Introduction: The goal of this study was to determine the contribution of Magnetic Resonance Imaging (MRI) in the etiological diagnosis of slow spinal cord compressions. Methods: This was a prospective descriptive study conducted over a period of six months, from August 16, 2023, to February 16, 2024. Results: During the study period, 1082 MRI scans were performed, of which 68 cases (6.28%) were diagnosed with slow spinal cord compressions. The mean age of patients was 51.85 ± 18.87 years, ranging from 3 to 92 years. Males accounted for 72.1% (n = 49), with a sex ratio of 2.57. Most patients were referred by the neurology department (67.6%). The average time to MRI examination after clinical consultation was 2 ± 0.71 days. The most common presenting symptoms were spinal pain and motor disturbances, noted in 70.6% of cases. The cervical and thoracic spinal levels were the most frequently affected, each accounting for more than 41.2% (n = 28) of cases. Extradural lesions were predominant, observed in 83.8% of cases. Degenerative pathologies were the most common cause (44.1%), followed by tumoral lesions (42.6%). Cervicoarthrosic myelopathy was the most frequent radiologic diagnosis, accounting for 33.9% of cases. Conclusion: Slow spinal cord compression is a recurrent spinal cord pathology affecting individuals of all ages, with a male predominance. The extradural compartment is most frequently involved, primarily due to degenerative conditions, especially cervical spondylotic myelopathy. Tumoral lesions, primarly metastatic, represent the second most frequent etiology.
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited.
Slow spinal cord compressions (SSCC) are common spinal cord pathologies caused by expansive lesions resulting from mechanical and/or vascular processes
[1]
Dagbe M, N’timon B, Gbande P, Yaye I, Ntankeu -Tankoua P P, Kolou B et al. The MRI contribution in etiological diagnosis of the slow medullary compression in Lomé: about 72 cases. J Afr Imag Méd 2022; 14(4): 275-280.
[1]
.”
They represent a diagnostic and therapeutic emergency requiring early management to prevent irreversible complications, such as myelomalacia
[2]
Cherif Idrissi El Ganouni N, Khalil MR, Hiroual MR, El Idrissi I, Haddi M, Aït Benali S, et al. Contribution of MRI in slow spinal cord compressions of tumoral and infectious origin. Feuillets de Radiologie. 2009; 49(4): 251–262.
[3]
Ayoun AR. Spinal Cord Compression. Faculty of Medicine of Oran. Neurology Module, 4th Year Medical Studies.
[2, 3]
.
Spinal pain is the most frequent clinical symptom of spinal cord compression, occurring in almost 90% of cases
[4]
Amjoud M. Contibution of MRI to non-traumatic spinal cord compression [Doctoral thesis in Medicine]. Marrakech: Faculty of Medicine and Pharmacy of Marrakech.; N 017/2023; 154 p.
[4]
.
Their etiologies are diverse and classified into 3 groups: intramedullary lesions (rare), extramedullary intradural lesions and extradural lesions.
[5]
Ndao AC, Faye A, Diagne N, Dia AD, Dia DG, Kane BS, et al. Etiological profile of slow spinal cord compressions in Internal Medicine. RAFMI 2021; 8(1): 25-30.
[6]
New PW, Cripps RA, Bonne Lee B. Global maps of non-traumatic spinal cord injury epidemiology: towards a living data repository. Spinal Cord 2014; 52(2): 97–109.
[5, 6]
.
In developed countries, malignant etiologies (tumors) predominate over benign ones
[1]
Dagbe M, N’timon B, Gbande P, Yaye I, Ntankeu -Tankoua P P, Kolou B et al. The MRI contribution in etiological diagnosis of the slow medullary compression in Lomé: about 72 cases. J Afr Imag Méd 2022; 14(4): 275-280.
[1]
.
Slow Spinal Cord Compressions (SSCCs) are frequently occurring spinal cord pathologies caused by expansive lesions resulting from mechanical and/or vascular processes
[1]
Dagbe M, N’timon B, Gbande P, Yaye I, Ntankeu -Tankoua P P, Kolou B et al. The MRI contribution in etiological diagnosis of the slow medullary compression in Lomé: about 72 cases. J Afr Imag Méd 2022; 14(4): 275-280.
[1]
.
They represent both a diagnostic and therapeutic emergency, requiring early management to prevent irreversible complications such as myelomalacia
[2]
Cherif Idrissi El Ganouni N, Khalil MR, Hiroual MR, El Idrissi I, Haddi M, Aït Benali S, et al. Contribution of MRI in slow spinal cord compressions of tumoral and infectious origin. Feuillets de Radiologie. 2009; 49(4): 251–262.
[3]
Ayoun AR. Spinal Cord Compression. Faculty of Medicine of Oran. Neurology Module, 4th Year Medical Studies.
[2, 3]
.
Spinal pain is the most common clinical symptom of spinal cord compression, observed in nearly 90% of cases
[4]
Amjoud M. Contibution of MRI to non-traumatic spinal cord compression [Doctoral thesis in Medicine]. Marrakech: Faculty of Medicine and Pharmacy of Marrakech.; N 017/2023; 154 p.
[4]
. The etiologies are diverse and can be classified into three groups: intramedullary lesions (rare), intradural extramedullary lesions, and extradural lesions
[5]
Ndao AC, Faye A, Diagne N, Dia AD, Dia DG, Kane BS, et al. Etiological profile of slow spinal cord compressions in Internal Medicine. RAFMI 2021; 8(1): 25-30.
[6]
New PW, Cripps RA, Bonne Lee B. Global maps of non-traumatic spinal cord injury epidemiology: towards a living data repository. Spinal Cord 2014; 52(2): 97–109.
[5, 6]
. In developed countries, malignant (tumorous) causes are more prevalent than benign ones
[1]
Dagbe M, N’timon B, Gbande P, Yaye I, Ntankeu -Tankoua P P, Kolou B et al. The MRI contribution in etiological diagnosis of the slow medullary compression in Lomé: about 72 cases. J Afr Imag Méd 2022; 14(4): 275-280.
[1]
.
Degenerative spinal diseases account for 59% of non-traumatic spinal cord lesions in Japan, 54% in the United States, 31% in Europe, 22% in Australia, and between 4% and 30% in Africa
[7]
Kassegne I, Sakiye K, Kanassoua K, Beketi AK, Seydou Badiane B, Koffi Balogou AA. Management of spinal cord compression in Togo. Med Sante Trop 2013; 23: 206-210.
[7]
. There appear to be regional specificities in Africa, with a predominance of tuberculous etiology, although some African studies report a higher prevalence of metastatic spinal causes
[1]
Dagbe M, N’timon B, Gbande P, Yaye I, Ntankeu -Tankoua P P, Kolou B et al. The MRI contribution in etiological diagnosis of the slow medullary compression in Lomé: about 72 cases. J Afr Imag Méd 2022; 14(4): 275-280.
[1]
. Pott’s disease remains prevalent in sub-Saharan Africa, much more so than in North Africa. In Côte d’Ivoire, its frequency was considerable, reaching 52%
[1]
Dagbe M, N’timon B, Gbande P, Yaye I, Ntankeu -Tankoua P P, Kolou B et al. The MRI contribution in etiological diagnosis of the slow medullary compression in Lomé: about 72 cases. J Afr Imag Méd 2022; 14(4): 275-280.
[1]
. In Togo, Kassegne I et al. (2013) reported that 27% of SSCC cases were managed in their study
[8]
Camara MA, N’Diaye M, Coulibaly MB, Traore MM, Diarra H, Toure BM et al. MRI Contribution in the Diagnosis of Non-Traumatic Medular Compressions at the Mali Hospital of about 179 Cases. Open Journal of Medical Imaging. 2020; 10: 186-195.
[8]
. Magnetic resonance imaging (MRI) has undoubtedly simplified the diagnosis and treatment planning, and is now the gold standard in the management of SSCC
[1]
Dagbe M, N’timon B, Gbande P, Yaye I, Ntankeu -Tankoua P P, Kolou B et al. The MRI contribution in etiological diagnosis of the slow medullary compression in Lomé: about 72 cases. J Afr Imag Méd 2022; 14(4): 275-280.
[9]
Fadiga SI. MRI features of infectious spondylodiscitis in the medical imaging department of Mali Hospital: a series of 152 cases [DES Radiology and Medical Imaging Thesis]. Mali: Faculty of Medicine and Odonto-Stomatology 2022. 106 p.
[1, 9]
. The increasing demand for spinal MRI in cases of slow spinal cord compression, along with the lack of prior studies on this subject in our clinical setting, motivated this study. Its general objective was to determine the etiological profile of slow spinal cord compressions on MRI in our context. More specifically, the study aimed to determine the frequency of MRI performed for SSCC, rank MRI diagnostic hypotheses by frequency, identify the most common lesions by spinal segment, and determine the time delay between medical prescription and MRI completion.
2. Methods
This was a prospective descriptive study conducted over a period of six months, from August 16, 2023, to February 16, 2024 at the CNSS Diagnostic Center in Conakry. Our study included all vertebro-medullary MRI examinations of patients admitted to the department for slow spinal cord compression, in which the MRI protocol was followed and the results were interpreted and validated by a radiologist.
Only the MRI reports confirming the presence of Slow Spinal Cord Compression were included in the analysis.
Excluded were incomplete or non-interpretable examinations (due to artifacts), as well as follow-up MRIs or those performed for already diagnosed and treated conditions.
Our Data collection was based on MRI examination reports and registers. The information were collected using a pre-established data collection form.
We conducted an exhaustive recruitment of all MRI results that met our inclusion criteria. The variables studied included sociodemographic data (age, sex), the time interval between prescription and MRI completion, and the underlying causes of spinal cord compression.
For the examinations we used a 1.5 Tesla TOSHIBA Vantage Elan MRI scanner, which has been operational since 2019.
For all patients, we performed the basic sequences: T1- and T2-weighted sagittal Time Spin Echo (TSE), axial T2 TSE centred on the pathological spinal segments, and sagittal T2 STIR (Short Time Inversion Recovry).
Additional complementary sequences were performed as required by each case, including T1 TSE fat-saturated post-contrast (Fat sat + Gadolinium), T2 (T2-weighted sequence with rapid signal decay), myelographic MRI sequences, and diffusion-weighted imaging (DWI). Data analysis was carried out using SPSS software, version 22.0. The information obtained was used solely for scientific purposes, with the free and informed consent of all participants, and confidentiality was strictly maintained.
3. Results
During our study, 68 cases of SSCC were identified among 1,082 MRI examinations performed in our department, representing a frequency of 6.3%.
Males were the most represented, at 72.1%, with a sex ratio of 2.6 Male/Female (M/F).
The 60-69 age group was the most represented (25%), with an average age of 51.85 +/- 18.87 years and extremes of 3 and 92 years.
The majority of our patients were referred from the neurology department (67.6%), followed by the neurosurgery department (27.9%).
The time interval between the consultation and the MRI ranged from 24 to 72 hours in 50% of our patients, with a mean time of 2 ± 0.71 days.
The reasons for consultation were spinal pain (70.6%), motor deficits (70.6%), radicular pain (33.8%), sphincter disorders (19.1%), and sensory deficits (14.7%). These symptoms were categorized into three main syndromes: spinal syndrome (70.6%, n=48), lesion syndrome (33.8%, n=23), and sublesional syndrome (72.1%, n=49).
Spinal cord compression was located in the cervical region (41.2%), thoracic region (41.2%), lumbar region (5.9%), cervicothoracic junction (7.3%), thoracolumbar junction (2.9%), and involved multiple levels (1.5%). The types of lesions encountered included degenerative processes (44.1%), tumor processes (42.6%), and infectious processes (13.2%).
The extraforaminal compartment was the most frequently affected (83.8%), followed by the intraforaminal extramedullary (8.8%) and intramedullary compartments (7.4%). Regarding contrast administration, 51.5% (n=35) of patients received gadolinium injection, while 48.5% (n=33) did not.
Cervical spondylotic myelopathy was the most frequently suggested radiological diagnosis in our series (33.9%) (Table 1).
Table 1. Distribution of Etiologies of Slow Spinal Cord Compressions According to Radiological Diagnosis.
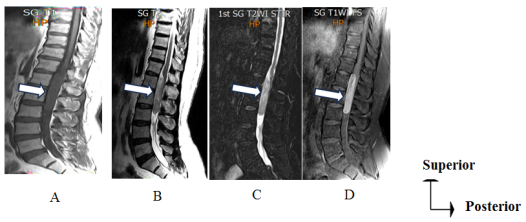
Figure 1. Sagittal T1 (A), T2 (B), T2 STIR (C), and post-contrast T1 fat-sat (D) sequences demonstrating an intraspinal extramedullary mass in contact with the anterior meningeal spaces. The lesion exhibits intense contrast enhancement and exerts significant mass effect on the conus medullaris, suggestive of meningioma.
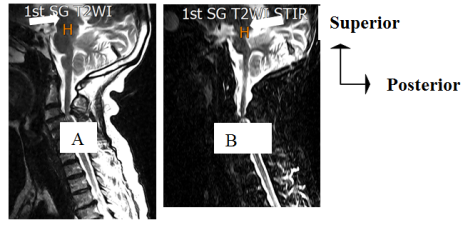
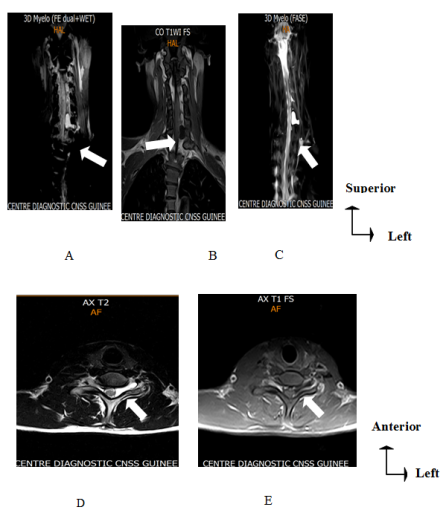
Figure 2. Cervical spine MRI, sagittal T2-weighted TSE (A) and T2 STIR (B) sequences: Multilevel disc-osteophytic protrusion from C3-C4 to C6-C7, associated with advanced hypertrophic zygapophyseal osteoarthritis at C3-C4, causing severe central spinal canal stenosis. Corresponding T2 hyperintensity within the spinal cord is noted, consistent with cervical spondylotic myelopathy.
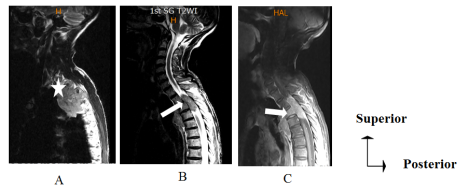
Figure 3. Sagittal T2 TSE (A), T2 TSE (B), and T2 STIR (C) post-contrast sequences revealed a pulmonary lesion suspicious for malignancy in the right upper lobe, with invasion of the D2, D3, and D4 vertebral bodies and intraspinal extension compromising the spinal cord at D2–D4 levels.
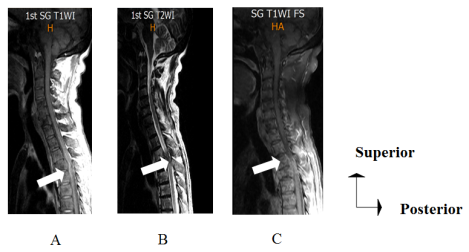
Figure 5. Cervical spine MRI, sagittal T2-weighted TSE (A) and T2 STIR (B) sequences: Multilevel disc-osteophytic protrusion from C3-C4 to C6-C7, associated with advanced hypertrophic zygapophyseal osteoarthritis at C3-C4, causing severe central spinal canal stenosis. Corresponding T2 hyperintensity within the spinal cord is noted, consistent with cervical spondylotic myelopathy.
4. Discussion
In our series, spinal cord compression accounted for 6.3% of MRI examinations performed during the study period.
This frequency was higher than that of Dagbe M et al
[1]
Dagbe M, N’timon B, Gbande P, Yaye I, Ntankeu -Tankoua P P, Kolou B et al. The MRI contribution in etiological diagnosis of the slow medullary compression in Lomé: about 72 cases. J Afr Imag Méd 2022; 14(4): 275-280.
[1]
who reported a frequency of 4.9% of patients received for slow spinal cord compression. This result can be explained by the fact that the radiology department of the National Social Security is, on one hand, one of the best-equipped imaging centers in the country, with the largest number of radiologists. On the other hand, it benefits from the proximity to two major university hospitals that house departments of neurology, neurosurgery, and rheumatology, from which the majority of our patients originate.
We observed a male predominance. This result is consistent with data from the literature
[1]
Dagbe M, N’timon B, Gbande P, Yaye I, Ntankeu -Tankoua P P, Kolou B et al. The MRI contribution in etiological diagnosis of the slow medullary compression in Lomé: about 72 cases. J Afr Imag Méd 2022; 14(4): 275-280.
[2]
Cherif Idrissi El Ganouni N, Khalil MR, Hiroual MR, El Idrissi I, Haddi M, Aït Benali S, et al. Contribution of MRI in slow spinal cord compressions of tumoral and infectious origin. Feuillets de Radiologie. 2009; 49(4): 251–262.
[5]
Ndao AC, Faye A, Diagne N, Dia AD, Dia DG, Kane BS, et al. Etiological profile of slow spinal cord compressions in Internal Medicine. RAFMI 2021; 8(1): 25-30.
[10]
Cisse NA. Chronic spinal cord compression: Epidemiological, diagnostic, and therapeutic aspects, a retrospective study of 110 cases [Doctoral thesis]. Mali: Faculty of Medicine, Pharmacy, and Odonto-Stomatology; N 26/2016. 163p.
[1, 2, 5, 10]
. This male predominance may be partly attributed to the high prevalence of cervico-arthritic myelopathies and primary osteophilic cancers, including prostate cancer.
The mean age of our patients was 51.85 ± 18.87 years, with extremes ranging from 3 to 92 years. This average age was comparable to that reported by Amjoud M
[5]
Ndao AC, Faye A, Diagne N, Dia AD, Dia DG, Kane BS, et al. Etiological profile of slow spinal cord compressions in Internal Medicine. RAFMI 2021; 8(1): 25-30.
[5]
in Morocco and by Ndao A. C et al.
[6]
New PW, Cripps RA, Bonne Lee B. Global maps of non-traumatic spinal cord injury epidemiology: towards a living data repository. Spinal Cord 2014; 52(2): 97–109.
[6]
, who found mean ages of 53.2 and 58 years, respectively. In contrast, Badij N et al.
[11]
Badij N, Deme H, Akpo G, Ndong B, Toure MH, Diop SB et al. The contribution of MRI in the management of slowly progressive nontraumatic spinal cord compression. Pan African Medical Journal. 2016; 24(221): 1-6.
[11]
and Ekouele Mbaki H. B et al.
[12]
Camara B. Contribution of magnetic resonance imaging in the diagnosis of non-traumatic myelopathies at the Hospital of Mali [Doctoral thesis]. Bamako: University of Sciences, Techniques, and Technologies; 2022. 109 p.
[12]
reported lower mean ages of 42.6 and 49.22 years, respectively.
The most common age group was between 60 and 69 years. This result is similar to that reported by Konate M. S
[13]
Konate MS. Epidemiologic, clinical, and therapeutic aspects of chronic spinal cord compression in the neurosurgery department of Mali Hospital [doctoral thesis in Medicine]. Mali: Faculty of Medicine and Odonto-Stomatology; N 093/2021. 163p.
[13]
, who found that the majority of cases occurred in individuals aged 60 years and older. This can be explained by the fact that this pathology is more frequently observed after the age of forty
[10]
Cisse NA. Chronic spinal cord compression: Epidemiological, diagnostic, and therapeutic aspects, a retrospective study of 110 cases [Doctoral thesis]. Mali: Faculty of Medicine, Pharmacy, and Odonto-Stomatology; N 26/2016. 163p.
[10]
.
The majority of patients were referred by the neurology department (67.6%), which differs from the findings of Fadiga S. I
[9]
Fadiga SI. MRI features of infectious spondylodiscitis in the medical imaging department of Mali Hospital: a series of 152 cases [DES Radiology and Medical Imaging Thesis]. Mali: Faculty of Medicine and Odonto-Stomatology 2022. 106 p.
[9]
, where most patients were referred by the neurosurgery department (51%). This discrepancy could be explained by the proximity of the neurology department to our unit, combined with patients limited awareness of spinal cord compression symptoms, which may have led them to seek care in less appropriate departments. Additionally, the absence of a triage system at the admissions unit may have contributed to this pattern.
The mean interval for obtaining an MRI was 2 days, which is notably shorter than the mean delay of over 5 days reported by Dagbe M et al.
[1]
Dagbe M, N’timon B, Gbande P, Yaye I, Ntankeu -Tankoua P P, Kolou B et al. The MRI contribution in etiological diagnosis of the slow medullary compression in Lomé: about 72 cases. J Afr Imag Méd 2022; 14(4): 275-280.
[1]
. This could be attributed to the relatively high cost of MRI which often exceeding the financial capacity of patients from low- to middle-income backgrounds, as well as logistical challenges related to patient transportation.
Spinal pain and motor deficits were the most common reasons for consultation in our studies, each reported in 70.6% of cases. These results are consistent with prior studies, including those by Amjoud M
[4]
Amjoud M. Contibution of MRI to non-traumatic spinal cord compression [Doctoral thesis in Medicine]. Marrakech: Faculty of Medicine and Pharmacy of Marrakech.; N 017/2023; 154 p.
[4]
, who reported a 70% prevalence of spinal pain, and Musubire A. K et al.
[14]
Musubire AK, Meya DB, Katabira ET, Meyer ACL, Bohjanen PR, Boulware DR et al. Epidemiology of non-traumatic spinal cord injury in Uganda: a single center, prospective study with MRI evaluation. BMC Neurol. 2019; 19(1): 10.
[14]
, who identified motor deficits as the predominant clinical feature in 70% of patients.
The cervical and thoracic spine were the most commonly involved regions, each representing 41.2% of cases. This distribution contrasts with findings by Fadoukhair Z et al.
[15]
Fadoukhair Z, Lalya I, Amzerin M, Ismaili N, Belbaraka R, Bensouda Y, et al. Malignant cord compression. J Afr Cancer 2012; 4: 142-150.
[15]
and Ekouele Mbaki H. B et al.
[16]
Ekouele Mbaki HB, Boukassa L, Sounga Bandzouzi PEG, Diatewa J, Mpandzou GA, Ossou-Nguiet PM. Etiologies and treatment of nontraumatic radiculo-medullary compression in neurosurgical environment at Brazzaville. Health Sci. Dis: 2020; 21(1): 75-79.
[16]
, who reported higher involvement of the thoracic spine (60% and 47%, respectively) and lumbar spine (24% in both studies).
Regarding contrast agent administration, 48.5% of our patients did not receive contrast enhancement. This frequency of non-enhanced examinations was lower than that reported in Camara B's study
[12]
Camara B. Contribution of magnetic resonance imaging in the diagnosis of non-traumatic myelopathies at the Hospital of Mali [Doctoral thesis]. Bamako: University of Sciences, Techniques, and Technologies; 2022. 109 p.
[12]
, where non-enhanced scans accounted for 89.5% of cases.
In both studies, degenerative pathologies were predominant, and the diagnosis of these conditions did not require gadolinium contrast administration.
Gadolinium contrast administration is particularly valuable for detecting tumorous or infectious pathologies, as it not only enhances lesion visualization but simultaneously enables assessment of intraspinal extension and potential spinal cord infiltration.
Degenerative processes accounted for 33.8% of cases, comparable to the 32% rate of degenerative lesions reported by Badji N et al
[11]
Badij N, Deme H, Akpo G, Ndong B, Toure MH, Diop SB et al. The contribution of MRI in the management of slowly progressive nontraumatic spinal cord compression. Pan African Medical Journal. 2016; 24(221): 1-6.
[11]
in Dakar. In our study, the affected compartment showed predominantly extraforaminal involvement (83.8%). This result is in line with the findings of Cherif Idrissi El Ganouni N et al.
[2]
Cherif Idrissi El Ganouni N, Khalil MR, Hiroual MR, El Idrissi I, Haddi M, Aït Benali S, et al. Contribution of MRI in slow spinal cord compressions of tumoral and infectious origin. Feuillets de Radiologie. 2009; 49(4): 251–262.
[2]
, who also reported a predominance of extra-foraminal involvement, accounting for 70% of cases.
In our series, cervical spondylotic myelopathy was the most frequently suspected etiological radiological diagnosis (33.9%). This contrasts with the rates reported by Diomandé M et al.
[17]
Diomandé M, Nseng-Nseng RIO, Kouamé-Assouan AE, Gbané-Koné M, Coulibaly AK et al. Spinal cord compressions: prevalence and etiology, experience of Department of Rheumatology of the University Hospital of Cocody in Abidjan. Rev Mar Rhum 2015; 33: 27-30.
[17]
and Kassegne I et al.
[7]
Kassegne I, Sakiye K, Kanassoua K, Beketi AK, Seydou Badiane B, Koffi Balogou AA. Management of spinal cord compression in Togo. Med Sante Trop 2013; 23: 206-210.
[7]
(14.8% and 23%, respectively). Cervical spondylotic myelopathy is the most common form of spinal cord dysfunction in adults. It results from It results from cervical spinal canal narrowing due to age-related arthritic changes.
[18]
Milligan J, Ryan K, Fehling M, Bauman C. Degenerative myelopathy: Diagnosis and management in primary care. Canadian Family Physicians 2019; 65(9): 619-624.
[18]
5. Conclusion
Slow spinal cord compression represents a highly recurrent spinal pathology affecting patients of all ages, with a predilection for elderly males. The extraforaminal compartment is most frequently involved.
The cervical and thoracic levels were the most frequently involved. Degenerative pathology, particularly cervical spondylotic myelopathy, was the most common diagnosis. This was followed by tumor pathology, with spinal metastasis being the most frequent type of tumor lesion.
However, there is a delay in performing spinal cord MRI after it is requested. A larger multicenter study with a longer investigation period could help identify other etiologies of slow-progressing spinal cord compression on MRI.
Dagbe M, N’timon B, Gbande P, Yaye I, Ntankeu -Tankoua P P, Kolou B et al. The MRI contribution in etiological diagnosis of the slow medullary compression in Lomé: about 72 cases. J Afr Imag Méd 2022; 14(4): 275-280.
[2]
Cherif Idrissi El Ganouni N, Khalil MR, Hiroual MR, El Idrissi I, Haddi M, Aït Benali S, et al. Contribution of MRI in slow spinal cord compressions of tumoral and infectious origin. Feuillets de Radiologie. 2009; 49(4): 251–262.
[3]
Ayoun AR. Spinal Cord Compression. Faculty of Medicine of Oran. Neurology Module, 4th Year Medical Studies.
[4]
Amjoud M. Contibution of MRI to non-traumatic spinal cord compression [Doctoral thesis in Medicine]. Marrakech: Faculty of Medicine and Pharmacy of Marrakech.; N 017/2023; 154 p.
[5]
Ndao AC, Faye A, Diagne N, Dia AD, Dia DG, Kane BS, et al. Etiological profile of slow spinal cord compressions in Internal Medicine. RAFMI 2021; 8(1): 25-30.
[6]
New PW, Cripps RA, Bonne Lee B. Global maps of non-traumatic spinal cord injury epidemiology: towards a living data repository. Spinal Cord 2014; 52(2): 97–109.
[7]
Kassegne I, Sakiye K, Kanassoua K, Beketi AK, Seydou Badiane B, Koffi Balogou AA. Management of spinal cord compression in Togo. Med Sante Trop 2013; 23: 206-210.
[8]
Camara MA, N’Diaye M, Coulibaly MB, Traore MM, Diarra H, Toure BM et al. MRI Contribution in the Diagnosis of Non-Traumatic Medular Compressions at the Mali Hospital of about 179 Cases. Open Journal of Medical Imaging. 2020; 10: 186-195.
[9]
Fadiga SI. MRI features of infectious spondylodiscitis in the medical imaging department of Mali Hospital: a series of 152 cases [DES Radiology and Medical Imaging Thesis]. Mali: Faculty of Medicine and Odonto-Stomatology 2022. 106 p.
[10]
Cisse NA. Chronic spinal cord compression: Epidemiological, diagnostic, and therapeutic aspects, a retrospective study of 110 cases [Doctoral thesis]. Mali: Faculty of Medicine, Pharmacy, and Odonto-Stomatology; N 26/2016. 163p.
[11]
Badij N, Deme H, Akpo G, Ndong B, Toure MH, Diop SB et al. The contribution of MRI in the management of slowly progressive nontraumatic spinal cord compression. Pan African Medical Journal. 2016; 24(221): 1-6.
[12]
Camara B. Contribution of magnetic resonance imaging in the diagnosis of non-traumatic myelopathies at the Hospital of Mali [Doctoral thesis]. Bamako: University of Sciences, Techniques, and Technologies; 2022. 109 p.
[13]
Konate MS. Epidemiologic, clinical, and therapeutic aspects of chronic spinal cord compression in the neurosurgery department of Mali Hospital [doctoral thesis in Medicine]. Mali: Faculty of Medicine and Odonto-Stomatology; N 093/2021. 163p.
[14]
Musubire AK, Meya DB, Katabira ET, Meyer ACL, Bohjanen PR, Boulware DR et al. Epidemiology of non-traumatic spinal cord injury in Uganda: a single center, prospective study with MRI evaluation. BMC Neurol. 2019; 19(1): 10.
[15]
Fadoukhair Z, Lalya I, Amzerin M, Ismaili N, Belbaraka R, Bensouda Y, et al. Malignant cord compression. J Afr Cancer 2012; 4: 142-150.
[16]
Ekouele Mbaki HB, Boukassa L, Sounga Bandzouzi PEG, Diatewa J, Mpandzou GA, Ossou-Nguiet PM. Etiologies and treatment of nontraumatic radiculo-medullary compression in neurosurgical environment at Brazzaville. Health Sci. Dis: 2020; 21(1): 75-79.
[17]
Diomandé M, Nseng-Nseng RIO, Kouamé-Assouan AE, Gbané-Koné M, Coulibaly AK et al. Spinal cord compressions: prevalence and etiology, experience of Department of Rheumatology of the University Hospital of Cocody in Abidjan. Rev Mar Rhum 2015; 33: 27-30.
[18]
Milligan J, Ryan K, Fehling M, Bauman C. Degenerative myelopathy: Diagnosis and management in primary care. Canadian Family Physicians 2019; 65(9): 619-624.
Abdoulaye, B. A., Aminata, B. O., Mamoudou, C., Pihou, G. (2025). The Contribution of Magnetic Resonance Imaging (MRI) to the Etiological Diagnosis of Slow Spinal Cord Compression. International Journal of Medical Imaging, 13(2), 20-26. https://doi.org/10.11648/j.ijmi.20251302.11
Abdoulaye, B. A.; Aminata, B. O.; Mamoudou, C.; Pihou, G. The Contribution of Magnetic Resonance Imaging (MRI) to the Etiological Diagnosis of Slow Spinal Cord Compression. Int. J. Med. Imaging2025, 13(2), 20-26. doi: 10.11648/j.ijmi.20251302.11
Abdoulaye BA, Aminata BO, Mamoudou C, Pihou G. The Contribution of Magnetic Resonance Imaging (MRI) to the Etiological Diagnosis of Slow Spinal Cord Compression. Int J Med Imaging. 2025;13(2):20-26. doi: 10.11648/j.ijmi.20251302.11
@article{10.11648/j.ijmi.20251302.11,
author = {Balde Alpha Abdoulaye and Bah Ousmane Aminata and Camara Mamoudou and Gbande Pihou},
title = {The Contribution of Magnetic Resonance Imaging (MRI) to the Etiological Diagnosis of Slow Spinal Cord Compression},
journal = {International Journal of Medical Imaging},
volume = {13},
number = {2},
pages = {20-26},
doi = {10.11648/j.ijmi.20251302.11},
url = {https://doi.org/10.11648/j.ijmi.20251302.11},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ijmi.20251302.11},
abstract = {Introduction: The goal of this study was to determine the contribution of Magnetic Resonance Imaging (MRI) in the etiological diagnosis of slow spinal cord compressions. Methods: This was a prospective descriptive study conducted over a period of six months, from August 16, 2023, to February 16, 2024. Results: During the study period, 1082 MRI scans were performed, of which 68 cases (6.28%) were diagnosed with slow spinal cord compressions. The mean age of patients was 51.85 ± 18.87 years, ranging from 3 to 92 years. Males accounted for 72.1% (n = 49), with a sex ratio of 2.57. Most patients were referred by the neurology department (67.6%). The average time to MRI examination after clinical consultation was 2 ± 0.71 days. The most common presenting symptoms were spinal pain and motor disturbances, noted in 70.6% of cases. The cervical and thoracic spinal levels were the most frequently affected, each accounting for more than 41.2% (n = 28) of cases. Extradural lesions were predominant, observed in 83.8% of cases. Degenerative pathologies were the most common cause (44.1%), followed by tumoral lesions (42.6%). Cervicoarthrosic myelopathy was the most frequent radiologic diagnosis, accounting for 33.9% of cases. Conclusion: Slow spinal cord compression is a recurrent spinal cord pathology affecting individuals of all ages, with a male predominance. The extradural compartment is most frequently involved, primarily due to degenerative conditions, especially cervical spondylotic myelopathy. Tumoral lesions, primarly metastatic, represent the second most frequent etiology.
},
year = {2025}
}
TY - JOUR
T1 - The Contribution of Magnetic Resonance Imaging (MRI) to the Etiological Diagnosis of Slow Spinal Cord Compression
AU - Balde Alpha Abdoulaye
AU - Bah Ousmane Aminata
AU - Camara Mamoudou
AU - Gbande Pihou
Y1 - 2025/06/30
PY - 2025
N1 - https://doi.org/10.11648/j.ijmi.20251302.11
DO - 10.11648/j.ijmi.20251302.11
T2 - International Journal of Medical Imaging
JF - International Journal of Medical Imaging
JO - International Journal of Medical Imaging
SP - 20
EP - 26
PB - Science Publishing Group
SN - 2330-832X
UR - https://doi.org/10.11648/j.ijmi.20251302.11
AB - Introduction: The goal of this study was to determine the contribution of Magnetic Resonance Imaging (MRI) in the etiological diagnosis of slow spinal cord compressions. Methods: This was a prospective descriptive study conducted over a period of six months, from August 16, 2023, to February 16, 2024. Results: During the study period, 1082 MRI scans were performed, of which 68 cases (6.28%) were diagnosed with slow spinal cord compressions. The mean age of patients was 51.85 ± 18.87 years, ranging from 3 to 92 years. Males accounted for 72.1% (n = 49), with a sex ratio of 2.57. Most patients were referred by the neurology department (67.6%). The average time to MRI examination after clinical consultation was 2 ± 0.71 days. The most common presenting symptoms were spinal pain and motor disturbances, noted in 70.6% of cases. The cervical and thoracic spinal levels were the most frequently affected, each accounting for more than 41.2% (n = 28) of cases. Extradural lesions were predominant, observed in 83.8% of cases. Degenerative pathologies were the most common cause (44.1%), followed by tumoral lesions (42.6%). Cervicoarthrosic myelopathy was the most frequent radiologic diagnosis, accounting for 33.9% of cases. Conclusion: Slow spinal cord compression is a recurrent spinal cord pathology affecting individuals of all ages, with a male predominance. The extradural compartment is most frequently involved, primarily due to degenerative conditions, especially cervical spondylotic myelopathy. Tumoral lesions, primarly metastatic, represent the second most frequent etiology.
VL - 13
IS - 2
ER -
Faculty of Health Sciences and Technology, Gamal Abdel Nasser University of Conakry, Conakry, Republic of Guinea; Diagnostic Center, National Social Security Fund, Conakry, Republic of Guinea; Radiology and Medical Imaging Department, Donka University Hospital, Conakry, Republic of Guinea
Faculty of Health Sciences and Technology, Gamal Abdel Nasser University of Conakry, Conakry, Republic of Guinea; Army Reference Diagnostic Center, Conakry Military Hospital, Conakry, Republic of Guinea
Abdoulaye, B. A., Aminata, B. O., Mamoudou, C., Pihou, G. (2025). The Contribution of Magnetic Resonance Imaging (MRI) to the Etiological Diagnosis of Slow Spinal Cord Compression. International Journal of Medical Imaging, 13(2), 20-26. https://doi.org/10.11648/j.ijmi.20251302.11
Abdoulaye, B. A.; Aminata, B. O.; Mamoudou, C.; Pihou, G. The Contribution of Magnetic Resonance Imaging (MRI) to the Etiological Diagnosis of Slow Spinal Cord Compression. Int. J. Med. Imaging2025, 13(2), 20-26. doi: 10.11648/j.ijmi.20251302.11
Abdoulaye BA, Aminata BO, Mamoudou C, Pihou G. The Contribution of Magnetic Resonance Imaging (MRI) to the Etiological Diagnosis of Slow Spinal Cord Compression. Int J Med Imaging. 2025;13(2):20-26. doi: 10.11648/j.ijmi.20251302.11
@article{10.11648/j.ijmi.20251302.11,
author = {Balde Alpha Abdoulaye and Bah Ousmane Aminata and Camara Mamoudou and Gbande Pihou},
title = {The Contribution of Magnetic Resonance Imaging (MRI) to the Etiological Diagnosis of Slow Spinal Cord Compression},
journal = {International Journal of Medical Imaging},
volume = {13},
number = {2},
pages = {20-26},
doi = {10.11648/j.ijmi.20251302.11},
url = {https://doi.org/10.11648/j.ijmi.20251302.11},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ijmi.20251302.11},
abstract = {Introduction: The goal of this study was to determine the contribution of Magnetic Resonance Imaging (MRI) in the etiological diagnosis of slow spinal cord compressions. Methods: This was a prospective descriptive study conducted over a period of six months, from August 16, 2023, to February 16, 2024. Results: During the study period, 1082 MRI scans were performed, of which 68 cases (6.28%) were diagnosed with slow spinal cord compressions. The mean age of patients was 51.85 ± 18.87 years, ranging from 3 to 92 years. Males accounted for 72.1% (n = 49), with a sex ratio of 2.57. Most patients were referred by the neurology department (67.6%). The average time to MRI examination after clinical consultation was 2 ± 0.71 days. The most common presenting symptoms were spinal pain and motor disturbances, noted in 70.6% of cases. The cervical and thoracic spinal levels were the most frequently affected, each accounting for more than 41.2% (n = 28) of cases. Extradural lesions were predominant, observed in 83.8% of cases. Degenerative pathologies were the most common cause (44.1%), followed by tumoral lesions (42.6%). Cervicoarthrosic myelopathy was the most frequent radiologic diagnosis, accounting for 33.9% of cases. Conclusion: Slow spinal cord compression is a recurrent spinal cord pathology affecting individuals of all ages, with a male predominance. The extradural compartment is most frequently involved, primarily due to degenerative conditions, especially cervical spondylotic myelopathy. Tumoral lesions, primarly metastatic, represent the second most frequent etiology.
},
year = {2025}
}
TY - JOUR
T1 - The Contribution of Magnetic Resonance Imaging (MRI) to the Etiological Diagnosis of Slow Spinal Cord Compression
AU - Balde Alpha Abdoulaye
AU - Bah Ousmane Aminata
AU - Camara Mamoudou
AU - Gbande Pihou
Y1 - 2025/06/30
PY - 2025
N1 - https://doi.org/10.11648/j.ijmi.20251302.11
DO - 10.11648/j.ijmi.20251302.11
T2 - International Journal of Medical Imaging
JF - International Journal of Medical Imaging
JO - International Journal of Medical Imaging
SP - 20
EP - 26
PB - Science Publishing Group
SN - 2330-832X
UR - https://doi.org/10.11648/j.ijmi.20251302.11
AB - Introduction: The goal of this study was to determine the contribution of Magnetic Resonance Imaging (MRI) in the etiological diagnosis of slow spinal cord compressions. Methods: This was a prospective descriptive study conducted over a period of six months, from August 16, 2023, to February 16, 2024. Results: During the study period, 1082 MRI scans were performed, of which 68 cases (6.28%) were diagnosed with slow spinal cord compressions. The mean age of patients was 51.85 ± 18.87 years, ranging from 3 to 92 years. Males accounted for 72.1% (n = 49), with a sex ratio of 2.57. Most patients were referred by the neurology department (67.6%). The average time to MRI examination after clinical consultation was 2 ± 0.71 days. The most common presenting symptoms were spinal pain and motor disturbances, noted in 70.6% of cases. The cervical and thoracic spinal levels were the most frequently affected, each accounting for more than 41.2% (n = 28) of cases. Extradural lesions were predominant, observed in 83.8% of cases. Degenerative pathologies were the most common cause (44.1%), followed by tumoral lesions (42.6%). Cervicoarthrosic myelopathy was the most frequent radiologic diagnosis, accounting for 33.9% of cases. Conclusion: Slow spinal cord compression is a recurrent spinal cord pathology affecting individuals of all ages, with a male predominance. The extradural compartment is most frequently involved, primarily due to degenerative conditions, especially cervical spondylotic myelopathy. Tumoral lesions, primarly metastatic, represent the second most frequent etiology.
VL - 13
IS - 2
ER -