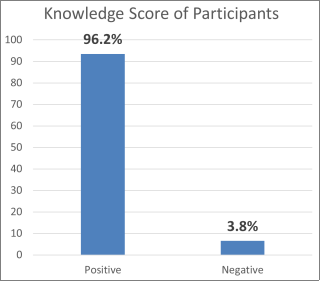
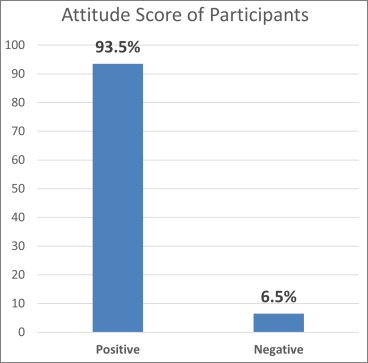
Immunization is a proven tool for controlling and eliminating life-threatening infectious diseases such as Tuberculosis, Poliomyelitis, Haemophilus Influenza type b (HIB), Diphtheria, Pertusis, Tetanus and Hepatitis B, neonatal tetanus yellow fever, measles, cerebrospinal meningitis and is estimated to avert between 2 and 3 million deaths each year. The objective of this study is to appraise routine immunization coverage among children 0-2 years in Akure South Local Government Area of Ondo State. This is a descriptive cross-sectional study, designed to appraise routine immunization coverage among children 0-2 years in Akure South Local Government Area of Ondo State. The study focused on children 0-2 years. Majority 102 (25.2%) of the respondents were within the age range of 25-29 years, 82 (20.5%) were >39 years. 314 (78.5%) were Yorubas. 385 (96.2%) had good knowledge while 15 (3.8%) had poor knowledge. 374 (93.5%) of the women have positive attitude while 26 (6.5%) of them have negative attitude. Most of the respondents, 391 (97.8%) of the respondents reported that they have taken their child to the health facility for immunization and 232 (58%) have taken their child to 4-5 immunization sessions. Based on the findings of the present study, it could be concluded that very few of the women had poor knowledge of childhood immunization, majority of the women had positive attitude score and practice of childhood immunization, practice of childhood immunization is quite high, and the uptake of childhood immunization is quite high.
| Published in | International Journal of Immunology (Volume 12, Issue 2) |
| DOI | 10.11648/j.iji.20241202.11 |
| Page(s) | 19-29 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2024. Published by Science Publishing Group |
Immunization, Coverage, Knowledge, Attitude, Practice
VARIABLES | FREQUENCY (n=400) | PERCENTAGE (%) |
|---|---|---|
AGE | ||
<25 | 78 | 19.5 |
25-29 | 102 | 25.2 |
30-34 | 78 | 19.5 |
35-39 | 60 | 15 |
>39 | 82 | 20.5 |
ETHNICITY | ||
YORUBA | 314 | 78.5 |
IBO | 57 | 14.3 |
HAUSA | 19 | 4.8 |
OTHERS | 10 | 2.5 |
RELIGION | ||
CHRISTIANITY | 342 | 85.5 |
ISLAM | 44 | 11.0 |
TRADITIONAL | 13 | 3.3 |
OTHERS | 1 | 0.3 |
MARITAL STATUS | ||
MARRIED | 295 | 73.8 |
WIDOWED | 27 | 6.8 |
DIVORCED | 27 | 6.8 |
SEPARATED | 51 | 12.8 |
EDUCATIONAL LEVEL | ||
NO FORMAL EDUCATION | 39 | 9.8 |
PRIMARY | 59 | 14.8 |
SECONDARY | 189 | 47.3 |
TERTIARY | 113 | 28.3 |
TYPES OF OCCUPATION | ||
FARMING/ARTISAN/PETTY TRADING | 149 | 37.3 |
BUSINESS | 108 | 27.0 |
CIVIL SERVANTS/PROFESSIONALS | 104 | 26.0 |
OTHERS | 39 | 9.8 |
NUMBER OF CHILDREN | ||
0 | 9 | 2.3 |
1-5 | 345 | 86.3 |
>5 | 46 | 11.5 |
VARIABLES | FREQUENCY (n=400) | PERCENTAGE (%) |
|---|---|---|
AGE OF LAST CHILD | ||
No child | 9 | 2.3 |
<1 years | 145 | 36.3 |
1-2 years | 246 | 61.5 |
SEX | ||
Female | 293 | 73.3 |
Male | 107 | 26.8 |
Position of Child | ||
1-2 | 166 | 41.5 |
3-4 | 154 | 38.5 |
>4 | 80 | 20 |
VARIABLE | FREQUENCY (n=400) | PERCENTAGE (%) |
|---|---|---|
What is immunization? | ||
Means of preventing diseases/infections | 314 | 78.5 |
Means of treating diseases/infections | 71 | 17.7 |
No response | 15 | 3.8 |
What type of vaccines do you know? | ||
OPV and IPV | 381 | 95.3 |
Measles | 396 | 99 |
HBV | 274 | 68.5 |
PCV | 142 | 35.5 |
Yellow fever | 370 | 92.5 |
Td | 56 | 14 |
Penta | 129 | 32.3 |
BCG | 357 | 89.3 |
Do immunizations protect babies against serious diseases. | ||
Yes | 394 | 98.5 |
No | 6 | 1.5 |
What are the benefits of immunization? | ||
It prevents diseases. | 368 | 92 |
It improves the body antigens. | 310 | 77.5 |
It improves living. | 254 | 63.5 |
It serves as a balanced diet. | 54 | 13.5 |
None of the above | 5 | 1.3 |
VARIABLE | FREQUENCY (n=400) | PERCENTAGE (%) |
|---|---|---|
I may not take my child for immunization. | ||
Agree | 38 | 9.5 |
Strongly agree. | 14 | 3.5 |
Disagree | 317 | 79.3 |
Strongly disagree | 31 | 7.8 |
My spouse doesn’t support immunization. | ||
Agree | 24 | 6 |
Strongly agree | 10 | 2.5 |
Disagree | 157 | 39.3 |
Strongly disagree | 191 | 47.3 |
I prefer traditional medicine to immunization. | ||
Agree | 2 | 0.5 |
Strongly agree | 0 | 0 |
Disagree | 200 | 50 |
Strongly disagree | 198 | 49.5 |
Immunization is not completely safe for my baby | ||
Agree | 3 | 0.8 |
Strongly agree | 0 | 0 |
Disagree | 397 | 99.3 |
Strongly disagree | ||
Health workers reaction towards pregnant mother is good | ||
Agree | 47 | 11.8 |
Strongly agree | 19 | 4.8 |
Disagree | 302 | 75.5 |
Strongly disagree | 32 | 8 |
Vaccine is effective in preventing diseases | ||
Agree | 385 | 96.3 |
Strongly agree | 5 | 1.3 |
Disagree | 10 | 2.5 |
Strongly disagree | 0 | 0 |
VARIABLE | FREQUENCY (n=400) | PERCENTAGE (%) |
|---|---|---|
Have you ever taken your child for immunization in a health facility | ||
Yes | 391 | 97.8 |
No | 9 | 2.3 |
How many sessions of immunization has your child had | ||
1-3 sessions | 140 | 35 |
4-5 sessions | 232 | 58 |
>5 sessions | 28 | 7 |
VARIABLE | FREQUENCY (n=400) | PERCENTAGE (%) |
|---|---|---|
BCG | ||
COMPLETE | 378 | 94.5 |
INCOMPLETE | 22 | 5.5 |
HBV | ||
COMPLETE | 209 | 52.3 |
INCOMPLETE | 191 | 47.5 |
OPV 0 | ||
COMPLETE | 390 | 97.5 |
INCOMPLETE | 10 | 2.5 |
OPV 1 | ||
COMPLETE | 390 | 97.5 |
INCOMPLETE | 10 | 2.5 |
OPV 2 | ||
COMPLETE | 390 | 97.5 |
INCOMPLETE | 10 | 2.5 |
OPV 3 | ||
COMPLETE | 390 | 97.5 |
INCOMPLETE | 10 | 2.5 |
PCV 1 | ||
COMPLETE | 102 | 25.5 |
INCOMPLETE | 298 | 74.5 |
PCV 2 | ||
COMPLETE | 96 | 24 |
INCOMPLETE | 304 | 76 |
PCV 3 | ||
COMPLETE | 13 | 3.3 |
INCOMPLETE | 387 | 96.8 |
PENTA 1 | ||
COMPLETE | 254 | 63.5 |
INCOMPLETE | 146 | 36.5 |
PENTA 2 | ||
COMPLETE | 218 | 54.5 |
INCOMPLETE | 182 | 45.5 |
PENTA 3 | ||
COMPLETE | 169 | 42.3 |
INCOMPLETE | 231 | 57.8 |
IPV | ||
COMPLETE | 175 | 43.8 |
INCOMPLETE | 225 | 56.3 |
MEASLES | ||
COMPLETE | 384 | 96 |
INCOMPLETE | 16 | 4 |
YELLOW FEVER | ||
COMPLETE | 384 | 96 |
INCOMPLETE | 16 | 4 |
VARIABLE | FREQUENCY (n=400) | PERCENTAGE (%) |
|---|---|---|
Did you always complete the prescribed series of immunizations for your child or children that you immunized before? | ||
Yes | 350 | 87.5 |
No | 50 | 12.5 |
If No, what are your reasons? | ||
Husband do not agree | 5 | 10 |
I do not have time for vaccination | 7 | 14 |
Health facility is far to my house | 1 | 2 |
Adverse effect | 37 | 74 |
HIb | Hemophilus Influenza type b |
WHO | Wordl Health Organization |
LGA | Local Government Area |
NPI | National Programme on Immunization |
RI | Routine Immunization |
SIAs | Supplementary Immunization Activities |
SPSS | Statistical Package for Social Sciences |
| [1] |
World Health Organization. (2023). Immunization coverage. Retrieved May 29, 2024, from
https://www.who.int/news-room/fact-sheets/detail/immunization-coverage |
| [2] | UNICEF. (1990). World Declaration on the Survival, Protection and Development of Children. Asia Pacific Journal of Public Health, 4(2-3), 99–101. |
| [3] | United Nations (UN). (n. d.). Convention on the Rights of the Child. Retrieved May 29, 2024, from |
| [4] | Global Immunization Vision and Strategy (GIVS). (2013). Retrieved May 29, 2024, from |
| [5] | World Health Organization (WHO). (n.d.). Public health preparedness and response. Retrieved May 29, 2024, from |
| [6] | Expanded Programme on Immunization (EPI). (n.d.). Nigeria. Retrieved May 29, 2024, from |
| [7] | National Programme on Immunization (NPI). (n.d.). Nigeria. Routine immunization schedule. Retrieved May 29, 2024, from |
| [8] | UNICEF and WHO. (n.d.). Immunization statistics. Retrieved May 29, 2024, from |
| [9] | World Health Organization (WHO). (n.d.). Demographic Health Survey Nigeria 1999 & 2003. Retrieved May 29, 2024, from |
| [10] | WHO Regional Office for Africa. (n.d.). Immunization in Africa. Retrieved May 29, 2024, from |
| [11] | Tagbo, B. N., Eke, C. B., Omotowo, B. I., Onwuasigwe, C. N., Onyeka, E. B., & Mildred, U. O. (2014). Vaccination coverage and its determinants in children aged 11-23 months in an urban district of Nigeria. World Journal of Vaccines, 4(4), 175-183. |
| [12] |
Worldometer. (2021). Nigeria Population (Live). Retrieved from
https://www.worldometers.info/world-population/nigeria-population/ |
| [13] | Chidiebere, O. D. I., Uchenna, E., & Kenechi, O. S. (2014). Maternal sociodemographic factors that influence full child immunization uptake in Nigeria. South African Journal of Child Health, 8(4), 138-142. |
| [14] | Adeyinka, D. A., Oladimeji, O., Adeyinka, F. E., & Aimakhu, C. (2009). Uptake of childhood immunization among mothers of under-five in Southwestern Nigeria. Journal of Public Health and Epidemiology, 1(2), 35-40. |
| [15] | Babalola, S. (2011). Maternal reasons for non-immunization and under-immunization of children in northern Nigeria. Journal of paediatrics and child health, 47(5), 276-81. |
| [16] | Hussain, S. F., Boyle, P., Patel, P., & Sullivan, R. (2010). Eradicating polio in Pakistan: A study of the challenges and solutions. Globalization and health, 12(1), 63. |
| [17] | Yang, J., et al. (2020). Factors associated with recommendation behaviors of four non-National Immunization Program vaccines: a cross-sectional survey among public health workers in China. Infectious Diseases of Poverty. |
| [18] | Patra, S., & Singh, P. (2021). Exploring the dynamics of vaccine hesitancy in rural India. Vaccine, 39(19), 2658-2665. |
| [19] | Belachew, T., et al. (2021). Factors influencing the uptake of childhood immunization in Ethiopia: A community-based cross-sectional study. BMC Public Health, 21(1), 421. |
| [20] | Hussain, S., et al. (2020). Barriers to childhood immunization in rural Pakistan: A qualitative study. Vaccine, 38(30), 4737-4745. |
| [21] | Ophori, E. A., Tula, M. Y., Azih, A. V., Okojie, R., & Ikpo, P. E. (2014). Current trends of immunization in Nigeria: prospect and challenges. Tropical Medicine and Health, 42(2), 67-75. |
| [22] | Akwataghibe, N. N., Ogunsola, E. A., Broerse, J., Popoola, O. A., Agbo, A. I., & Dieleman, M. A. (2019). Exploring factors influencing immunization utilization in Nigeria-A mixed methods study. Frontiers in Public Health, 7, 392. |
APA Style
Daniel, E. O., Olawale, O. O., Avwerhota, M., Bello, A. M., Tomori, M. O., et al. (2024). An Appraisal of Routine Immunization Coverage Among Children 0-2 Years in Akure South Local Government Area of Ondo State. International Journal of Immunology, 12(2), 19-29. https://doi.org/10.11648/j.iji.20241202.11
ACS Style
Daniel, E. O.; Olawale, O. O.; Avwerhota, M.; Bello, A. M.; Tomori, M. O., et al. An Appraisal of Routine Immunization Coverage Among Children 0-2 Years in Akure South Local Government Area of Ondo State. Int. J. Immunol. 2024, 12(2), 19-29. doi: 10.11648/j.iji.20241202.11
@article{10.11648/j.iji.20241202.11,
author = {Ebenezer Obi Daniel and Oluseyi Oludamilola Olawale and Michael Avwerhota and Ahmed Mamuda Bello and Michael Olabode Tomori and Israel Olukayode Popoola and Adebanke Adetutu Ogun and Aisha Oluwakemi Salami and Olukayode Oladeji Alewi and Taiwo Aderemi Popoola and Celestine Emeka Ekwuluo},
title = {An Appraisal of Routine Immunization Coverage Among Children 0-2 Years in Akure South Local Government Area of Ondo State
},
journal = {International Journal of Immunology},
volume = {12},
number = {2},
pages = {19-29},
doi = {10.11648/j.iji.20241202.11},
url = {https://doi.org/10.11648/j.iji.20241202.11},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.iji.20241202.11},
abstract = {Immunization is a proven tool for controlling and eliminating life-threatening infectious diseases such as Tuberculosis, Poliomyelitis, Haemophilus Influenza type b (HIB), Diphtheria, Pertusis, Tetanus and Hepatitis B, neonatal tetanus yellow fever, measles, cerebrospinal meningitis and is estimated to avert between 2 and 3 million deaths each year. The objective of this study is to appraise routine immunization coverage among children 0-2 years in Akure South Local Government Area of Ondo State. This is a descriptive cross-sectional study, designed to appraise routine immunization coverage among children 0-2 years in Akure South Local Government Area of Ondo State. The study focused on children 0-2 years. Majority 102 (25.2%) of the respondents were within the age range of 25-29 years, 82 (20.5%) were >39 years. 314 (78.5%) were Yorubas. 385 (96.2%) had good knowledge while 15 (3.8%) had poor knowledge. 374 (93.5%) of the women have positive attitude while 26 (6.5%) of them have negative attitude. Most of the respondents, 391 (97.8%) of the respondents reported that they have taken their child to the health facility for immunization and 232 (58%) have taken their child to 4-5 immunization sessions. Based on the findings of the present study, it could be concluded that very few of the women had poor knowledge of childhood immunization, majority of the women had positive attitude score and practice of childhood immunization, practice of childhood immunization is quite high, and the uptake of childhood immunization is quite high.
},
year = {2024}
}
TY - JOUR T1 - An Appraisal of Routine Immunization Coverage Among Children 0-2 Years in Akure South Local Government Area of Ondo State AU - Ebenezer Obi Daniel AU - Oluseyi Oludamilola Olawale AU - Michael Avwerhota AU - Ahmed Mamuda Bello AU - Michael Olabode Tomori AU - Israel Olukayode Popoola AU - Adebanke Adetutu Ogun AU - Aisha Oluwakemi Salami AU - Olukayode Oladeji Alewi AU - Taiwo Aderemi Popoola AU - Celestine Emeka Ekwuluo Y1 - 2024/06/25 PY - 2024 N1 - https://doi.org/10.11648/j.iji.20241202.11 DO - 10.11648/j.iji.20241202.11 T2 - International Journal of Immunology JF - International Journal of Immunology JO - International Journal of Immunology SP - 19 EP - 29 PB - Science Publishing Group SN - 2329-1753 UR - https://doi.org/10.11648/j.iji.20241202.11 AB - Immunization is a proven tool for controlling and eliminating life-threatening infectious diseases such as Tuberculosis, Poliomyelitis, Haemophilus Influenza type b (HIB), Diphtheria, Pertusis, Tetanus and Hepatitis B, neonatal tetanus yellow fever, measles, cerebrospinal meningitis and is estimated to avert between 2 and 3 million deaths each year. The objective of this study is to appraise routine immunization coverage among children 0-2 years in Akure South Local Government Area of Ondo State. This is a descriptive cross-sectional study, designed to appraise routine immunization coverage among children 0-2 years in Akure South Local Government Area of Ondo State. The study focused on children 0-2 years. Majority 102 (25.2%) of the respondents were within the age range of 25-29 years, 82 (20.5%) were >39 years. 314 (78.5%) were Yorubas. 385 (96.2%) had good knowledge while 15 (3.8%) had poor knowledge. 374 (93.5%) of the women have positive attitude while 26 (6.5%) of them have negative attitude. Most of the respondents, 391 (97.8%) of the respondents reported that they have taken their child to the health facility for immunization and 232 (58%) have taken their child to 4-5 immunization sessions. Based on the findings of the present study, it could be concluded that very few of the women had poor knowledge of childhood immunization, majority of the women had positive attitude score and practice of childhood immunization, practice of childhood immunization is quite high, and the uptake of childhood immunization is quite high. VL - 12 IS - 2 ER -
Department of Public Health, Swansea University, Swansea, United Kingdom; Department of Public Health, Texila American University, Georgetown, Guyana
Department of Public Health, Walden University, Minneapolis, United States of America
Department of Public Health, Atlantic International University, Hawaii, United States of America
Department of Public Health, Texila American University, Georgetown, Guyana
Department of Public Health, Texila American University, Georgetown, Guyana
Department of Epidemiology and Community Health, University of Ilorin, Ilorin, Nigeria
Department of Policy, Governance, Liaison, and Support, International Organization for Migration, Abuja, Nigeria
Department of Public Health, Texila American University, Georgetown, Guyana
Department of Public Health, Texila American University, Georgetown, Guyana
Department of Research, PhMetrika Limited, Birmingham, United Kingdom
Department of Child Health, United Nations International Children's Emergency Fund, Abuja, Nigeria
Information