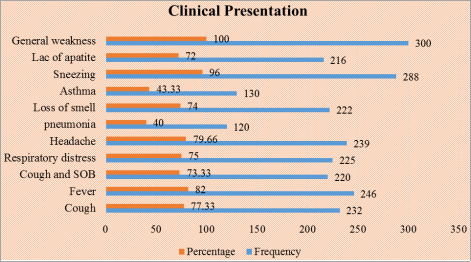
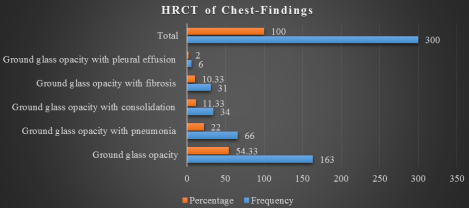
Introduction: Recent studies have assessed the importance of chest CT scans, particularly high-resolution CT (HRCT), in hospitalized COVID-19 patients who are suspected of having the virus or have had false negative test results. Objective: The aim of this study was to determine the outcome of High-Resolution Computed Tomography (HRCT) of chest of confirmed COVID-19 positive cases. Methodology: This was a cross-sectional prospective study carried out in the department of Radiology and imaging in collaboration with the department of Virology and COVID unit in IbnSina Hospital, Dhaka, Bangladesh during January, 2022 to June, 2022. A total of 300 confirmed COVID-19 positive admitted cases in the hospital, aged above 18 years were enrolled in this study. All the patients were under went High Resolution Computed Tomography (HRCT) of Chest scan. The collected data were cleaned, edited and entered into computer for analysis. The data were analyzed by SPSS-23.0. The ethical clearance of this study was obtained from the Ethics Committee of School of Public Health & Life Science, University of South Asia, and Dhaka, Bangladesh. Results: In this study a total of 300 COVID-19 positive cases were enrolled. Among the patients, the majority203 (67.66%) patients belonged to the age group >52 years, which was the highest and followed by 44 (14.66%) age group (43-52) years, 36 (12%) (33-42) years, 14 (4.66%) (22-32) years and 3 (1%) <22 years. According to sex distribution, the majority cases 160 (53.33%) were male and 140 (46.66%) were female. According to the distribution of clinical presentation, the highest symptom was observed, general weakness 300 (100%) and followed by sneezing 288 (96%), fever 246 (82%), headache 239 (79.66%), cough 232 (77.33%), respiratory distress, 225 (75%), cough and SOB, 220 (73.33%), loss of smell, 222 (74%), lac of apatite, 216 (72%), asthma 130 (43.33) and pneumonia, 120 (40%). According to the distribution of HRCT findings of chest of the COVID-19 positive cases, 163 (54.33%) had Ground glass opacity, which was the largest observation and followed by 66 (22%), Ground glass opacity with pneumonia, 34 (11.33%) Ground glass opacity with consolidation, 31 (10.33) Ground glass opacity with fibrosis, and 6 (2%) Ground glass opacity with pleural effusion. Conclusion: The results of this study indicate that doing a high-resolution computed tomography (HRCT) scan of the chest is a valuable method for diagnosing and assessing the response to treatment in COVID-19 patients. Additionally, it serves as a significant predictor for future prognosis.
| Published in | International Journal of Medical Imaging (Volume 12, Issue 2) |
| DOI | 10.11648/j.ijmi.20241202.15 |
| Page(s) | 51-56 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2024. Published by Science Publishing Group |
Outcome. HRCT, Scan, Chest COVID-19, Positive, Cases, Ground Glass Opacity (GGO), Dedicated, Hospital
Age in years | Frequency | Percentage |
|---|---|---|
< 22 | 3 | 1 |
22-32 | 14 | 4.66 |
33-42 | 36 | 12 |
43-52 | 44 | 14.66 |
> 52 | 203 | 67.66 |
Total | 300 | 100 |
Clinical Presentation | Frequency | Percentage |
|---|---|---|
Cough | 232 | 77.33 |
Fever | 246 | 82 |
Cough and SOB | 220 | 73.33 |
Respiratory distress | 225 | 75 |
Headache | 239 | 79.66 |
pneumonia | 120 | 40 |
Loss of smell | 222 | 74 |
Asthma | 130 | 43.33 |
Sneezing | 288 | 96 |
Lac of apatite | 216 | 72 |
General weakness | 300 | 100 |
HRCT of Chest- Findings | Frequency | Percentage |
|---|---|---|
Ground glass opacity | 163 | 54.33 |
Ground glass opacity with pneumonia | 66 | 22 |
Ground glass opacity with consolidation | 34 | 11.33 |
Ground glass opacity with fibrosis | 31 | 10.33 |
Ground glass opacity with pleural effusion | 6 | 2 |
Total | 300 | 100 |
| [1] | Zhu N, Zhang D, Wang W, et al. A novel coronavirus from patients with pneumonia in China, 2019. New Engl J Med 2020; 382: 727-33. [PMC free article] [PubMed] [Google Scholar] |
| [2] | Wang C, Horby PW, Hayden FG, et al. A novel coronavirus outbreak of global health concern. Lancet 2020; 395: 470-3. [PMC free article] [PubMed] [Google Scholar] |
| [3] | Lu H, Stratton CW, Tang YW. Outbreak of pneumonia of unknown etiology in Wuhan China: the mystery and the miracle. J Med Virol 2020; 92: 401-2. [PMC free article] [PubMed] [Google Scholar] |
| [4] | Sohrabi C, Alsafi Z, O’Neill N, et al. World Health Organization declares global emergency: A review of the 2019 novel coronavirus (COVID-19). Inter J Surg 2020; 76: 71-6. [Google Scholar] |
| [5] | Kozera B, Rapacz M. Reference genes in real-time PCR. J Appl Genet. 2013 Nov; 54(4): 391-406. PMID: 24078518; PMCID: PMC3825189. |
| [6] | Ishfaq A, Farooq SM, Goraya A, Yousaf M, Gilani SA, Kiran A, Ayoub M, Javed A, Bacha R. Role of High Resolution Computed Tomography chest in the diagnosis and evaluation of COVID-19 patients-A systematic review and meta-analysis. European journal of radiology open. 2021 Jan 1; 8: 100350. |
| [7] | Ai T, Yang Z, Hou H, Zhan C, Chen C, Lv W, et al. Correlation of chest CT and RT-PCR testing for Coronavirus disease 2019 (COVID-19) in China: A report of 1014 cases. Radiology 2020; 296: E32-40. |
| [8] | Fang Y, Zhang H, Xie J, Lin M, Ying L, Pang P, et al. Sensitivity of chest CT for COVID-19: Comparison to RT-PCR. Radiology 2020; 296: E115-7. |
| [9] | Huang P, Liu T, Huang L, Liu H, Lei M, Xu W, et al. Use of chest CT in combination with negative RT-PCR assay for the 2019 novel coronavirus but high clinical suspicion. Radiology 2020; 295: 22-3. |
| [10] | Chen D, Jiang X, Hong Y, Wen Z, Wei S, Peng G, et al. Can chest CT features distinguish patients with negative from those with positive initial RT-PCR results for coronavirus disease (COVID-19)? AJR Am J Roentgenol 2020; 216: 66-70. |
| [11] | Raman S, Bahar T. COVID 19: The New Threat, Int J Infect. 2020; 7(1): e102184. |
| [12] | Bayraktaroğlu S, Çinkooğlu A, Ceylan N, Savaş R (2020) The novel coronavirus pneumonia (COVID-19): a pictorial review of chest CT features. DiagnIntervRadiol. |
| [13] | Kim H, Hong H, Yoon SH. Diagnostic performance of CT and reverse transcriptase polymerase chain reaction for coronavirus disease 2019: A meta- analysis. Radiology 2020; 296: E145-55. |
| [14] | Zhang, N., Xu, X., Zhou, L. et al. Clinical characteristics and Chest CT imaging features of critically ill COVID 19 patients. EurRadiol (2020). |
| [15] | Adams HJ, Kwee TC, Yakar D, Hope MD, Kwee RM. Systematic review and meta-analysis on the value of chest CT in the diagnosis of coronavirus disease (COVID-19): Sol Scientiae, Illustra Nos. AJR Am J Roentgenol 2020; 215: 1342-50. |
| [16] | Bernheim A, Mei X, Huang M, Yang Y, Fayad ZA, Zhang N, Diao K, Lin B, Zhu X, Li K, Li S, Shan H, Jacobi A, Chung M. Chest CT Findings in Coronavirus Disease-19 (COVID-19): Relationship to Duration of Infection. Radiology. 2020 Jun; 295(3): 200463. |
| [17] | Simpson S, Kay FU, Abbara S, Bhalla S, Chung JH, Chung M, et al. Radiological society of North America expert consensus document on reporting chest CT findings related to COVID-19: Endorsed by the society of thoracic radiology, the American College of Radiology, and RSNA. J Thorac Imaging 2020; 35: 219-27. |
| [18] | Paul NS, Roberts H, Butany J, Chung T, Gold W, Mehta S, Konen E, Rao A, Provost Y, Hong HH, Zelovitsky L, Weisbrod GL. Radiologic pattern of disease in patients with severe acute respiratory syndrome: the Toronto experience. Radiographics 2004; 24: 553-63. [Crossref] [PubMed] |
| [19] | Inui S, Fujikawa A, Jitsu M, Kunishima N, Watanabe S, Suzuki Y, Umeda S, Uwabe Y. Chest CT Findings in Cases from the Cruise Ship “Diamond Princess” with Coronavirus Disease 2019 (COVID-Radiology: Cardiothorac Imaging 2020. |
| [20] | Xu R, Du M, Li L, Zhen Z, Wang H, Hu X. CT imaging of one extended family cluster of corona virus disease 2019 (COVID-19) including adolescent patients and “silent infection”. Quant Imaging Med Surg 2020; 10: 800-804. [Crossref] [PubMed] |
| [21] | Zhou Z, Guo D, Li C, Fang Z, Chen L, Yang R, Li X, Zeng W. Coronavirus disease 2019: initial chest CT findings. Eur Radiol 2020. Epub ahead of print. [Crossref] [PubMed] |
| [22] | Bai HX, Hsieh B, Xiong Z, Halsey K, Choi JW, Tran TML, Pan I, Shi LB, Wang DC, Mei J, Jiang XL, Zeng QH, Egglin TK, Hu PF, Agarwal S, Xie F, Li S, Healey T, Atalay MK, Liao WH. Performance of radiologists in differentiating COVID-19 from viral pneumonia on chest CT. Radiology 2020. Epub ahead of print. [Crossref] [PubMed] |
| [23] | Li Y, Xia L. Coronavirus disease 2019 (COVID-19): role of chest CT in diagnosis and management. AJR Am J Roentgenol 2020. Epub ahead of print. [Crossref] [PubMed] |
| [24] | Ng MY, Lee M, Yang J, Yang F, Li X, Wang H, Lui M, Lo C, Leung B, Khong P, Hui C, Yuen K, Kuo M. Imaging profile of the COVID-19 infection: Radiologic findings and literature review. Radiology Cardiothorac Imaging 2020. |
APA Style
Ahamed, M., Sikder, M. R., Rahman, M. M., Sumon, S. R., Rahman, M. M., et al. (2024). Outcome of High Resolution Computed Tomography (HRCT) Scan of Chest of COVID-19 Affected Patients: A Study in a COVID-19 Dedicated Hospital. International Journal of Medical Imaging, 12(2), 51-56. https://doi.org/10.11648/j.ijmi.20241202.15
ACS Style
Ahamed, M.; Sikder, M. R.; Rahman, M. M.; Sumon, S. R.; Rahman, M. M., et al. Outcome of High Resolution Computed Tomography (HRCT) Scan of Chest of COVID-19 Affected Patients: A Study in a COVID-19 Dedicated Hospital. Int. J. Med. Imaging 2024, 12(2), 51-56. doi: 10.11648/j.ijmi.20241202.15
AMA Style
Ahamed M, Sikder MR, Rahman MM, Sumon SR, Rahman MM, et al. Outcome of High Resolution Computed Tomography (HRCT) Scan of Chest of COVID-19 Affected Patients: A Study in a COVID-19 Dedicated Hospital. Int J Med Imaging. 2024;12(2):51-56. doi: 10.11648/j.ijmi.20241202.15
@article{10.11648/j.ijmi.20241202.15,
author = {Marzuk Ahamed and Mohammad Ripon Sikder and Mohammad Mojibur Rahman and Sohel Rana Sumon and Mohammad Motiur Rahman and Abdur Rab Akanda and Mohammad Salehin Abedin},
title = {Outcome of High Resolution Computed Tomography (HRCT) Scan of Chest of COVID-19 Affected Patients: A Study in a COVID-19 Dedicated Hospital
},
journal = {International Journal of Medical Imaging},
volume = {12},
number = {2},
pages = {51-56},
doi = {10.11648/j.ijmi.20241202.15},
url = {https://doi.org/10.11648/j.ijmi.20241202.15},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ijmi.20241202.15},
abstract = {Introduction: Recent studies have assessed the importance of chest CT scans, particularly high-resolution CT (HRCT), in hospitalized COVID-19 patients who are suspected of having the virus or have had false negative test results. Objective: The aim of this study was to determine the outcome of High-Resolution Computed Tomography (HRCT) of chest of confirmed COVID-19 positive cases. Methodology: This was a cross-sectional prospective study carried out in the department of Radiology and imaging in collaboration with the department of Virology and COVID unit in IbnSina Hospital, Dhaka, Bangladesh during January, 2022 to June, 2022. A total of 300 confirmed COVID-19 positive admitted cases in the hospital, aged above 18 years were enrolled in this study. All the patients were under went High Resolution Computed Tomography (HRCT) of Chest scan. The collected data were cleaned, edited and entered into computer for analysis. The data were analyzed by SPSS-23.0. The ethical clearance of this study was obtained from the Ethics Committee of School of Public Health & Life Science, University of South Asia, and Dhaka, Bangladesh. Results: In this study a total of 300 COVID-19 positive cases were enrolled. Among the patients, the majority203 (67.66%) patients belonged to the age group >52 years, which was the highest and followed by 44 (14.66%) age group (43-52) years, 36 (12%) (33-42) years, 14 (4.66%) (22-32) years and 3 (1%) <22 years. According to sex distribution, the majority cases 160 (53.33%) were male and 140 (46.66%) were female. According to the distribution of clinical presentation, the highest symptom was observed, general weakness 300 (100%) and followed by sneezing 288 (96%), fever 246 (82%), headache 239 (79.66%), cough 232 (77.33%), respiratory distress, 225 (75%), cough and SOB, 220 (73.33%), loss of smell, 222 (74%), lac of apatite, 216 (72%), asthma 130 (43.33) and pneumonia, 120 (40%). According to the distribution of HRCT findings of chest of the COVID-19 positive cases, 163 (54.33%) had Ground glass opacity, which was the largest observation and followed by 66 (22%), Ground glass opacity with pneumonia, 34 (11.33%) Ground glass opacity with consolidation, 31 (10.33) Ground glass opacity with fibrosis, and 6 (2%) Ground glass opacity with pleural effusion. Conclusion: The results of this study indicate that doing a high-resolution computed tomography (HRCT) scan of the chest is a valuable method for diagnosing and assessing the response to treatment in COVID-19 patients. Additionally, it serves as a significant predictor for future prognosis.
},
year = {2024}
}
TY - JOUR T1 - Outcome of High Resolution Computed Tomography (HRCT) Scan of Chest of COVID-19 Affected Patients: A Study in a COVID-19 Dedicated Hospital AU - Marzuk Ahamed AU - Mohammad Ripon Sikder AU - Mohammad Mojibur Rahman AU - Sohel Rana Sumon AU - Mohammad Motiur Rahman AU - Abdur Rab Akanda AU - Mohammad Salehin Abedin Y1 - 2024/05/24 PY - 2024 N1 - https://doi.org/10.11648/j.ijmi.20241202.15 DO - 10.11648/j.ijmi.20241202.15 T2 - International Journal of Medical Imaging JF - International Journal of Medical Imaging JO - International Journal of Medical Imaging SP - 51 EP - 56 PB - Science Publishing Group SN - 2330-832X UR - https://doi.org/10.11648/j.ijmi.20241202.15 AB - Introduction: Recent studies have assessed the importance of chest CT scans, particularly high-resolution CT (HRCT), in hospitalized COVID-19 patients who are suspected of having the virus or have had false negative test results. Objective: The aim of this study was to determine the outcome of High-Resolution Computed Tomography (HRCT) of chest of confirmed COVID-19 positive cases. Methodology: This was a cross-sectional prospective study carried out in the department of Radiology and imaging in collaboration with the department of Virology and COVID unit in IbnSina Hospital, Dhaka, Bangladesh during January, 2022 to June, 2022. A total of 300 confirmed COVID-19 positive admitted cases in the hospital, aged above 18 years were enrolled in this study. All the patients were under went High Resolution Computed Tomography (HRCT) of Chest scan. The collected data were cleaned, edited and entered into computer for analysis. The data were analyzed by SPSS-23.0. The ethical clearance of this study was obtained from the Ethics Committee of School of Public Health & Life Science, University of South Asia, and Dhaka, Bangladesh. Results: In this study a total of 300 COVID-19 positive cases were enrolled. Among the patients, the majority203 (67.66%) patients belonged to the age group >52 years, which was the highest and followed by 44 (14.66%) age group (43-52) years, 36 (12%) (33-42) years, 14 (4.66%) (22-32) years and 3 (1%) <22 years. According to sex distribution, the majority cases 160 (53.33%) were male and 140 (46.66%) were female. According to the distribution of clinical presentation, the highest symptom was observed, general weakness 300 (100%) and followed by sneezing 288 (96%), fever 246 (82%), headache 239 (79.66%), cough 232 (77.33%), respiratory distress, 225 (75%), cough and SOB, 220 (73.33%), loss of smell, 222 (74%), lac of apatite, 216 (72%), asthma 130 (43.33) and pneumonia, 120 (40%). According to the distribution of HRCT findings of chest of the COVID-19 positive cases, 163 (54.33%) had Ground glass opacity, which was the largest observation and followed by 66 (22%), Ground glass opacity with pneumonia, 34 (11.33%) Ground glass opacity with consolidation, 31 (10.33) Ground glass opacity with fibrosis, and 6 (2%) Ground glass opacity with pleural effusion. Conclusion: The results of this study indicate that doing a high-resolution computed tomography (HRCT) scan of the chest is a valuable method for diagnosing and assessing the response to treatment in COVID-19 patients. Additionally, it serves as a significant predictor for future prognosis. VL - 12 IS - 2 ER -
Department of Public Health and Life Science, University of South Asia, Dhaka, Bangladesh
Information