients. Arch Phys Med Rehabil. 2000; 81(6): 747–751. https://doi.org/10.1016/s0003-9993(00)90105-9 |
| [21] | Smeltzer SC, Lavietes MH, Cook SD. Expiratory training in multiple sclerosis. Arch Phys Med Rehabil. 1996; 77(9): 909–912. https://doi.org/10.1016/s0003-9993(96)90281-6 |
[18-21]
.
A recent pre-post trial revealed that a five-week inspiratory and expiratory muscle training program increased muscle strength and decreased fatigue in patients with mild to moderate MS
| [19] | Ray AD, Udhoji S, Mashtare TL, Fisher NM. A combined inspiratory and expiratory muscle training program improves respiratory muscle strength and fatigue in multiple sclerosis. Arch Phys Med Rehabil. 2013; 94(10): 1964–1970. https://doi.org/10.1016/j.apmr.2013.05.005 |
[19]
. Only two randomized trials have been conducted to assess expiratory muscle strength training in severely disabled patients with MS
.
Numerous studies have examined the effects of aerobic exercises, such as treadmill training, and respiratory muscle exercises in patients with MS
| [2] | Motl RW, Pilutti LA. The benefits of exercise training in multiple sclerosis. Nat Rev Neurol. 2012; 8(9): 487-497. https://doi.org/10.1038/nrneurol.2012.136 |
| [4] | Lapierre Y, Hum S. Treating fatigue. Int MS J. 2007; 14(2): 64-71. |
| [5] | Fry DK, Pfalzer LA, Chokshi AR, Wagner MT, Jackson ES. Randomized control trial of effects of a 10-week inspiratory muscle training program on measures of pulmonary function in persons with multiple sclerosis. Journal of Neurological Physical Therapy. 2007; 31(4): 162-172. https://doi.org/10.1097/NPT.0b013e31815ce136 |
| [7] | Motl RW, Goldman MD, Benedict RH. Walking impairment in patients with multiple sclerosis: Exercise training as a treatment option. Neuropsychiatric Disease and Treatment. 2010; 6: 767–774. https://doi.org/10.2147/NDT.S10480 |
| [12] | Cakt BD, Nacir B, Genc H, et al. Cycling progressive resistance training for people with multiple sclerosis: A randomized controlled study. Am J Phys Med Rehabil. 2010; 89: 446–457. https://doi.org/10.1097/PHM.0b013e3181d3e71f |
| [13] | Rampello A, Franceschini M, Piepoli M, et al. Effect of aerobic training on walking capacity and maximal exercise tolerance in patients with multiple sclerosis: A randomized crossover-controlled study. Phys Ther. 2007; 87: 545–555. https://doi.org/10.2522/ptj.20060085 |
| [14] | Castellano V, Patel DI, White LJ. Cytokine responses to acute and chronic exercise in multiple sclerosis. J Appl Physiol. 2008; 104: 1697–1702. https://doi.org/10.1152/japplphysiol.00954.2007 |
| [15] | Devasahayam AJ, Downer MB, Ploughman M. The effects of aerobic exercise on the recovery of walking ability and neuroplasticity in people with multiple sclerosis: A systematic review of animal and clinical studies. Mult Scler Int. 2017: 2017: 4815958. https://doi.org/10.1155/2017/4815958 |
| [16] | Schulz KH, Gold SM, Witte J, Bartsch K, Lang UE, Hellweg R, et al. Impact of aerobic training on immune-endocrine parameters, neurotrophic factors, quality of life and coordinative function in multiple sclerosis. J Neurol Sci. 2004; 225(1–2): 11–18. https://doi.org/10.1016/j.jns.2004.06.009 |
| [17] | Ploughman M. A new era of multiple sclerosis rehabilitation: Lessons from stroke. Lancet Neurol. 2017; 16(10): 768–769. https://doi.org/10.1016/S1474-4422(17)30301-0 |
| [18] | Ghannadi S, Noormohammadpour P, Mazaheri R, et al. Effect of eight weeks respiratory muscle training on respiratory capacity, functional capacity, and quality of life on subjects with mild to moderate relapsing-remitting multiple sclerosis: A single-blinded randomized controlled trial. Mult Scler Relat Disord. 2022; 68: 104208. https://doi.org/10.1016/j.msard.2022.104208 |
| [19] | Ray AD, Udhoji S, Mashtare TL, Fisher NM. A combined inspiratory and expiratory muscle training program improves respiratory muscle strength and fatigue in multiple sclerosis. Arch Phys Med Rehabil. 2013; 94(10): 1964–1970. https://doi.org/10.1016/j.apmr.2013.05.005 |
| [20] | Gosselink R, Kovacs L, Ketelaer P, Carton H, Decramer M. Respiratory muscle weakness and respiratory muscle training in severely disabled multiple sclerosis patients. Arch Phys Med Rehabil. 2000; 81(6): 747–751. https://doi.org/10.1016/s0003-9993(00)90105-9 |
| [21] | Smeltzer SC, Lavietes MH, Cook SD. Expiratory training in multiple sclerosis. Arch Phys Med Rehabil. 1996; 77(9): 909–912. https://doi.org/10.1016/s0003-9993(96)90281-6 |
[2, 4, 5, 7, 12-21]
. However, there is limited research on the combined effects of the combination of interventions in persons living with MS who also have prehypertension. This case report investigated the impact of a six-week treadmill walking program combined with submaximal inspiratory exercise in a 39-year-old female with prehypertension and MS.
1.2. Clinical Question
Can a six-week treadmill walking program combined with submaximal inspiratory exercise effectively manage prehypertension in a 39-year-old female living with MS? Additionally, what are the effects of these interventions on pain level, fatigue level, and level of functional activities involving both lower extremities and symptoms related to MS?
2. Case Description
2.1. Patient History and Systems Review
This case report pertained to a 39-year-old African American female who was employed as a secretary and was diagnosed with relapsing-remitting multiple sclerosis (RRMS) three years prior to the plan of care established in this case report. The patient's medical history was marked by neurological symptoms associated with repeated exacerbations of RRMS, including pain, muscle weakness, numbness, and visual disturbances. The patient was on 0.25 mg of Betaseron (self-administered every two to three days), 200 mg of Celebrex (taken once a day), 75 mg of Pregabalin (taken twice a day), 10 mg of Atorvastatin, 1000 mg of Acetaminophen (taken as needed), and Vitamin A.
The patient reported moderate fatigue, reduced lower extremity functional abilities, and occasional pain, particularly during physical activities. Four months before outpatient physical therapy referral, she experienced worsening MS symptoms, including pain in unspecified areas of both thighs and weakness in the left leg. The only significant symptom observed was fatigue.
She consulted her doctor approximately eight weeks before referral to outpatient physical therapy. A repeat magnetic resonance imaging test was requested, and the radiological report revealed further distal demyelination within the brain tissues and plaque formation in the corpus callosum, a band of nerve tissues connecting the cerebral hemispheres. Although the patient did not report any changes in clinical symptoms based on the last radiological findings, a thorough clinical history revealed a gradual progression of MS-related symptoms over the past two years. The patient had experienced at least two episodes of relapse and remissions prior to the most recent one that occurred four months ago, with varying degrees of neurological impairments during relapse episodes, which were followed by partial or complete recovery during remission periods.
The functional limitations observed included minimal balance constraints impacting ambulation, reduced gait velocity, and decreased gross muscle power in the lower extremities. The patient stated that she occasionally experienced fatigue, forcing her to take seated rest breaks for extended periods, which caused limitations in her activities of daily living (ADLs). She also reported tripping episodes when climbing stairs when fatigued.
The patient's medical history also indicated the presence of comorbidities, including, prehypertension and dyslipidemia. The patient was taking 10 mg of Atorvastatin to manage dyslipidemia and was given a physical therapy referral for exercise to control resting blood pressure in addition to MS-related symptoms. As a precautionary measure to prevent hypotension or syncope that could lead to falls, the doctor recommended physical therapy instead of antihypertensive medication(s).
The patient lived with her husband, worked full-time, and took care of herself with minimal to no assistance and no need for ambulatory aid. She stopped driving six months after her initial diagnosis of RRMS but enjoyed dog walking, especially in the evening, and with good lighting, she enjoyed reading.
As part of the assessment, a thorough examination was conducted to evaluate the patient's overall health condition and to detect any impairment related to her medical condition. The mean resting systolic blood pressure (SBP) was 128 mmHg and, the mean resting diastolic blood pressure (DBP) was 88 mmHg. No other significant anomalies were observed in the cardiovascular, respiratory, or gastrointestinal systems. There was no significant abnormality in the musculoskeletal system except for pain with varying intensity and frequency, which she sometimes described as a stabbing, burning, or tingling sensation in the back and lower extremities, specifically in the thigh and calf muscles.
From a neurological perspective, the patient exhibited motor deficits, leading to diminished coordination, muscle weakness in the upper and lower extremities, and minimal difficulty with balance and gait. She had normal muscle tone in both upper and lower extremities. However, she demonstrated reduced muscle strength in bilateral lower extremities (LEs), with gross manual muscle testing (MMT) graded as 4/5 in the right LE and 4-/5 in the left LE.
She experienced higher levels of fatigue from noon to 3 pm on most days, leading to difficulties in engaging in daily activities, mood changes, body pain, weakness, and reduced quality of life. She also reported experiencing cognitive difficulties that affected her ability to process information quickly and remember things. The patient's main goal in seeking physical therapy was to maintain her blood pressure at a normal level, as recommended by her doctor. She also wanted to improve her ability to walk longer distances on both even and uneven surfaces with minimal fatigue and pain and enhance her functional activities, particularly with her lower limbs, by increasing her gross muscle strength.
2.2. Clinical Impression I - Examination
Following an initial examination, the patient presented with a range of symptoms, including general body pain, weakness, and fatigue, which are commonly associated with MS. The patient's blood pressure reading fell within the prehypertension range
| [22] | Chobanian AV, Bakris GL, Black HR. et al. The seventh report of the Joint National Committee on prevention, detection, evaluation, and treatment of high blood pressure. The JNC-7 Report. JAMA. 2003; 289(19): 2560–2572. https://doi.org/10.1001/jama.289.19.2560 |
[22]
. Reduced muscle strength was observed throughout the body with attention to the LEs. These findings suggested that reduced muscle power, particularly in the lower limbs, resulted in impaired mobility and gait. The patient showed mild-to-moderate coordination and proprioception impairments but was able to ambulate with minimal balance problems. Cognitive impairments were present, including attention difficulties, forgetfulness, multitasking issues, and mood changes, which affected quality of life. The patient was ideal for this case report because of her motivation and enthusiasm for full participation in physical therapy, independent functioning, and eagerness to increase productivity at her job.
2.3. Tests and Measures
The manual sphygmomanometer is a popular tool for measuring SBP and DBP. This case report used an aneroid manometer with a handheld dial for SBP and DBP measurements. The aneroid manometer has a sensitivity of 86.7% and a specificity of 98.7%
| [23] | Shahbabu B, Dasgupta A, Sarkar K, Sahoo SK. Which is more accurate in measuring the blood pressure? A digital or an aneroid sphygmomanometer. J Clin Diagn Res. 2016; 10(3): LC11-LC14. https://doi.org/10.7860/JCDR/2016/14351.7458 |
[23]
. The SBP was subtracted from DBP to determine the pulse pressure.
The NPRS, or Numeric Pain Rating Scale, was used to evaluate the patient's pain level. It consists of a 0 – 10 scale where the patient rated her pain, with 10 indicating the most severe possible pain requiring hospitalization and 0 indicating no pain. The NPRS has good test-retest reliability in individuals with chronic pain, with a correlation coefficient of 0.79 – 0.96
| [24] | Ferraz MB, Quaresma MR, Aquino LR, et al. Reliability of pain scales in the assessment of literate and illiterate patients with rheumatoid arthritis. J Rheumatol. 1990; 17(8): 1022–1024. |
| [25] | Hawker GA, Mian S, Kendzerska T, et al. Measures of adult pain: Visual analog scale for pain, numeric rating scale for pain, McGill pain questionnaire, short-form McGill pain questionnaire, chronic pain grade scale, short-form-36 bodily pain scale, and measure of intermittent and constant osteoarthritis pain. Arthritis Care. 2011; 63(11): S240–252. https://doi.org/10.1002/acr.20543 |
| [26] | Downie WW, Leatham PA, Rhind VM, et al. Studies with pain rating scales. Ann Rheum Dis. 1978; 37(4): 378–381. https://doi.org/10.1136/ard.37.4.378 |
| [27] | Marques AP, Assumpcao A, Matsutani LA, et al. Pain in fibromyalgia and discrimination power of the instruments: Visual analog scale, dolorimetry, and the McGill pain questionnaire. Acta Reumatol Port. 2008; 33(3): 345–351. |
| [28] | Jensen MP, McFarland CA. Increasing the reliability and validity of pain intensity measurement in chronic pain patients. Pain. 1993; 55(2): 195–203. https://doi.org/10.1016/0304-3959(93)90148-I |
[24-28]
. The NPRS has also been correlated with the verbal rating scale (VRS) and visual analog scale (VAS), confirming its construct validity
.
The LEFS, or Lower Extremity Functional Scale, is a self-reported 20-item questionnaire used to evaluate a patient's ability to perform daily functional tasks and functions of the LEs. The test-retest reliability of the LEFS was excellent, R = 0.94 (95% lower limit, CI = 0.89)
| [30] | Binkley JM, Stratford PW, Lott SA, Riddle DL. The Lower Extremity Functional Scale (LEFS): Scale development, measurement properties, and clinical application. North American Orthopaedic Rehabilitation Research Network. Phys Ther. 1999; 79(4): 371-383. https://doi.org/10.1093/ptj/79.4.371 |
[30]
, and construct validity was supported by comparison with the SF-36
| [30] | Binkley JM, Stratford PW, Lott SA, Riddle DL. The Lower Extremity Functional Scale (LEFS): Scale development, measurement properties, and clinical application. North American Orthopaedic Rehabilitation Research Network. Phys Ther. 1999; 79(4): 371-383. https://doi.org/10.1093/ptj/79.4.371 |
[30]
.
The Modified Fatigue Impact Scale, MFIS, was used to evaluate the impact of fatigue on the patient's daily life. It is a 21-item questionnaire, with a total score ranging from 0 to 84. The items on the MFIS address the impact of fatigue on the patient's physical, cognitive, and psychosocial well-being. The MFIS possesses good structural, cross-cultural, and nomological validity and is suitable for multidimensional Rasch analysis
| [31] | Morten R, Philipp T, Michael N, Finn B. Multimethodological validation of the modified fatigue impact scale in a Danish population of people with multiple sclerosis. Multiple Sclerosis and Related Disorders. 2022; 65: https://doi.org/10.1016/j.msard.2022.104012 |
[31]
.
All outcome measurements were taken at the initial assessment and the end of the 6th week of the intervention.
2.4. Clinical Impression II - Observations
Based on the initial examination findings and clinical impression, the patient in this case report was ideal for skilled physical therapy care. After conducting an initial assessment and examination of the patient, the following observations were made regarding her condition: the patient was diagnosed with relapsing-remitting MS and prehypertension as a comorbidity that was not being managed with medication. The patient's progressive symptoms and functional limitations required targeted interventions to promote overall well-being, including physical, cognitive, and psychosocial health. The patient's muscle weakness, reduced muscle power in both lower extremities, general body pain, proprioception, coordination impairments, and balance issues affected her mobility and functional independence. Additionally, cognitive impairment and mood changes further contributed to her functional limitations. Physical therapy interventions aimed to control the patient's blood pressure, address pain and weakness, and ultimately enhance the patient's physical functions, cognitive abilities, and overall well-being.
3. Interventions
A six-week treadmill walking program combined with submaximal inspiratory exercise was implemented for the patient to improve blood pressure, decrease general body pain, and decrease mobility limitations. These interventions aimed to promote functional independence, reduce physical and cognitive fatigue levels, and improve psychosocial well-being, ultimately improving the patient's overall quality of life. The patient participated in conventional exercises, treadmill walking, and submaximal inspiratory exercises using a manual incentive spirometer. The interventions were tailored to the patient's level of comfort and pain.
Procedural Interventions
A combination of procedural checklists, verbal instructions, demonstrations, and pictorial charts ensured that the patient understood the treatments. The mean blood pressure base readings, pulse pressure, pain level using the NPRS, LEFS, and MFIS were recorded at initial evaluation and at the end of the 6th week.
The following steps were taken during each treatment session during the six-week intervention period:
3.1. Warm-up Period
The patient was instructed to inhale deeply through the nostrils and exhale through pursed lips for 10 repetitions. The soft tissues of both the upper and lower extremities were mobilized. Finally, the patient completed the warm-up period with stretching exercises for the back, upper, and lower extremities. The warm-up period was performed three times a week for six weeks, lasting 10 minutes per session.
3.2. Conventional Exercises
Following the warm-up, the patient underwent a 15-minute bout of conventional exercise three times a week, including joint mobility activities, eccentric contractions, and muscle-strengthening exercises for the upper and lower extremities. The patient completed a series of exercises involving isometric contractions in the joints of the upper and lower extremities using a weight of 1.5 pounds for 3 sets of 10 repetitions. Additionally, the patient performed straight leg raises for bilateral lower extremities and bridging for 3 sets of 10 repetitions each. The patient performed 3 sets of 10 repetitions of 3 for assisted-active range of motion exercises for both hips, knees, and ankles, followed by a brief rest. The patient repeated the exercises at each session, three times a week for six weeks.
3.3. Treadmill Walking
This study used a Cardios Pro treadmill with a maximum load of 200 kg, a speed range of 0 – 12 mph at 60 Hz, and a power rating of 2.2 KW. Following a brief rest period, the patient participated in treadmill walking at a comfortable pace for 10 minutes per session three times a week on alternate days from Monday to Friday, totaling 18 sessions over the intervention period of six weeks. The treadmill speed was set at 2.5 mph in the first week and increased by 0.2 mph each week, such that the speed in the 6th week of intervention was 3.5 mph, as depicted in
Table 1.
3.4. Submaximal Inspiratory Exercise
Submaximal inspiratory exercise was completed using a manual incentive spirometer that offered visual feedback to help the patient take deep breaths and fully expand the lungs. The patient was instructed to perform 5 sets of 6 breaths at least twice daily, 6 days per week, for six weeks. The patient was given a detailed explanation of how to use the incentive spirometer, and one was provided for her to take home to continue the exercise. Weekly progress monitoring sessions were scheduled for six weeks to provide guidance, motivation, and support throughout the intervention and address any concerns. The patient was instructed to inhale deeply through the mouthpiece of the spirometer, such that the balls in the first and second compartments rose to the maximum, but the ball in the third compartment was just at the mid-level of the device. The patient was instructed to hold the breath for 3 seconds and progressed to 5 seconds from the 3rd week of intervention to the 6th week, as shown in
Table 1. The patient was then told to breathe slowly through pursed lips until the lungs were empty, allowing the chest and shoulder muscles to relax. The patient was told to take a 1-minute rest period between sets. A home exercise log was used to track exercise compliance, recording the frequency of exercise, and any reported issues.
Table 1. Summary of the interventions over six weeks.
Week # | Warm-up period (10mins) | Conventional exercises (15mins) | Treadmill walking (10mins) | Submaximal inspiratory exercise (5 sets of 6 breaths) | Cool-down period (10mins) |
1 | ✔ (3x weekly) | ✔ (3x weekly) | 2.5 mph (3x weekly) | hold breath for 3s (≥ 2x,6d weekly) | ✔ (3x weekly) |
2 | ✔ (3x weekly) | ✔ (3x weekly) | 2.7 mph (3x weekly) | hold breath for 3s (≥ 2x,6d weekly) | ✔ (3x weekly) |
3 | ✔ (3x weekly) | ✔ (3x weekly) | 2.9 mph (3x weekly) | hold breath for 5s (≥ 2x,6d weekly) | ✔ (3x weekly) |
4 | ✔ (3x weekly) | ✔ (3x weekly) | 3.1 mph (3x weekly) | hold breath for 5s (≥ 2x,6d weekly) | ✔ (3x weekly) |
5 | ✔ (3x weekly) | ✔ (3x weekly) | 3.3 mph (3x weekly) | hold breath for 5s (≥ 2x,6d weekly) | ✔ (3x weekly) |
6 | ✔ (3x weekly) | ✔ (3x weekly) | 3.5 mph (3x weekly) | hold breath for 5s (≥ 2x,6d weekly) | ✔ (3x weekly) |
Key
✔ - Completed; x – Number of times interventions occurred; mins – Minutes
s – Seconds; mph – miles per hour; # - Week number; d - Day
3.5. Cool-down Period
Finally, the patient was instructed to inhale deeply through the nostrils and exhale slowly through pursed lips for 10 repetitions to enhance relaxation. Subsequently, stretches were performed on the quadriceps, hamstrings, and calf muscles to alleviate tension in the lower extremities. Finally, the cool-down period included stretching exercises to the arms, neck, upper back, and shoulders to relax the major muscle groups of the body. The cool-down was performed three times a week for six weeks, lasting 10 minutes per session.
4. Results
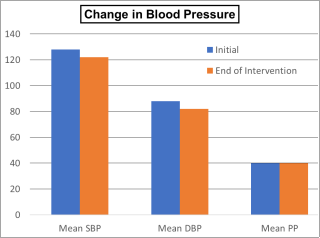
At the end of the episode of care, the patient demonstrated improvements in all outcome measures. The mean blood pressure readings for resting SBP and DBP were 122 mmHg and 82 mmHg, respectively. These readings were based on the mean value of three measurements
| [32] | Viitanem JV, Kautiainen H, Suni J. The relative value of spinal and thoracic mobility measurement in ankylosing spondylitis. Scandinavian Journal of Rheumatology. 1995; 24: 94-97. https://doi.org/10.3109/03009749509099291 |
[32]
and represented an improvement from the previous mean values of resting SBP at 128 mmHg and resting DBP at 88 mmHg, shown in
Figure 1. However, pulse pressure did not show significant changes. The patient's pain score decreased from 7 at worst to 4 at present, 3 at best, and 5 at worst on the NPRS shown in
Table 2.
Figure 1. The systolic, diastolic, and pulse pressure changes over six-week interventions.
Rooney et al.
| [33] | Rooney S, McFadyen A, Wood L, Moffat F, Paul L. Minimally important difference of the fatigue severity scale and modified fatigue impact scale in people with multiple sclerosis. Multiple Sclerosis and Related Disorders. 2019; 35: 158-163. https://doi.org/10.1016/j.msard.2019.07.028 |
[33]
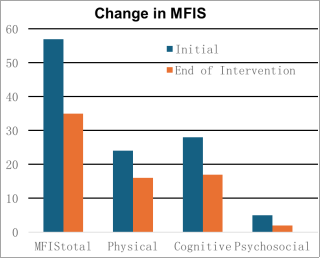
estimated that a difference of 4 points in the MFIS score is a clinically significant difference in fatigue for people living with MS. The total MFIS score improved from 57/84 at the initial examination to 35/84 at the end of the intervention in this case study. Improvement in the MFIS score was evident in the physical, cognitive, and psychosocial subscales, shown in
Figure 2.
A systematic review by Mehta et al.
| [34] | Mehta SP, Fulton A, Quach C, Thistle M, Toledo C, Evans NA. Measurement properties of the lower extremity functional scale: A systematic review. Journal of Orthopaedic & Sports Physical Therapy. 2016; 46(3): 200-216. https://doi.org/10.2519/jospt.2016.6165 |
[34]
validated the use of LEFS across a wide range of lower extremity diagnoses. They found that the pooled estimate of the minimal detectable change at a 90% confidence level (MDC
90) was 6 points and the minimal clinically important difference (MCID) was 9 points. In this study, the LEFS score increased from 26/80 (32.5%) to 39/80 (48.8%), indicating an improvement in the patient's physical activity level, as observed in her walking, balancing, and stair climbing. Improvements in the MFIS and LEFS suggested enhanced functional abilities, especially in the LEs
| [30] | Binkley JM, Stratford PW, Lott SA, Riddle DL. The Lower Extremity Functional Scale (LEFS): Scale development, measurement properties, and clinical application. North American Orthopaedic Rehabilitation Research Network. Phys Ther. 1999; 79(4): 371-383. https://doi.org/10.1093/ptj/79.4.371 |
[30]
, and improved quality of life for the patient
| [30] | Binkley JM, Stratford PW, Lott SA, Riddle DL. The Lower Extremity Functional Scale (LEFS): Scale development, measurement properties, and clinical application. North American Orthopaedic Rehabilitation Research Network. Phys Ther. 1999; 79(4): 371-383. https://doi.org/10.1093/ptj/79.4.371 |
| [31] | Morten R, Philipp T, Michael N, Finn B. Multimethodological validation of the modified fatigue impact scale in a Danish population of people with multiple sclerosis. Multiple Sclerosis and Related Disorders. 2022; 65: https://doi.org/10.1016/j.msard.2022.104012 |
[30, 31]
.
The improvements observed in the patient's resting SBP and DBP, reduced pain level, enhanced functionality of her lower extremities, and reduced fatigue levels translated into improved blood pressure and increased ability to function independently. These improvements were evident in the patient's ability to walk on even and uneven surfaces with minimal fatigue, increased concentration, attentiveness, and other cognitive and psychosocial abilities, as reported by the patient, leading to a better quality of life at the end of the six weeks of intervention.
Figure 2. The Modified Fatigue Impact Scale (MFIS) Total, Physical, Cognitive, and Psychosocial Subscales Change Over Six-week Interventions.
Table 2. Summary of results at the initial examination (baseline) and week 6.
Outcome Measures | Baseline Reading (Initial Examination) | End of Intervention Reading (Week 6) |
BP Reading | First | Second | Third | Mean | First | Second | Third | Mean |
SBP (mmHg) | 128 | 128 | 128 | ≈ 128 | 122 | 123 | 122 | ≈ 122 |
DBP (mmHg) | 88 | 89 | 87 | ≈ 88 | 82 | 83 | 82 | ≈ 82 |
PP (mmHg) | 40 | 39 | 41 | ≈ 40 | 40 | 40 | 40 | 40 |
NPRS | 6 at present; 5 at best; 7 at worst | 4 at present, 3 at best, and 5 at worst |
MFIS (total) | 57/84 | 35/84 |
Physical | 24/36 | 16/36 |
Cognitive | 28/40 | 17/40 |
Psychosocial | 5/8 | 2/8 |
LEFS | 26/80 (32.5%) | 39/80 (48.8%) |
Key
BP – Blood pressure; SBP – Systolic blood pressure; DBP – Diastolic blood pressure
PP – Pulse pressure; NPRS – Numeric pain rating scale; MFIS - Modified fatigue impact scale
LEFS - Lower extremity functional scale; mmHg - Millimeters of mercury
5. Discussion
This case report investigated the impact of a six-week treadmill walking program combined with submaximal inspiratory exercise in a 39-year-old prehypertensive female living with MS. The study also examined the effects of these interventions on pain, fatigue, and functional levels, specifically in both lower extremities. The peculiarity of the patient's presentation necessitated a thorough clinical examination, encompassing both subjective and objective assessments, to fully comprehend the patient's medical history, functional abilities, and expectations before the interventions were implemented
. The patient demonstrated significant improvements in fatigue, lower extremity function, pain, and cardiovascular parameters for blood pressure. These findings align with previous research that underscores the effectiveness of exercise-based interventions and respiratory therapy in managing MS-associated symptoms
| [18] | Ghannadi S, Noormohammadpour P, Mazaheri R, et al. Effect of eight weeks respiratory muscle training on respiratory capacity, functional capacity, and quality of life on subjects with mild to moderate relapsing-remitting multiple sclerosis: A single-blinded randomized controlled trial. Mult Scler Relat Disord. 2022; 68: 104208. https://doi.org/10.1016/j.msard.2022.104208 |
| [19] | Ray AD, Udhoji S, Mashtare TL, Fisher NM. A combined inspiratory and expiratory muscle training program improves respiratory muscle strength and fatigue in multiple sclerosis. Arch Phys Med Rehabil. 2013; 94(10): 1964–1970. https://doi.org/10.1016/j.apmr.2013.05.005 |
| [36] | Gervasoni E, Cattaneo D, Jonsdottir J. Effect of treadmill training on fatigue in multiple sclerosis: a pilot study. Int J Rehabil Res. 2014; 37(1): 54-60. https://doi.org/10.1097/MRR.0000000000000034 |
[18, 19, 36]
. Supervised low-to-moderate intensity exercise programs effectively improve cardiovascular fitness, mood, and quality of life in people living with MS who have an expanded disability status scale of less than 7 (EDSS < 7) in just four weeks
. The patient's fatigue level improved, as seen in the physical, cognitive, and psychosocial subscales of the MFIS, from 57/84 to 35/84. This improvement could be explained by changes resulting from the interventions, such as reduced long-term inactivity, increased neuroprotection, and neuroplasticity
.
According to a study by Harvard Medical School, aerobic exercise can reduce average blood pressure by 7.1 points for SBP and 5.1 points for DBP
. Rabi et al.
| [41] | Rabi DM, McBrien KA, Sapir-Pichhadze R, et al. Hypertension Canada's 2020 comprehensive guidelines for the prevention, diagnosis, risk assessment, and treatment of hypertension in adults and children. Can J Cardiol. 2020; 36(5): 596-624. https://doi.org/10.1016/j.cjca.2020.02.086 |
[41]
also stated that walking and jogging can lower blood pressure and improve MS-related symptoms. The patient's blood pressure decreased from 128 mmHg to 122 mmHg and from 88 mmHg to 82 mmHg for SBP and DBP, respectively. A study by Fry et al.
| [5] | Fry DK, Pfalzer LA, Chokshi AR, Wagner MT, Jackson ES. Randomized control trial of effects of a 10-week inspiratory muscle training program on measures of pulmonary function in persons with multiple sclerosis. Journal of Neurological Physical Therapy. 2007; 31(4): 162-172. https://doi.org/10.1097/NPT.0b013e31815ce136 |
[5]
suggested that improved blood pressure in patients living with MS may be due to enhanced autonomic nervous system regulation.
The patient's pain level also decreased following a six-week treadmill walking program combined with submaximal inspiratory exercise. The patient's improvement in pain level may be attributed to physical therapy interventions that triggered the release of the body's natural painkiller, endorphins
.
The patient showed a significant improvement in the ability to use the lower extremities, as seen in the performance of physical activities, such as balancing, walking, and climbing stairs. The LEFS increased from 26/80 to 39/80 after the six-week intervention, confirming this improvement. A study by Braendvik et al.
| [43] | Braendvik SM, Koret T, Helbostad JL, et al. Treadmill training or progressive strength training to improve walking in people with multiple sclerosis? A randomized parallel-group trial. Physiother Res Int. 2016; 21(4): 228-236. https://doi.org/10.1002/pri.1636 |
[43]
showed that task-specific training via treadmill walking is a better approach than progressive strength training to improve lower extremity function in persons with mild and moderate MS, consistent with the improvement in the patients' walking abilities. In a study by Rampello et al.
| [13] | Rampello A, Franceschini M, Piepoli M, et al. Effect of aerobic training on walking capacity and maximal exercise tolerance in patients with multiple sclerosis: A randomized crossover-controlled study. Phys Ther. 2007; 87: 545–555. https://doi.org/10.2522/ptj.20060085 |
[13]
, structured aerobic exercise programs that affect the cardiovascular and respiratory systems were more effective than certain neurological interventions focused on improving respiratory-postural and respiratory-motor synergies in patients living with MS.
6. Conclusions and Future Research
The findings of this case report indicated that a six-week treadmill walking program combined with submaximal inspiratory exercise can significantly reduce the adverse effects of MS and improve the patient's quality of life and functional capabilities. Improvements in cardiovascular fitness, respiratory function, autonomic regulation, and neuromuscular coordination are just a few of the distinct mechanisms that each intervention possesses, which can be responsible for the observed improvements
| [18] | Ghannadi S, Noormohammadpour P, Mazaheri R, et al. Effect of eight weeks respiratory muscle training on respiratory capacity, functional capacity, and quality of life on subjects with mild to moderate relapsing-remitting multiple sclerosis: A single-blinded randomized controlled trial. Mult Scler Relat Disord. 2022; 68: 104208. https://doi.org/10.1016/j.msard.2022.104208 |
| [36] | Gervasoni E, Cattaneo D, Jonsdottir J. Effect of treadmill training on fatigue in multiple sclerosis: a pilot study. Int J Rehabil Res. 2014; 37(1): 54-60. https://doi.org/10.1097/MRR.0000000000000034 |
[18, 36]
. Some positive factors may have contributed to the improvement in functional outcomes, including the patient's motivation to increase productivity at work, compliance level, and eagerness to improve independent functioning. A six-week treadmill walking program combined with submaximal inspiratory exercise significantly improved patient outcomes.
Further research should focus on whether the effects of these interventions are sustained in patients with similar presentations after treatment termination and, if so, for how long. Future research should also endeavor to conduct larger-scale studies to validate the findings of this case report and to explore additional intervention approaches in prehypertensive patients of similar age groups living with MS.
Abbreviations
MS: Multiple Sclerosis
DBP: Diastolic Blood Pressure
SBP: Systolic Blood Pressure
MFIS: Modified Fatigue Impact Scale
NPRS: Numeric Pain Rating Scale
LEFS: Lower Extremity Functional Scale
Author Contributions
Abiodun Akanbi Adeogun: Conceptualization, Data curation, Formal Analysis, Investigation, Methodology, Project administration, Resources, Validation, Visualization, Writing – original draft, Writing – review & editing
Jade Bender-Burnett: Formal Analysis, Visualization, Writing – review & editing
Conflicts of Interest
The authors declare no conflicts of interest.
References
| [1] |
Browne P, Chandraratna D, Angood C, Tremlett H, Baker C, Taylor BV, et al. Atlas of multiple sclerosis 2013: A growing global problem with widespread inequity. Neurol. 2014; 83(11): 1022–1024.
https://doi.org/10.1212/WNL.0000000000000768
|
| [2] |
Motl RW, Pilutti LA. The benefits of exercise training in multiple sclerosis. Nat Rev Neurol. 2012; 8(9): 487-497.
https://doi.org/10.1038/nrneurol.2012.136
|
| [3] |
Klaren RE, Sandroff BM, Fernhall B, et al. Comprehensive profile of cardiopulmonary exercise testing in ambulatory persons with multiple sclerosis. Sports Med. 2016; 46(9): 1365-1379.
https://doi.org/10.1007/s40279-016-0472-6
|
| [4] |
Lapierre Y, Hum S. Treating fatigue. Int MS J. 2007; 14(2): 64-71.
|
| [5] |
Fry DK, Pfalzer LA, Chokshi AR, Wagner MT, Jackson ES. Randomized control trial of effects of a 10-week inspiratory muscle training program on measures of pulmonary function in persons with multiple sclerosis. Journal of Neurological Physical Therapy. 2007; 31(4): 162-172.
https://doi.org/10.1097/NPT.0b013e31815ce136
|
| [6] |
Smeltzer SC, Utell MJ, Rudick RA, Herndon RM. Pulmonary function and dysfunction in multiple sclerosis. Archives of Neurology. 1988; 45(11): 1245-1249.
https://doi.org/10.1001/archneur.1988.00520350083020
|
| [7] |
Motl RW, Goldman MD, Benedict RH. Walking impairment in patients with multiple sclerosis: Exercise training as a treatment option. Neuropsychiatric Disease and Treatment. 2010; 6: 767–774.
https://doi.org/10.2147/NDT.S10480
|
| [8] |
Marrie RA, Yu BN, Leung S, et al. Rising prevalence of vascular comorbidities in multiple sclerosis: Validation of administrative definitions for diabetes, hypertension, and hyperlipidemia. Mult Scler. 2012; 18: 1310-1319.
https://doi.org/10.1177/1352458512437814
|
| [9] |
Motl RW, Bollaert R. Sedentary behavior in persons with multiple sclerosis: Is the time ripe for targeting a new health behavior? Kinesiol Rev. 2022; 81: 63-69.
https://doi.org/10.1123/kr.2018-0056
|
| [10] |
Heffernan KS, Ranadive S, Weikert M, et al. Pulse pressure is associated with walking impairment in multiple sclerosis. J Neurol Sci. 2011; 309: 105-109.
https://doi.org/10.1016/j.jns.2011.07.004
|
| [11] |
Hubbard EA, Motl RW, Fernhall B. Sedentary behavior and blood pressure in patients with multiple sclerosis. Int J MS Care. 2018; 20: 1-8.
https://doi.org/10.7224/1537-2073.2016-021
|
| [12] |
Cakt BD, Nacir B, Genc H, et al. Cycling progressive resistance training for people with multiple sclerosis: A randomized controlled study. Am J Phys Med Rehabil. 2010; 89: 446–457.
https://doi.org/10.1097/PHM.0b013e3181d3e71f
|
| [13] |
Rampello A, Franceschini M, Piepoli M, et al. Effect of aerobic training on walking capacity and maximal exercise tolerance in patients with multiple sclerosis: A randomized crossover-controlled study. Phys Ther. 2007; 87: 545–555.
https://doi.org/10.2522/ptj.20060085
|
| [14] |
Castellano V, Patel DI, White LJ. Cytokine responses to acute and chronic exercise in multiple sclerosis. J Appl Physiol. 2008; 104: 1697–1702.
https://doi.org/10.1152/japplphysiol.00954.2007
|
| [15] |
Devasahayam AJ, Downer MB, Ploughman M. The effects of aerobic exercise on the recovery of walking ability and neuroplasticity in people with multiple sclerosis: A systematic review of animal and clinical studies. Mult Scler Int. 2017: 2017: 4815958.
https://doi.org/10.1155/2017/4815958
|
| [16] |
Schulz KH, Gold SM, Witte J, Bartsch K, Lang UE, Hellweg R, et al. Impact of aerobic training on immune-endocrine parameters, neurotrophic factors, quality of life and coordinative function in multiple sclerosis. J Neurol Sci. 2004; 225(1–2): 11–18.
https://doi.org/10.1016/j.jns.2004.06.009
|
| [17] |
Ploughman M. A new era of multiple sclerosis rehabilitation: Lessons from stroke. Lancet Neurol. 2017; 16(10): 768–769.
https://doi.org/10.1016/S1474-4422(17)30301-0
|
| [18] |
Ghannadi S, Noormohammadpour P, Mazaheri R, et al. Effect of eight weeks respiratory muscle training on respiratory capacity, functional capacity, and quality of life on subjects with mild to moderate relapsing-remitting multiple sclerosis: A single-blinded randomized controlled trial. Mult Scler Relat Disord. 2022; 68: 104208.
https://doi.org/10.1016/j.msard.2022.104208
|
| [19] |
Ray AD, Udhoji S, Mashtare TL, Fisher NM. A combined inspiratory and expiratory muscle training program improves respiratory muscle strength and fatigue in multiple sclerosis. Arch Phys Med Rehabil. 2013; 94(10): 1964–1970.
https://doi.org/10.1016/j.apmr.2013.05.005
|
| [20] |
Gosselink R, Kovacs L, Ketelaer P, Carton H, Decramer M. Respiratory muscle weakness and respiratory muscle training in severely disabled multiple sclerosis patients. Arch Phys Med Rehabil. 2000; 81(6): 747–751.
https://doi.org/10.1016/s0003-9993(00)90105-9
|
| [21] |
Smeltzer SC, Lavietes MH, Cook SD. Expiratory training in multiple sclerosis. Arch Phys Med Rehabil. 1996; 77(9): 909–912.
https://doi.org/10.1016/s0003-9993(96)90281-6
|
| [22] |
Chobanian AV, Bakris GL, Black HR. et al. The seventh report of the Joint National Committee on prevention, detection, evaluation, and treatment of high blood pressure. The JNC-7 Report. JAMA. 2003; 289(19): 2560–2572.
https://doi.org/10.1001/jama.289.19.2560
|
| [23] |
Shahbabu B, Dasgupta A, Sarkar K, Sahoo SK. Which is more accurate in measuring the blood pressure? A digital or an aneroid sphygmomanometer. J Clin Diagn Res. 2016; 10(3): LC11-LC14.
https://doi.org/10.7860/JCDR/2016/14351.7458
|
| [24] |
Ferraz MB, Quaresma MR, Aquino LR, et al. Reliability of pain scales in the assessment of literate and illiterate patients with rheumatoid arthritis. J Rheumatol. 1990; 17(8): 1022–1024.
|
| [25] |
Hawker GA, Mian S, Kendzerska T, et al. Measures of adult pain: Visual analog scale for pain, numeric rating scale for pain, McGill pain questionnaire, short-form McGill pain questionnaire, chronic pain grade scale, short-form-36 bodily pain scale, and measure of intermittent and constant osteoarthritis pain. Arthritis Care. 2011; 63(11): S240–252.
https://doi.org/10.1002/acr.20543
|
| [26] |
Downie WW, Leatham PA, Rhind VM, et al. Studies with pain rating scales. Ann Rheum Dis. 1978; 37(4): 378–381.
https://doi.org/10.1136/ard.37.4.378
|
| [27] |
Marques AP, Assumpcao A, Matsutani LA, et al. Pain in fibromyalgia and discrimination power of the instruments: Visual analog scale, dolorimetry, and the McGill pain questionnaire. Acta Reumatol Port. 2008; 33(3): 345–351.
|
| [28] |
Jensen MP, McFarland CA. Increasing the reliability and validity of pain intensity measurement in chronic pain patients. Pain. 1993; 55(2): 195–203.
https://doi.org/10.1016/0304-3959(93)90148-I
|
| [29] |
Hrvatin I, Puh U. Measurement properties of the numerical pain rating scale in patients with musculoskeletal impairments of the limbs – A systematic literature review. Zdrav Vestn. 2021; 90(9–10): 512–520.
https://doi.org/https://doi.org/10.6016/ZdravVestn.3108
|
| [30] |
Binkley JM, Stratford PW, Lott SA, Riddle DL. The Lower Extremity Functional Scale (LEFS): Scale development, measurement properties, and clinical application. North American Orthopaedic Rehabilitation Research Network. Phys Ther. 1999; 79(4): 371-383.
https://doi.org/10.1093/ptj/79.4.371
|
| [31] |
Morten R, Philipp T, Michael N, Finn B. Multimethodological validation of the modified fatigue impact scale in a Danish population of people with multiple sclerosis. Multiple Sclerosis and Related Disorders. 2022; 65:
https://doi.org/10.1016/j.msard.2022.104012
|
| [32] |
Viitanem JV, Kautiainen H, Suni J. The relative value of spinal and thoracic mobility measurement in ankylosing spondylitis. Scandinavian Journal of Rheumatology. 1995; 24: 94-97.
https://doi.org/10.3109/03009749509099291
|
| [33] |
Rooney S, McFadyen A, Wood L, Moffat F, Paul L. Minimally important difference of the fatigue severity scale and modified fatigue impact scale in people with multiple sclerosis. Multiple Sclerosis and Related Disorders. 2019; 35: 158-163.
https://doi.org/10.1016/j.msard.2019.07.028
|
| [34] |
Mehta SP, Fulton A, Quach C, Thistle M, Toledo C, Evans NA. Measurement properties of the lower extremity functional scale: A systematic review. Journal of Orthopaedic & Sports Physical Therapy. 2016; 46(3): 200-216.
https://doi.org/10.2519/jospt.2016.6165
|
| [35] |
Burks JS, Bigley GK, Hill HH. Rehabilitation challenges in multiple sclerosis. Ann Indian Acad Neurol. 2009; 12(4): 296-306.
https://doi.org/10.4103/0972-2327.58273
|
| [36] |
Gervasoni E, Cattaneo D, Jonsdottir J. Effect of treadmill training on fatigue in multiple sclerosis: a pilot study. Int J Rehabil Res. 2014; 37(1): 54-60.
https://doi.org/10.1097/MRR.0000000000000034
|
| [37] |
White LJ, Dressendorfer RH. Exercise and multiple sclerosis. Sports Med. 2004; 34(15): 1077–1100.
https://doi.org/10.2165/00007256-200434150-00005
|
| [38] |
Mostert S, Kesselring J. Effects of a short-term exercise training program on aerobic fitness, fatigue, health perception and activity level of subjects with multiple sclerosis. Multiple Sclerosis. 2002; 8(2): 161–168.
https://doi.org/10.1191/1352458502ms779oa
|
| [39] |
Heine M, van de Port I, Rietberg MB, van Wegen EE, Kwakkel G. Exercise therapy for fatigue in multiple sclerosis. Cochrane Database Syst Rev. 2015; 11(9): CD009956.
https://doi.org/10.1002/14651858.CD009956.pub2
|
| [40] |
Julie C. Aerobic exercise helps hard-to-treat high blood pressure. November 1, 2021. Accessed February 29, 2024.
https://www.health.harvard.edu/heart-health/aerobic-exercise-helps-hard-to-treat-high-blood-pressure
|
| [41] |
Rabi DM, McBrien KA, Sapir-Pichhadze R, et al. Hypertension Canada's 2020 comprehensive guidelines for the prevention, diagnosis, risk assessment, and treatment of hypertension in adults and children. Can J Cardiol. 2020; 36(5): 596-624.
https://doi.org/10.1016/j.cjca.2020.02.086
|
| [42] |
Endorphins: The brain's natural pain reliever. Harvard Medical School. Updated July 20, 2021. Accessed February 29, 2024.
https://www.health.harvard.edu/mind-and-mood/endorphins-the-brains-natural-pain-reliever
|
| [43] |
Braendvik SM, Koret T, Helbostad JL, et al. Treadmill training or progressive strength training to improve walking in people with multiple sclerosis? A randomized parallel-group trial. Physiother Res Int. 2016; 21(4): 228-236.
https://doi.org/10.1002/pri.1636
|
Cite This Article
-
APA Style
Adeogun, A. A., Bender-Burnett, J. (2024). Impact of a Six-Week Treadmill Walking Program Combined with Submaximal Inspiratory Exercise in a Prehypertensive Female Living with Multiple Sclerosis: A Case Report. International Journal of Neurologic Physical Therapy, 10(1), 16-24. https://doi.org/10.11648/j.ijnpt.20241001.13
 Copy
|
Copy
|
 Download
Download
ACS Style
Adeogun, A. A.; Bender-Burnett, J. Impact of a Six-Week Treadmill Walking Program Combined with Submaximal Inspiratory Exercise in a Prehypertensive Female Living with Multiple Sclerosis: A Case Report. Int. J. Neurol. Phys. Ther. 2024, 10(1), 16-24. doi: 10.11648/j.ijnpt.20241001.13
Copy
|
Download
AMA Style
Adeogun AA, Bender-Burnett J. Impact of a Six-Week Treadmill Walking Program Combined with Submaximal Inspiratory Exercise in a Prehypertensive Female Living with Multiple Sclerosis: A Case Report. Int J Neurol Phys Ther. 2024;10(1):16-24. doi: 10.11648/j.ijnpt.20241001.13
Copy
|
Download
-
@article{10.11648/j.ijnpt.20241001.13,
author = {Abiodun Akanbi Adeogun and Jade Bender-Burnett},
title = {Impact of a Six-Week Treadmill Walking Program Combined with Submaximal Inspiratory Exercise in a Prehypertensive Female Living with Multiple Sclerosis: A Case Report
},
journal = {International Journal of Neurologic Physical Therapy},
volume = {10},
number = {1},
pages = {16-24},
doi = {10.11648/j.ijnpt.20241001.13},
url = {https://doi.org/10.11648/j.ijnpt.20241001.13},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ijnpt.20241001.13},
abstract = {Introduction: Multiple sclerosis (MS) can result in a range of disability, cognitive and ambulatory dysfunction, depression, fatigue, pain, and reduced quality of life. Hypertension has also been identified as a comorbidity for people living with MS. This case report investigated the impact of a six-week treadmill walking program combined with submaximal inspiratory exercise in a 39-year-old prehypertensive female living with MS. Case Description: The patient was referred for outpatient physical therapy to manage prehypertension and symptoms associated with MS. The patient completed a six-week treadmill walking program combined with submaximal inspiratory exercise. Outcomes included were systolic blood pressure (SBP), diastolic blood pressure (DBP), Numeric Pain Rating Scale (NPRS), Modified Fatigue Impact Scale (MFIS), and Lower Extremity Functional Scale (LEFS). Results: Following six weeks of intervention, the patient's resting SBP decreased from 128 mmHg to 122 mmHg and resting DBP decreased from 88 mmHg to 82 mmHg. The patient's fatigue level, measured with MFIS, improved from 57/84 to 35/84. LEFS increased from 26/80 to 39/80 with improvements in balance, walking, and stair-climbing activities. Discussion: A six-week treadmill walking program combined with submaximal inspiratory exercise effectively lowered resting blood pressure and MS-related symptoms, improving the patient's quality of life and functional capabilities.
},
year = {2024}
}
Copy
|
Download
-
TY - JOUR
T1 - Impact of a Six-Week Treadmill Walking Program Combined with Submaximal Inspiratory Exercise in a Prehypertensive Female Living with Multiple Sclerosis: A Case Report
AU - Abiodun Akanbi Adeogun
AU - Jade Bender-Burnett
Y1 - 2024/05/10
PY - 2024
N1 - https://doi.org/10.11648/j.ijnpt.20241001.13
DO - 10.11648/j.ijnpt.20241001.13
T2 - International Journal of Neurologic Physical Therapy
JF - International Journal of Neurologic Physical Therapy
JO - International Journal of Neurologic Physical Therapy
SP - 16
EP - 24
PB - Science Publishing Group
SN - 2575-1778
UR - https://doi.org/10.11648/j.ijnpt.20241001.13
AB - Introduction: Multiple sclerosis (MS) can result in a range of disability, cognitive and ambulatory dysfunction, depression, fatigue, pain, and reduced quality of life. Hypertension has also been identified as a comorbidity for people living with MS. This case report investigated the impact of a six-week treadmill walking program combined with submaximal inspiratory exercise in a 39-year-old prehypertensive female living with MS. Case Description: The patient was referred for outpatient physical therapy to manage prehypertension and symptoms associated with MS. The patient completed a six-week treadmill walking program combined with submaximal inspiratory exercise. Outcomes included were systolic blood pressure (SBP), diastolic blood pressure (DBP), Numeric Pain Rating Scale (NPRS), Modified Fatigue Impact Scale (MFIS), and Lower Extremity Functional Scale (LEFS). Results: Following six weeks of intervention, the patient's resting SBP decreased from 128 mmHg to 122 mmHg and resting DBP decreased from 88 mmHg to 82 mmHg. The patient's fatigue level, measured with MFIS, improved from 57/84 to 35/84. LEFS increased from 26/80 to 39/80 with improvements in balance, walking, and stair-climbing activities. Discussion: A six-week treadmill walking program combined with submaximal inspiratory exercise effectively lowered resting blood pressure and MS-related symptoms, improving the patient's quality of life and functional capabilities.
VL - 10
IS - 1
ER -
Copy
|
Download