Abstract
Introduction: Autoimmune epilepsy remains under-recognized, and its true incidence remains uncertain. Objective: This study aimed to determine the prevalence of neuronal autoantibodies in patients with epilepsy of unknown etiology. Materials and Methods: An observational, longitudinal, prospective, and analytical study was conducted to assess the presence of autoantibodies associated with autoimmune encephalitis, glutamic acid decarboxylase-65 (GAD65), and onconeural antibodies in the serum and cerebrospinal fluid of consecutive patients with epilepsy of unknown etiology. Results: Sixty patients and 80 controls (30 healthy individuals, 30 with multiple sclerosis, 10 with systemic lupus erythematosus, and 10 with Sjögren's syndrome) were included to detect neuronal antibodies. Among epilepsy patients, 28 out of 60 (47%) tested positive for antibodies against N-methyl-D-aspartate receptor (NMDAR), contactin-associated protein 2 (CASPR2), leucine-rich glioma-inactivated 1 (LGI1), and glutamic acid decarboxylase (GAD), which was significantly higher (p < 0.001) than in the combined control cohort. No onconeural antibodies were detected in epilepsy patients except for 6 cases of epilepsy, 1 case of multiple sclerosis, and 3 cases of lupus with positive GAD by immunofluorescence assay and immunoblotting. There was no significant difference in antibody incidence between male and female epilepsy patients. The incidence of positive autoantibodies was significantly higher in patients with focal epilepsy compared to those with generalized epilepsy (p < 0.01). Conclusions: The findings indicate the presence of antibodies against NMDAR, VGKC-associated proteins (LGI1, CASPR2), and intracellular antigens (GAD65) in the serum and cerebrospinal fluid of patients with epilepsy, suggesting an autoimmune etiology. These results underscore the need for further research to elucidate the role of autoantibodies in epilepsy pathogenesis and to explore immunotherapeutic interventions.
Keywords
Established Epilepsy, New-Onset Epilepsy, Neuronal Autoantibodies, Voltage-Gated Potassium Channel Complex, Glutamic Acid Decarboxylase, NMDA Receptor
1. Introduction
Epileptic seizures are frequently encountered in autoimmune encephalitis, sometimes presenting as the sole symptom. The prevalence of neuronal autoantibodies in epilepsy of unknown origin varies among studies. These antibodies have been identified in conditions such as limbic encephalitis (LE)
| [1] | Vincent A, Buckley C, Schott JM, Baker I, Dewar BK, Detert N, et al. Potassium channel antibody-associated encephalopathy: a potentially immunotherapy-responsive form of limbic encephalitis. Brain 2004; 127: 701–712. https://doi.org/10.1093/brain/awh077 |
[1]
and, more recently, in faciobrachial dystonic seizures (FBDS)
| [2] | Irani SR, Michell AW, Lang B, Pettingill P, Waters P, Johnson MR, et al. Fachiobrachial dystonic seizures precede Lgi1 antibody limbic encephalitis. Ann Neurol 2011; 69: 892–900. https://doi.org/10.1002/ana.22307 |
[2]
. These encephalopathies often exhibit a monophasic course with antibody titers that typically decrease significantly within 1 to 2 years
| [3] | Buckley C, Oger J, Clover L, Tüzün E, Carpenter K, Jackson M, et al. Potassium channel antibodies in two patients with reversible limbic encephalitis. Ann Neurol 2001 50: 73–78. https://doi.org/10.1002/ana.1097 |
[3]
. Autoantibodies against neuronal antigens play a crucial role in synaptic signal transduction, contributing to seizures and neuropsychiatric manifestations. Associated autoimmune conditions include specific forms of limbic encephalitis, neuromyotonia, and Morvan's syndrome, which can be severe and potentially life-threatening, with both non-paraneoplastic and paraneoplastic etiologies.
Paraneoplastic neurological syndromes (PNS) encompass a spectrum of nervous system disorders associated with malignancies, not attributable to direct tumor effects. Instead, they are mediated by immunological mechanisms and are diagnosed based on specific antibodies known as onconeural antibodies (ONA). Graus et al. categorize ONAs against intracellular antigens as well-characterized (e.g., anti-Hu or ANNA-1, anti-Ri or ANNA-2, anti-Yo, anti-CV2/CRMP5, anti-Ma2, anti-amphiphysin, and anti-Tr or PCA-Tr) and partially characterized (e.g., anti-Zic4, anti-SOX, anti-ANNA-3, and PCA-2) antibodies. The prevalence of underlying tumors associated with these antibodies ranges from 10% to 70%, depending on the antibody type, suggesting a causal role in pathogenesis.
Early diagnosis is critical for favorable outcomes, as timely intervention with immunomodulatory therapies or tumor resection can lead to substantial symptom improvement in most patients. Neuronal protein antibodies are frequently detected in patients presenting with acute seizures suspected to have an autoimmune basis, identified by cerebrospinal fluid inflammation or abnormal neuroimaging findings
. Antibodies against proteins of the voltage-gated potassium channel complex (VGKC) and glutamic acid decarboxylase (GAD) have also been reported in a subset of patients where seizures are the primary or sole manifestation, often in the absence of overt autoimmune disease
| [5] | Kwan P, Sills GJ, Kelly K, Butler E, Brodie MJ. Glutamic acid decarboxylase autoantibodies in controlled and uncontrolled epilepsy: a pilot study. Epilepsy Res 2000 42: 191–195. https://doi.org/10.1016/s0920-1211(00)00180-7 |
[5]
. However, these studies typically recruit patients from tertiary centers, potentially biasing towards those with refractory and long-standing epilepsy. Consequently, it remains uncertain whether the elevated prevalence of neuronal autoantibodies in these contexts reflects a causal link to epilepsy or merely arises secondary to uncontrolled seizures and associated neurologic damage.
Recent reports have identified antibodies against other brain-expressed proteins, including N-methyl-D-aspartate receptor (NMDAR), α-amino-3-hydroxy-5-methyl-4-isoxazolepropionic acid receptor (AMPAR), γ-aminobutyric acid B receptor (GABABR), and glycine receptors (GLY-Rs) in patients with encephalopathies
. However, the incidence of these newer antibodies in larger cohorts of sporadic epilepsy remains poorly understood. Moreover, it is unclear whether these antibodies coexist with more established antibodies like VGKC and GAD in broader autoimmune profiles associated with seizure disorders.
This study aimed to assess the prevalence of both established and newly recognized neuronal autoantibodies in a cohort of epilepsy patients.
2. Materials and Methods
An observational, longitudinal, prospective, and analytical study was conducted to assess the presence of autoantibodies associated with autoimmune encephalitis, glutamic acid decarboxylase-65 (GAD), and onconeural antibodies in both serum and cerebrospinal fluid (CSF) of consecutive patients diagnosed with established epilepsy or recent-onset epilepsy of unknown etiology. Exclusion criteria included individuals with a history of alcohol abuse, recreational drug use, suspected non-epileptic seizures, or progressive neurological disorders. Laboratory analyses were performed based on clinical indications by the patients' neurologists as part of the differential diagnostic workup for suspected autoimmune neuroinflammatory diseases.
Serum and CSF samples underwent analysis using the following methods:
1. Tissue-based assay (IIF-TBA): Serum samples were diluted at 1:10 and 1:100, and CSF at 1:1 and 1:5, and applied onto primate cerebellum substrate. Following a 30-minute incubation and phosphate-buffered saline (PBS) wash, the substrate was further incubated with anti-IgG-fluorescein for another 30 minutes. Slides were visualized using fluorescence microscopy at 400x magnification by two independent operators.
2. Immunoblotting: A commercial immunoblotting kit (EUROLINE Paraneoplastic Neurological Syndromes 12 Ag; Euroimmun, Lübeck, Germany) was utilized according to manufacturer instructions. Reactive strips were scanned, and band intensities of Hu (ANNA1), Yo (PCA1), CV2 (CRMP5), Ri (ANNA2), Ma2, Tr (DNER), Zic-4, SOX1, recoverin, GAD, titin, and amphiphysin were evaluated using EUROLineScan software (Euroimmun, Lübeck, Germany). Band intensities ≤10 were considered negative for onconeural antibodies.
3. Cell-based assay (CBA): Serum was diluted 1:10 and CSF 1:1 and screened for antibodies against N-methyl-D-aspartate receptor (NMDAR), α-amino-3-hydroxy-5-methyl-4-isoxazolepropionic acid receptor type B (AMPAR), dipeptidyl aminopeptidase-like protein 6 (DPPX), voltage-gated potassium channels (VGKC), or VGKC-associated proteins (leucine-rich glioma-inactivated protein 1 LGI1, contactin-associated protein 2 CASPR2) using Autoimmune Encephalitis Mosaic 1 Biochip 6 (Euroimmun, Lübeck, Germany).
3. Statistical Analysis
Antibody results were expressed as relative incidence throughout the study period and analyzed using appropriate statistical tests. Categorical variables were compared using the chi-square test or Fisher's exact test, while continuous variables were assessed using the Mann-Whitney test. Demographic data and clinical characteristics were statistically compared to evaluate potential associations.
4. Results
Between January 2017 and March 2023, sixty patients with established or recent-onset epilepsy were analyzed, including serum (n = 60) and cerebrospinal fluid (CSF) samples (n = 60). The median age of the cohort was 48 years (range 15-65), with 27 patients (45%) being female.
In addition to the epilepsy cohort, were included 80 controls: 30 healthy volunteers, 30 patients with multiple sclerosis (MS), and 20 individuals with other autoimmune conditions (10 systemic lupus erythematosus, 10 Sjögren's syndrome). Serum and CSF samples were evaluated for antibodies against NMDAR, AMPAR, CASPR2, LGI1, DPPX, GABAB, and GAD in patients with epilepsy, whereas only serum samples were analyzed in healthy controls. Detailed results are summarized in
Table 1.
Among the epilepsy patients, 28 out of 60 (47%) tested positive for serum and CSF antibodies against NMDAR, CASPR2, LGI1, and GAD, representing a significantly higher incidence compared to the combined control cohort (p < 0.001) (
Table 1,
Figure 2). The most prevalent antibody was anti-NMDAR, detected in 15 epilepsy patients (25% of total), compared to 4 controls (5% of total). Antibodies against CASPR2, LGI1, and GAD were also identified in 3.3%, 8.3%, and 10% of epilepsy patients, respectively (
Figure 1).
None of the epilepsy patients or controls tested positive for onconeural antibodies, except for 6 epilepsy cases, 1 MS case, and 3 SLE cases showing anti-GAD positivity detected by IIF-TBA and immunoblotting (
Figure 3).
There was no significant difference in the incidence of studied autoantibodies between male and female epilepsy patients (
Table 2). However, a notably higher incidence of positive autoantibodies was observed in patients with focal epilepsy compared to those with generalized epilepsy (p < 0.01;
Table 2).
5. Discussion
Previous studies have highlighted the presence of autoantibodies against NMDAR
| [7] | Zhongqin Chena, Jintao Zhoua, Dengchang Wu, Caihong Ji, Benyan Luo, Kang Wang. Altered executive control network connectivity in anti-NMDA receptor encephalitis. Annals of Clinical and Translational Neurology 2022; 9(1): 30–40. https://doi.org/10.1002/acn3.51487 |
[7]
and GAD
| [8] | Anna R Tröscher, Katharina M Mair, Laia Verdú de Juan, Ulrike Köck, Anja Steinmaurer, Hartmut Baier, et al. Temporal lobe epilepsy with GAD antibodies: neurons killed by T cells not by complement membrane attack complex. Brain, Volume 146, Issue 4, April 2023, Pages 1436–1452. https://doi.org/10.1093/brain/awac404 |
[8]
in cross-sectional cohorts of patients with epilepsy, particularly in well-defined epileptic syndromes and those with suspected pre-existing neurological autoimmunity
. More recently, investigations into CASPR2
| [9] | Emilio R. Garrido Sanabria, Anza Zahid, Jeffrey Britton, Gregory J. Kraus, Alfonso Sebastian López-Chiriboga, Anastasia Zekeridou, et al. CASPR2-IgG-associated autoimmune seizures. First published: 15 January 2022. https://doi.org/10.1111/epi.17164 |
[9]
and LGI1
| [10] | Kelsey M. Smith, Divyanshu Dubey, Greta B. Liebo, Eoin P. Flanagan, Jeffrey W. Britton. Clinical Course and Features of Seizures Associated with LGI1-Antibody Encephalitis. First published July 7, 2021, https://doi.org/10.1212/WNL.0000000000012465 |
[10]
antibodies have expanded our understanding within the autoimmune epilepsy population, with limited studies focusing on pediatric cases of limbic encephalitis and status epilepticus
| [11] | Haberlandt E, Bast T, Ebner A, Holthausen H, Kluger G, Kravljanac R, et al. Limbic encephalitis in children and adolescents. Arch Dis Child 2011 96: 186–191. https://doi.org/10.1136/adc.2010.183897 |
[11]
.
In the study, antibodies in a consecutive, unselected cohort of epilepsy patients were systematically examined. A significantly higher incidence of NMDAR, CASPR2, LGI1, and GAD antibodies was observed compared to healthy and diseased controls. Specifically, 28 out of 60 epilepsy patients (47%) tested positive for antibodies against these neuronal antigens.
Notably, none of the patients in our this study exhibited clinical evidence of limbic encephalitis (LE) or anti-NMDAR encephalitis, emphasizing that several neurologic autoantibodies associated with subacute onset encephalopathies may also precipitate sporadic epilepsy, corroborating previous reports in young patients with unexplained-onset epilepsy
| [12] | Niehusmann P, Dalmau J, Rudlowski C, Vincent A, Elger CE, Rossi JE, et al. Diagnostic value of N-methyl-D-aspartate receptor antibodies in women with new-onset epilepsy. Arch Neurol 2009 66: 458–464. https://doi.org/10.1001/archneurol.2009.5 |
[12]
. Among the six patients positive for anti-GAD antibodies, all had focal epilepsy, evenly split between men and women, consistent with existing literature
and recent findings linking anti-GAD antibodies to temporal lobe epilepsy and mild cognitive impairments
| [14] | Liimatainen S, Peltola M, Sabater L, Fallah M, Kharazmi E, Haapala AM, et al. Clinical significance of glutamic acid decarboxylase antibodies in patients with epilepsy. Epilepsia 2010 51: 760–767. https://doi.org/10.1111/j.1528-1167.2009.02325.x |
| [15] | Lin Nan, Bai Lin, Liu Qing, Chen Jianhua, Ren Haitao, Guan Hongzhi et al. Seizure semiology and predictors of outcomes in Chinese patients with glutamic acid decarboxylase antibody-associated neurological syndrome. BMC Neurology 2023 volume 23, Article number: 149. https://doi.org/10.1186/s12883-023-03182-x |
| [16] | Balagopal K, Shenoy SG, Dutta D, et al. Autoimmune limbic encephalitis associated with glutamic acid decarboxylase antibodies. J Evolution Med Dent Sci 2021; 10(28): 2131-2133, https://doi.org/10.14260/jemds/2021/435 |
[14-16]
.
After anti-NMDAR antibodies, anti-GAD emerged as the second most prevalent autoantibody in our analysis. This aligns with historical data linking anti-GAD antibodies to drug-resistant epilepsies that do not meet criteria for limbic encephalitis
, a criterion consistent with our study's selection criteria.
Our findings also revealed that 7 out of 60 patients diagnosed with epilepsy—both focal and generalized—tested positive for anti-CASPR2 (3.3%) and anti-LGI1 (8.3%) antibodies, consistent with the relative prevalence observed in other studies. While generalized epilepsies are often genetically rooted, the potential overlap between genetic epilepsy and autoimmune mechanisms warrants further investigation. The International League Against Epilepsy (ILAE) has acknowledged this evolving understanding in its recent classification updates, recognizing "Immune" as an etiological factor in epilepsy for the first time
| [18] | Scheffer IE, Berkovic S, Capovilla G, et al. ILAE classification of the epilepsies: position paper of the ILAE commission for classification and terminology. Epilepsia 2017; 58: 512-521. https://doi.org/10.1111/epi.13709 |
[18]
.
Anti-NMDAR encephalitis, the most common autoimmune encephalitis associated with anti-neuronal surface antibodies (ANSA)
, underscores the autoimmune etiology within the broader spectrum of neurological disorders. A prospective, multicenter study supports autoimmune disorders as the third most prevalent cause of encephalitis after viral infections and acute disseminated encephalomyelitis
| [20] | Granerod J, Ambrose HE, Davies NW, et al. Causes of encephalitis and differences in their clinical presentations in England: a multicentre, population-based prospective study. Lancet Infect Dis 2010; 10: 835-44. https://doi.org/10.1016/S1473-3099(10)70222-X |
[20]
. Diagnostic confirmation of anti-NMDAR encephalitis hinges on cerebrospinal fluid antibody detection against the GluN1 subunit of NMDAR, given the less reliable serum tests that yield false negatives in up to 14% of cases
| [21] | Gresa-Arribas N, Titulaer MJ, Torrents A, et al. Antibody titres at diagnosis and during follow-up of anti-NMDA receptor encephalitis: a retrospective study. Lancet Neurol 2014; 13: 167-77. https://doi.org/10.1016/S1474-4422(13)70282-5 |
[21]
. Conversely, cases presenting with positive serum and negative cerebrospinal fluid antibodies should be carefully re-evaluated for accuracy
| [22] | Gleichman AJ, Spruce LA, Dalmau J, et al. Anti-NMDA receptor encephalitis antibody binding Is dependent on amino acid identity of a small region within the GluN1 amino terminal domain. J Neurosci 2012; 32: 11082-11094. https://doi.org/10.1523/JNEUROSCI.0064-12.2012 |
| [23] | Dalmau J, Lancaster E, Martinez-Hernandez E, et al. Clinical experience and laboratory investigations in patients with antiNMDAR encephalitis. Lancet Neurol 2011; 10: 63-74. https://doi.org/10.1016/S1474-4422(10)70253-2 |
[22, 23]
.
The anti-LGI1 antibody, previously identified as anti-VGKC, underscores the complexity of antibody characterization. While initially detected via radioimmunoassay targeting VGKC, subsequent studies revealed LGI1 and CASPR2 as true antigenic epitopes. This realization prompted the reclassification to anti-VGKC complex antibodies, urging a shift towards direct antigen naming rather than the VGKC complex. Such nuances highlight the importance of updated methodologies, such as cell-based assays (CBA), in accurately diagnosing autoimmune epilepsies
| [24] | van Sonderen A, Schreurs MW, Wirtz PW, et al. From VGKC to LGI1 and Caspr2 encephalitis: the evolution of a disease entity over time. Autoimmun Rev 2016; 15: 970-974. https://doi.org/10.1016/j.autrev.2016.07.018 |
| [25] | Lang B, Makuch M, Moloney T, et al. Intracellular and nonneuronal targets of voltage-gated potassium channel complex antibodies. J Neurol Neurosurg Psychiatry 2017; 88: 353-361. https://doi.org/10.1136/jnnp-2016-314758 |
[24, 25]
.
This study's antibody incidence data offer insights for future research directions and clinical considerations. Given the variability in antibody types and detection methodologies across studies, standardized protocols for neuronal autoantibody testing are crucial to obtain accurate prevalence estimates and improve clinical management strategies for patients with epilepsy of unknown origin.
In summary, our consecutive prospective study of epilepsy patients revealed a notable proportion with detectable neuronal antibodies in serum and cerebrospinal fluid, indicating a potential autoimmune basis. This study underscores the under-recognition and prevalence of autoimmune epilepsy. However, limitations, such as the unavailability of glycine receptor antibody testing and potential under-recognition of certain neurological autoantibodies, warrant further investigation to refine our understanding and clinical management of autoimmune epilepsy.
6. Conclusion
In conclusion, our study identifies antibodies against neuronal receptors (NMDAR), VGKC-associated proteins (LGI1, CASPR2), and intracellular antigens (GAD65) in the serum and cerebrospinal fluid of epilepsy patients, indicating potential responsiveness to immune-modulatory treatments. Future research should focus on prospective cohorts of newly diagnosed epilepsy patients to further elucidate the role of autoantibodies in epilepsy pathophysiology, aiming to enhance diagnostic accuracy and explore alternative treatment options, such as immunotherapies.
7. Recommendations
Based on this study, several recommendations can be made:
1. Enhanced Screening Protocols: Implement enhanced screening protocols to routinely test for neuronal antibodies (NMDAR, LGI1, CASPR2, GAD65) in both serum and cerebrospinal fluid of epilepsy patients, especially those with refractory epilepsy or atypical presentations.
2. Early Diagnosis and Intervention: Encourage early diagnosis by incorporating autoantibody testing into the diagnostic workup of epilepsy patients, potentially leading to earlier intervention with immunomodulatory therapies.
3. Educational Initiatives: Conduct educational initiatives for healthcare providers to increase awareness of autoimmune etiologies in epilepsy and the clinical significance of neuronal antibodies.
4. Collaborative Research Efforts: Foster collaborative efforts between neurologists, immunologists, and researchers to further investigate the pathophysiological roles of neuronal antibodies in epilepsy and develop targeted treatment strategies.
5. Longitudinal Studies: Support longitudinal studies to monitor the efficacy and long-term outcomes of immunomodulatory therapies in epilepsy patients positive for neuronal antibodies.
Implementing these recommendations can potentially improve diagnostic accuracy, optimize treatment outcomes, and advance our understanding of autoimmune contributions to epilepsy.
Table 1. Presence of neuronal autoantibodies in cases and controls.
| n | a-NMDAR (CBA) | a-AMPAR (CBA) | a-CASPR2 (CBA) | a-LGI1 (CBA) | a-DPPX (CBA) | a-GABAb (CBA) | a-GAD (IIF-TBA-IT) | Total, Ac + | p |
Cases | | | | | | | | | | |
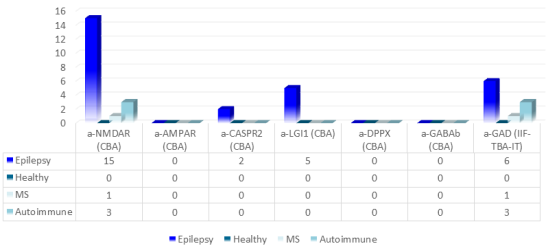
Epilepsy | 60 | 15 | 0 | 2 | 5 | 0 | 0 | 6 | 28 | |
Controls | | | | | | | | | | |
Healthy | 30 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | <0,001* |
MS | 30 | 1 | 0 | 0 | 0 | 0 | 0 | 1 | 2 | <0,001* |
Autoimmune | 20 | 3 | 0 | 0 | 0 | 0 | 0 | 3 | 6 | <0,01* |
Results are expressed as the number of samples showing a positive titer. Statistical comparisons (*total positive antibodies in cases vs controls) were conducted using the chi-square test or Fisher's exact test as appropriate.
Detected autoantibodies include: NMDAR, N-methyl-D-aspartate receptor; AMPAR, alpha-amino-3-hydroxy-5-methyl-4-isoxazolepropionic acid receptor; CASPR2, contactin-associated protein-like 2; LGI1, leucine-rich glioma inactivated 1 protein; DPPX, dipeptidyl-peptidase-like protein 6; GABAb, gamma-aminobutyric acid type B receptor; GAD, glutamic acid decarboxylase.
Methods for antibody determination were CBA: cell-based assay, IIF-TBA: immunofluorescence tissue-based assay, IT: immunotransfer; MS, multiple sclerosis; p, p-value. -n Number of cases and controls. -Total: Number of positive autoantibodies. -Autoimmune: Controls from other autoimmune diseases (systemic lupus erythematosus and Sjögren's syndrome).
This table provides a structured overview of the presence of specific neuronal autoantibodies in different groups of patients and controls, highlighting significant findings through statistical comparisons.
Table 2. Incidence of neuronal autoantibodies by demographic and clinical characteristics.
| n | a-NMDAR (CBA) | a-AMPAR (CBA) | a-CASPR2 (CBA) | a- LGI1 (CBA) | a-DPPX (CBA) | a-GABAb (CBA) | a-GAD (IIF-TBA-IT) | Total Ac + | p |
Sex | | | | | | | | | | ns |
Male | 33 | 8 (24%) | 0 (0%) | 1 (3%) | 3 (9%) | 0 (0%) | 0 (0%) | 3 (9%) | 15 (45%) |
Female | 27 | 7 (26%) | 0 (0%) | 1 (4%) | 2 (7%) | 0 (0%) | 0 (0%) | 3 (11%) | 13 (48%) |
Epilepsy Type | | | | | | | | | | |
Generalized | 20 | 5 (25%) | 0 (0%) | 0 (0%) | 1 (5%) | 0 (0%) | 0 (0%) | 1 (5%) | 7 (35%) | <0,01* |
Focal | 40 | 10 (25%) | 0 (0%) | 2 (5%) | 4 (10%) | 0 (0%) | 0 (0%) | 5 (12%) | 21 (52%) |
Results are expressed as the number of samples showing a positive titer in clinical cohorts. Statistical comparisons were performed using the chi-square test or Fisher's exact test as appropriate. -ns: not significant, *: statistically significant.
Detected autoantibodies include: NMDAR, N-methyl-D-aspartate receptor; AMPAR, alpha-amino-3-hydroxy-5-methyl-4-isoxazolepropionic acid receptor; CASPR2, contactin-associated protein-like 2; LGI1, leucine-rich glioma inactivated 1 protein; DPPX, dipeptidyl-peptidase-like protein 6; GABAb, gamma-aminobutyric acid type B receptor; GAD, glutamic acid decarboxylase.
Methods for antibody determination were CBA: cell-based assay, IIF-TBA: immunofluorescence tissue-based assay, IT: immunotransfer; p, p-value. -n Number of cases. -Total: Number of positive autoantibodies.
This table summarizes the incidence of specific neuronal autoantibodies categorized by sex and epilepsy type, demonstrating significant associations through statistical analysis.
Figure 1. Neuronal autoantibodies in cases and controls.
Patients with epilepsy (n = 60), disease controls [multiple sclerosis (MS) n = 30, autoimmune diseases, systemic lupus erythematosus (SLE) + Sjögren's syndrome (SS) n = 20], and healthy controls (n = 30) were analyzed for autoantibodies against various neuronal proteins. The figure depicts the results of autoantibody detection against NMDAR, N-methyl-D-aspartate receptor; AMPAR, alpha-amino-3-hydroxy-5-methyl-4-isoxazolepropionic acid receptor; CASPR2, contactin-associated protein-like 2; LGI1, leucine-rich glioma inactivated 1 protein; DPPX, dipeptidyl-peptidase-like protein 6; GABAb, gamma-aminobutyric acid type B receptor, by cell-based assay (CBA), and GAD, glutamic acid decarboxylase by immunoblot and immunofluorescence tissue-based assay (IIF-TBA).
This description summarizes the autoantibody detection against various neuronal proteins in patients with epilepsy and control groups, indicating the methodology used for each antibody type.
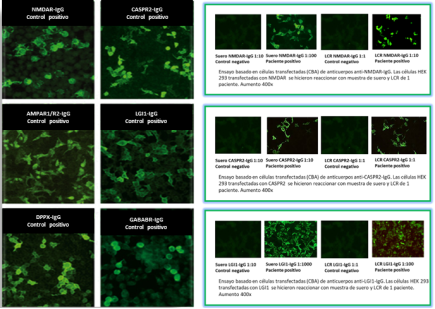
Figure 2. Autoimmune encephalitis mosaic. Cell-based assay.
Mono-specific determination of autoantibodies targeting neuronal surface antigens using indirect immunofluorescence assay based on transfected cells presenting the relevant antigens in their authentic or conformational form. Different transfected cellular substrates can be combined in multiplex.
The left panel displays positive controls for detecting antibodies against NMDAR, N-methyl-D-aspartate receptor; AMPAR, alpha-amino-3-hydroxy-5-methyl-4-isoxazolepropionic acid receptor; CASPR2, contactin-associated protein-like 2; LGI1, leucine-rich glioma inactivated 1 protein; DPPX, dipeptidyl-peptidase-like protein 6; GABAb, gamma-aminobutyric acid type B receptors. On the right, images of positive immunofluorescence from three patients are shown.
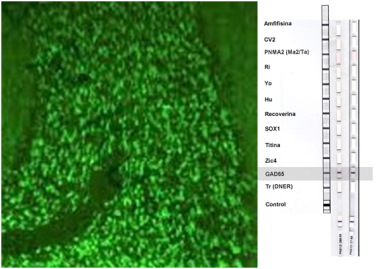
Figure 3. Anti-glutamic acid decarboxylase (GAD) autoantibodies.
(a) Immunofluorescence findings in a case of epilepsy associated with anti-GAD antibodies. Micrograph showing immunofluorescence using patient serum diluted 1:100 on cerebellum (400x magnification). The typical fluorescence pattern of anti-GAD antibodies shows prominent staining in the granular cell layer, unlike anti-amphiphysin antibodies, which do not stain the molecular layer.
(b) Anti-GAD detected by immunoblot in serum and cerebrospinal fluid (CSF) of the same patient. Serum dilution 1:100, CSF dilution 1:2. CV2: CV2/collapsin response mediator protein (CRMP) 5; PNMA2/Ma2: paraneoplastic Ma antigen family (PNMA) represented by at least fifteen family members, with PNMA1-3 associated with paraneoplastic disorder; Ri: 55 and 80 kDa proteins named Nova-1 and Nova-2, involved in pre-mRNA regulation; Yo: cytoplasmic proteins in Purkinje cells of cerebellum, 34 and 62 kDa; Hu: RNA-binding protein family (Hu-D, Hu-C, and Hel N1), 35-40 kDa, located in nuclei and cytoplasm of all neurons and also in tumor cells; SOX1: antigen localized in Bergmann glial cell nuclei of adult cerebellum; Zic4: proteins in granular layer nuclei, part of a zinc-finger protein family crucial in nervous system (NS) development; GAD65: glutamic acid decarboxylase, Tr (DNER): antigen expressed in Purkinje cell cytoplasm, axons, and dendrites.
Abbreviations
GlyR | Anti-glycine Receptor Antibodies |
AMPAR | α-amino-3-Hydroxy-5-Methyl-4- Isoxazolepropionic Acid Receptor |
anti- Amphiphysin | Antibodies Against a 128 kDa Protein Called Amphiphysin |
Anti-ANNA-3 | Anti-Neuronal Nuclear Type 3 (ANNA-3) Antibodies |
anti-CV2/CRMP5 | Antibodies Against CV2/Collapsin Response Mediator Protein 5 |
anti-Hu or ANNA-1 | Antibodies Against RNA-binding Protein Family (Hu-D, Hu-C, and Hel N1) |
anti-Ma2/PNMA2 | Antibodies Against Brain and Testis Proteins Including Ma1, Ma2, and Others |
anti-NSA | Anti-Neuronal Surface Antigen Antibodies |
Anti-PCA-2 | Antibodies Identified in a Small Group of Patients with Paraneoplastic Cerebellar Degeneration (PCD) Associated with Small-Cell Lung Cancer |
anti-Ri or ANNA-2 | Antibodies Against Nova-1 and Nova-2 Proteins (55 and 80 kDa) |
Anti-SOX1 | Anti-Glial Nuclear (AGNA) Antibodies |
anti-Tr (PCA-Tr) | Antibodies Associated with Paraneoplastic Cerebellar Degeneration (PCD) and Hodgkin's Disease |
anti-Yo | Antibodies Against Cytoplasmic Proteins of Purkinje Cells (34 and 62 kDa) |
Anti-Zic4 | Antibodies Against Zic4 Proteins |
AON | Onconeural Antibodies |
CASPR2 | Contactin-Associated Protein 2 |
CBA | Cell-Based Assay |
CDFB | Faciobrachial Dystonic Seizures |
AE | Autoimmune Encephalitis |
LE | Limbic Encephalitis |
MS | Multiple Sclerosis |
GABABR | γ-aminobutyric Acid B Receptor |
GAD | Glutamic Acid Decarboxylase |
GLY-Rs | Glycine Receptors |
IIF-TBA | Indirect Immunofluorescence Assay Using Primate Cerebellar Tissue |
ILAE | International League Against Epilepsy |
Kv1 | Potassium Voltage-Gated Channel Subfamily A member 1 |
CSF | Cerebrospinal Fluid |
SLE | Systemic Lupus Erythematosus |
LGI1 | Leucine-rich Glioma-Inactivated Protein 1 |
NMDAR | N-methyl-D-Aspartate receptor |
PBS | Phosphate-Buffered saline |
NS | Nervous System |
PNS | Paraneoplastic Neurological Syndromes |
VGKC | Voltage-Gated Potassium Channel Complex |
Author Contributions
Silvia Graciela Ramos: Conceptualization, Data curation, Formal Analysis, Investigation, Methodology, Supervision, Validation, Writing – original draft Writing – review & editing
Viviana Novoa: Conceptualization, Investigation, Supervision, Writing – review & editing
Claudio Aranda: Conceptualization, Supervision, Visualization
Conflicts of Interest
The authors declare no conflicts of interest.
References
| [1] |
Vincent A, Buckley C, Schott JM, Baker I, Dewar BK, Detert N, et al. Potassium channel antibody-associated encephalopathy: a potentially immunotherapy-responsive form of limbic encephalitis. Brain 2004; 127: 701–712.
https://doi.org/10.1093/brain/awh077
|
| [2] |
Irani SR, Michell AW, Lang B, Pettingill P, Waters P, Johnson MR, et al. Fachiobrachial dystonic seizures precede Lgi1 antibody limbic encephalitis. Ann Neurol 2011; 69: 892–900.
https://doi.org/10.1002/ana.22307
|
| [3] |
Buckley C, Oger J, Clover L, Tüzün E, Carpenter K, Jackson M, et al. Potassium channel antibodies in two patients with reversible limbic encephalitis. Ann Neurol 2001 50: 73–78.
https://doi.org/10.1002/ana.1097
|
| [4] |
Quek AML, Britton JW, McKeon A, So E, Lennon VA, Shin C, et al. Autoimmune epilepsy: clinical characteristics and response to immunotherapy. Arch Neurol 2012 69: 582–593.
https://doi.org/10.1001/archneurol.2011.2985
|
| [5] |
Kwan P, Sills GJ, Kelly K, Butler E, Brodie MJ. Glutamic acid decarboxylase autoantibodies in controlled and uncontrolled epilepsy: a pilot study. Epilepsy Res 2000 42: 191–195.
https://doi.org/10.1016/s0920-1211(00)00180-7
|
| [6] |
Vincent A, Crino PB. Systemic and neurologic autoimmune disorders associated with seizures or epilepsy. Epilepsia 2011 52: 12–17.
https://doi.org/10.1111/j.1528-1167.2011.03030.x
|
| [7] |
Zhongqin Chena, Jintao Zhoua, Dengchang Wu, Caihong Ji, Benyan Luo, Kang Wang. Altered executive control network connectivity in anti-NMDA receptor encephalitis. Annals of Clinical and Translational Neurology 2022; 9(1): 30–40.
https://doi.org/10.1002/acn3.51487
|
| [8] |
Anna R Tröscher, Katharina M Mair, Laia Verdú de Juan, Ulrike Köck, Anja Steinmaurer, Hartmut Baier, et al. Temporal lobe epilepsy with GAD antibodies: neurons killed by T cells not by complement membrane attack complex. Brain, Volume 146, Issue 4, April 2023, Pages 1436–1452.
https://doi.org/10.1093/brain/awac404
|
| [9] |
Emilio R. Garrido Sanabria, Anza Zahid, Jeffrey Britton, Gregory J. Kraus, Alfonso Sebastian López-Chiriboga, Anastasia Zekeridou, et al. CASPR2-IgG-associated autoimmune seizures. First published: 15 January 2022.
https://doi.org/10.1111/epi.17164
|
| [10] |
Kelsey M. Smith, Divyanshu Dubey, Greta B. Liebo, Eoin P. Flanagan, Jeffrey W. Britton. Clinical Course and Features of Seizures Associated with LGI1-Antibody Encephalitis. First published July 7, 2021,
https://doi.org/10.1212/WNL.0000000000012465
|
| [11] |
Haberlandt E, Bast T, Ebner A, Holthausen H, Kluger G, Kravljanac R, et al. Limbic encephalitis in children and adolescents. Arch Dis Child 2011 96: 186–191.
https://doi.org/10.1136/adc.2010.183897
|
| [12] |
Niehusmann P, Dalmau J, Rudlowski C, Vincent A, Elger CE, Rossi JE, et al. Diagnostic value of N-methyl-D-aspartate receptor antibodies in women with new-onset epilepsy. Arch Neurol 2009 66: 458–464.
https://doi.org/10.1001/archneurol.2009.5
|
| [13] |
Irani S, Bien C, Lang B. Autoimmune epilepsies. Curr Opin Neurol 2011b 24: 146–153.
https://doi.org/10.1097/WCO.0b013e3283446f05
|
| [14] |
Liimatainen S, Peltola M, Sabater L, Fallah M, Kharazmi E, Haapala AM, et al. Clinical significance of glutamic acid decarboxylase antibodies in patients with epilepsy. Epilepsia 2010 51: 760–767.
https://doi.org/10.1111/j.1528-1167.2009.02325.x
|
| [15] |
Lin Nan, Bai Lin, Liu Qing, Chen Jianhua, Ren Haitao, Guan Hongzhi et al. Seizure semiology and predictors of outcomes in Chinese patients with glutamic acid decarboxylase antibody-associated neurological syndrome. BMC Neurology 2023 volume 23, Article number: 149.
https://doi.org/10.1186/s12883-023-03182-x
|
| [16] |
Balagopal K, Shenoy SG, Dutta D, et al. Autoimmune limbic encephalitis associated with glutamic acid decarboxylase antibodies. J Evolution Med Dent Sci 2021; 10(28): 2131-2133,
https://doi.org/10.14260/jemds/2021/435
|
| [17] |
Graus, F.; Saiz, A.; Dalmau, J. GAD antibodies in neurological disorders—Insights and challenges. Nat. Rev. Neurol. 2020, 16, 353–365.
https://doi.org/10.1038/s41582-020-0359-x
|
| [18] |
Scheffer IE, Berkovic S, Capovilla G, et al. ILAE classification of the epilepsies: position paper of the ILAE commission for classification and terminology. Epilepsia 2017; 58: 512-521.
https://doi.org/10.1111/epi.13709
|
| [19] |
Dalmau J, Graus F. Antibody-mediated encephalitis. N Engl J Med 2018; 378: 840-851.
https://doi.org/10.1056/NEJMra1708712
|
| [20] |
Granerod J, Ambrose HE, Davies NW, et al. Causes of encephalitis and differences in their clinical presentations in England: a multicentre, population-based prospective study. Lancet Infect Dis 2010; 10: 835-44.
https://doi.org/10.1016/S1473-3099(10)70222-X
|
| [21] |
Gresa-Arribas N, Titulaer MJ, Torrents A, et al. Antibody titres at diagnosis and during follow-up of anti-NMDA receptor encephalitis: a retrospective study. Lancet Neurol 2014; 13: 167-77.
https://doi.org/10.1016/S1474-4422(13)70282-5
|
| [22] |
Gleichman AJ, Spruce LA, Dalmau J, et al. Anti-NMDA receptor encephalitis antibody binding Is dependent on amino acid identity of a small region within the GluN1 amino terminal domain. J Neurosci 2012; 32: 11082-11094.
https://doi.org/10.1523/JNEUROSCI.0064-12.2012
|
| [23] |
Dalmau J, Lancaster E, Martinez-Hernandez E, et al. Clinical experience and laboratory investigations in patients with antiNMDAR encephalitis. Lancet Neurol 2011; 10: 63-74.
https://doi.org/10.1016/S1474-4422(10)70253-2
|
| [24] |
van Sonderen A, Schreurs MW, Wirtz PW, et al. From VGKC to LGI1 and Caspr2 encephalitis: the evolution of a disease entity over time. Autoimmun Rev 2016; 15: 970-974.
https://doi.org/10.1016/j.autrev.2016.07.018
|
| [25] |
Lang B, Makuch M, Moloney T, et al. Intracellular and nonneuronal targets of voltage-gated potassium channel complex antibodies. J Neurol Neurosurg Psychiatry 2017; 88: 353-361.
https://doi.org/10.1136/jnnp-2016-314758
|
Cite This Article
-
-
@article{10.11648/j.iji.20241202.12,
author = {Silvia Graciela Ramos and Viviana Novoa and Claudio Aranda},
title = {Link Between Autoimmunity and Epilepsy: Neuronal Autoantibodies
},
journal = {International Journal of Immunology},
volume = {12},
number = {2},
pages = {30-37},
doi = {10.11648/j.iji.20241202.12},
url = {https://doi.org/10.11648/j.iji.20241202.12},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.iji.20241202.12},
abstract = {Introduction: Autoimmune epilepsy remains under-recognized, and its true incidence remains uncertain. Objective: This study aimed to determine the prevalence of neuronal autoantibodies in patients with epilepsy of unknown etiology. Materials and Methods: An observational, longitudinal, prospective, and analytical study was conducted to assess the presence of autoantibodies associated with autoimmune encephalitis, glutamic acid decarboxylase-65 (GAD65), and onconeural antibodies in the serum and cerebrospinal fluid of consecutive patients with epilepsy of unknown etiology. Results: Sixty patients and 80 controls (30 healthy individuals, 30 with multiple sclerosis, 10 with systemic lupus erythematosus, and 10 with Sjögren's syndrome) were included to detect neuronal antibodies. Among epilepsy patients, 28 out of 60 (47%) tested positive for antibodies against N-methyl-D-aspartate receptor (NMDAR), contactin-associated protein 2 (CASPR2), leucine-rich glioma-inactivated 1 (LGI1), and glutamic acid decarboxylase (GAD), which was significantly higher (p < 0.001) than in the combined control cohort. No onconeural antibodies were detected in epilepsy patients except for 6 cases of epilepsy, 1 case of multiple sclerosis, and 3 cases of lupus with positive GAD by immunofluorescence assay and immunoblotting. There was no significant difference in antibody incidence between male and female epilepsy patients. The incidence of positive autoantibodies was significantly higher in patients with focal epilepsy compared to those with generalized epilepsy (p < 0.01). Conclusions: The findings indicate the presence of antibodies against NMDAR, VGKC-associated proteins (LGI1, CASPR2), and intracellular antigens (GAD65) in the serum and cerebrospinal fluid of patients with epilepsy, suggesting an autoimmune etiology. These results underscore the need for further research to elucidate the role of autoantibodies in epilepsy pathogenesis and to explore immunotherapeutic interventions.
},
year = {2024}
}
 Copy
|
Copy
|
 Download
Download
-
TY - JOUR
T1 - Link Between Autoimmunity and Epilepsy: Neuronal Autoantibodies
AU - Silvia Graciela Ramos
AU - Viviana Novoa
AU - Claudio Aranda
Y1 - 2024/07/23
PY - 2024
N1 - https://doi.org/10.11648/j.iji.20241202.12
DO - 10.11648/j.iji.20241202.12
T2 - International Journal of Immunology
JF - International Journal of Immunology
JO - International Journal of Immunology
SP - 30
EP - 37
PB - Science Publishing Group
SN - 2329-1753
UR - https://doi.org/10.11648/j.iji.20241202.12
AB - Introduction: Autoimmune epilepsy remains under-recognized, and its true incidence remains uncertain. Objective: This study aimed to determine the prevalence of neuronal autoantibodies in patients with epilepsy of unknown etiology. Materials and Methods: An observational, longitudinal, prospective, and analytical study was conducted to assess the presence of autoantibodies associated with autoimmune encephalitis, glutamic acid decarboxylase-65 (GAD65), and onconeural antibodies in the serum and cerebrospinal fluid of consecutive patients with epilepsy of unknown etiology. Results: Sixty patients and 80 controls (30 healthy individuals, 30 with multiple sclerosis, 10 with systemic lupus erythematosus, and 10 with Sjögren's syndrome) were included to detect neuronal antibodies. Among epilepsy patients, 28 out of 60 (47%) tested positive for antibodies against N-methyl-D-aspartate receptor (NMDAR), contactin-associated protein 2 (CASPR2), leucine-rich glioma-inactivated 1 (LGI1), and glutamic acid decarboxylase (GAD), which was significantly higher (p < 0.001) than in the combined control cohort. No onconeural antibodies were detected in epilepsy patients except for 6 cases of epilepsy, 1 case of multiple sclerosis, and 3 cases of lupus with positive GAD by immunofluorescence assay and immunoblotting. There was no significant difference in antibody incidence between male and female epilepsy patients. The incidence of positive autoantibodies was significantly higher in patients with focal epilepsy compared to those with generalized epilepsy (p < 0.01). Conclusions: The findings indicate the presence of antibodies against NMDAR, VGKC-associated proteins (LGI1, CASPR2), and intracellular antigens (GAD65) in the serum and cerebrospinal fluid of patients with epilepsy, suggesting an autoimmune etiology. These results underscore the need for further research to elucidate the role of autoantibodies in epilepsy pathogenesis and to explore immunotherapeutic interventions.
VL - 12
IS - 2
ER -
Copy
|
Download