Background: The aims of this study were to assess the frequency of lower extremity arterial occlusive disease in HIV-positive patients on antiretroviral therapy by measuring the ankle-brachial index (ABI) and to examine the links between the HIV condition, antiretroviral therapy administration, and associated cardiovascular risk factors. Methods: This was a descriptive and analytical cross-sectional study with prospective data collection, conducted from May 1st to June 30th, 2022. Included were HIV-positive patients on antiretroviral therapy after signing an informed consent. The collected data included particularly the systematic and bilateral measurement of the ankle-brachial index. Any difference less than 0.05 was considered statistically significant. Results: Our study was conducted on 150 patients. There was a female predominance with a sex ratio of 0.58. The average age was 46.78±12.37 years. The main cardiovascular risk factors identified were dyslipidemia (51.6%), hypertension (19.5%), smoking (6.9%), and diabetes (3.4%). The duration of HIV infection over 15 years was most represented at 37.6%. The frequency of PAD was 55.2%. Among these, 37.6% had poorly compensated PAD. There was a correlation between PAD and smoking (p=0.029), dyslipidemia (p=0.02), and the duration of HIV infection between 6 and 10 years (p=0.039). Conclusion: Our study shows a very high frequency of PAD in patients living with HIV and highlights the importance of the ABI in screening for PAD in this patient group.
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited.
Peripheral Artery Disease, HIV, Sub-Saharan Africa
1. Introduction
Atherosclerosis is by far the main arterial disease affecting humans today. Targeting large and medium-sized arteries, it is defined as an obstructive disease of the lower limb vessels
[1]
Masiá M, Padilla S, García JA et al. Evolving understanding of cardiovascular, cerebrovascular and peripheral arterial disease in people living with HIV and role of novel biomarkers. A study of the Spanish CoRIS cohort, 2004-2015. PLoS One. 2019; 14(4): 215-27.
. It involves an atheromatous obstruction of the arteries between the abdominal aorta and the digital arteries supplying the lower limbs. Due to its complications and systemic expression, atherosclerosis is responsible for acute or chronic ischemic phenomena, with the main targets being the myocardium, the brain, and the lower limbs
[1]
Masiá M, Padilla S, García JA et al. Evolving understanding of cardiovascular, cerebrovascular and peripheral arterial disease in people living with HIV and role of novel biomarkers. A study of the Spanish CoRIS cohort, 2004-2015. PLoS One. 2019; 14(4): 215-27.
. Indeed, one-third of atheromatous patients are asymptomatic polyvascular individuals who are at very high cardiovascular risk
[1]
Masiá M, Padilla S, García JA et al. Evolving understanding of cardiovascular, cerebrovascular and peripheral arterial disease in people living with HIV and role of novel biomarkers. A study of the Spanish CoRIS cohort, 2004-2015. PLoS One. 2019; 14(4): 215-27.
Peripheral Arterial Disease (PAD) is the third most common location for atherosclerosis, after coronary and cerebral involvement,
[2]
Knudsen AD, Gelpi M, Afzal S et al. Brief Report: Prevalence of Peripheral Artery Disease Is Higher in Persons Living With HIV Compared With Uninfected Controls. J Acquir Immune Defic Syndr. 2018; 79(3): 381-5.
. It is estimated that more than 200 million individuals are affected by PAD worldwide. This prevalence has increased by about 25% between 2000 and 2010, particularly in low/middle-income countries. Nearly two-thirds of the PAD-affected population presents its asymptomatic form
[1]
Masiá M, Padilla S, García JA et al. Evolving understanding of cardiovascular, cerebrovascular and peripheral arterial disease in people living with HIV and role of novel biomarkers. A study of the Spanish CoRIS cohort, 2004-2015. PLoS One. 2019; 14(4): 215-27.
. Hence, the majority of epidemiological studies utilize the measurement of the Ankle-Brachial Index (ABI)
[3]
Aboyans V, Criqui MH, Abraham P et al. Measurement and interpretation of the Ankle-Brachial Index: a scientific statement from the American Heart Association. Circulation. 2012; 126: 2890-909.
The ABI measurement is indicated as a first-intention non-invasive test for screening and diagnosing PAD (I, C)
[3]
Aboyans V, Criqui MH, Abraham P et al. Measurement and interpretation of the Ankle-Brachial Index: a scientific statement from the American Heart Association. Circulation. 2012; 126: 2890-909.
. It is a simple, non-invasive, and cost-effective clinical measure. An arterial component is suspected in case of an ABI lower than 0.9, and confirmed if the ABI is below 0.5
[3]
Aboyans V, Criqui MH, Abraham P et al. Measurement and interpretation of the Ankle-Brachial Index: a scientific statement from the American Heart Association. Circulation. 2012; 126: 2890-909.
. Thus, lower limb arterial occlusive disease serves as a severity marker of atherothrombotic disease, whether symptomatic or not.
In patients living with HIV (PLWH) on Antiretroviral (ARV), lower limb involvement is often overlooked, yet it also represents a marker of poorer prognosis. The world regions that have seen the most significant increase in PAD are Southeast Asia and the Western Pacific, with global data on PAD prevalence trends between 2000 and 2010 being recently published. During this period, the number of individuals with PAD rose by 28.7% in low and middle-income countries and by 13.1% in high-income countries
[4]
Fowkes FGR, Rudan D, Rudan I et al. Comparison of global estimates of prevalence and risk factors for peripheral artery disease in 2000 and 2010: a systematic review and analysis. Lancet. 2013; 382: 1329-40.
. However, this improvement in survival has led to the emergence of non-infectious comorbidities.
HIV-positive patients have twice the risk of cardiovascular events (CVD) compared to non-HIV-infected individual
[6]
Fiorentini A. "QTc interval prolongation in HIV-infected patients: a case–control study by 24-hour Holter ECG recording." BMC Cardiovascular Disorders. 2012; 12: 1-6.
. Cardiovascular disease (CVD) remains one of the leading causes of death among PLWH, along with cancer and infection
[7]
Larifla L. Athérosclérose, hypertension, thrombose. Elsevier Masson; 2002: 1; 25-58.
[7]
. It, therefore, seems pertinent to screen for this involvement, particularly by measuring the Ankle-Brachial Index, to detect a patient subgroup at higher risk levels, thus optimizing therapeutic management
[5]
Schwartz PJ, Woosley RL. Predicting the Unpredictable: Drug-Induced QT Prolongation and Torsades de Pointes. J Am Coll Cardiol. 2016; 67(13): 1639-50.
Marcus JL, Chao CR, Leyden Wa et al. Narrowing the gap in life expectancy between HIV-infected and HIV-uninfected individuals with access to care. J Acquir Immune Defic Syndr. 2016; 58: 242-52.
The main objective of the study was to screen for lower limb arterial occlusive disease by measuring the ABI in patients living with HIV on ART. The specific objectives were to describe the epidemiological and diagnostic aspects of lower limb arterial disease, to analyze ABI data, and to correlate lower limb arterial disease with HIV status, ART administration, and associated cardiovascular risk factors in patients living with HIV on ART.
2. Methodology
2.1. Study Design and Inclusion Criteria
This was a cross-sectional, descriptive, analytical study with prospective data collection. The study was conducted over a 2-month period from May 1 to June 30, 2022. Included in our study were HIV-positive patients on ART aged at least 18 years, of all genders, followed at the regional research and training center of the FANN University Hospital in Dakar. We studied sociodemographic aspects, cardiovascular risk factors, clinical, and paraclinical data. These various parameters were collected based on a questionnaire and compiled into an exploitation sheet.
2.2. Ankle-Brachial Index Measurement Method
The Ankle-Brachial Index (ABI) was obtained by calculating the ratio of the systolic blood pressure at the ankle (anterior and posterior tibial arteries) to the brachial systolic blood pressure. For this, a Spengler manual sphygmomanometer and an EDAN SD3 VASCULAR pocket Doppler (Hamburg, Germany) were used. The performance of the ABI, ECG (Electrocardiogram), and cardiac ultrasound was free for all patients. After joining, the PAD and the ABI were explained to them, as well as the measurement technique. The duration of the measurement varied between 5 and 10 minutes. Patients with pathological ABI values either received medical treatment or were referred to cardiovascular surgery for optimal care.
2.3. Ethical Considerations
This work was carried out in collaboration with the Director of the Regional Research and Training Center (RRTC) after obtaining the center's approval by signing the RRTC confidentiality sheet. An information note was prepared for the patients, summarizing the survey made available to each patient. The two-page information letter mentioned the title, objectives, target, duration, number of patients to include, advantages and disadvantages of the survey, and contact details of the survey leaders. Written consent was obtained from the patients; those who refused to participate were excluded, and this did not impact their care and follow-up in the service. All patients were informed about the confidentiality of the study.
2.4. Statistical Analysis
Data analysis was performed using Epi Info software version 7 and R studio version 4. In the descriptive analysis, qualitative variables were described by frequency, percentages, and quantitative variables by mean with standard deviation, extremes, and median. The bivariate analysis consisted of correlating PAD with other variables. The Chi-square tests (Fisher and Pearson) and Yates's corrected Chi-square were used for proportion comparisons. The relationship was considered statistically significant when the p-value was strictly less than 0.05.
3. Results
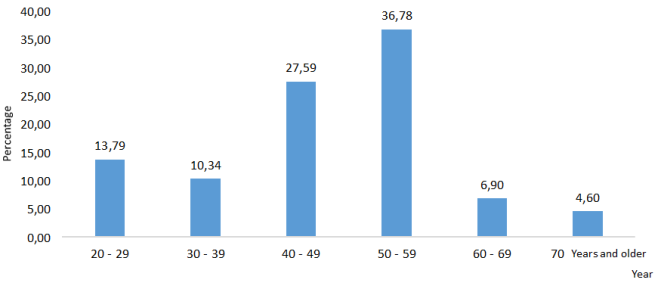
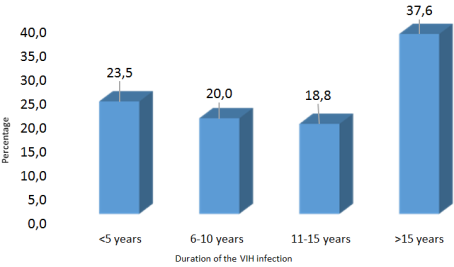
Our study was conducted on 150 patients. There was a female predominance with a sex ratio of 0.58. The mean age was 46.78 years +/- 12.37, with the median age at 47.5 years, ranging from 18 to 83 years. The 50 to 59 age group was the most represented (Figure 1). The majority of patients came from the suburbs of Dakar, accounting for 49.4%. Patients working in the private sector were more represented (54%). The main cardiovascular risk factors identified were dyslipidemia (51.6%), sedentary lifestyle (24.6%), hypertension (19.5%), obesity (15%), smoking (6.9%), and diabetes (3.4%). The duration of HIV infection exceeding 15 years was the most represented at 37.6% (Figure 2).
Figure 2. Distribution of the sample based on the duration of HIV infection (n=150).
Clinically, 4.6% of patients had intermittent claudication. Among them, 25% complained of numbness, and 75% had cramps. Erectile dysfunction was observed in 16% of the study patients. It was moderate in half of the cases and severe in 21.4%, with a significant relationship (p value=0.03). The examination of peripheral pulses did not reveal unilateral abolition of pedal and retro-malleolar pulses. The main disturbances in the lipid profile were elevated total cholesterol (51.56%), LDL cholesterol (20.7%), and triglycerides (26.1%). The anomalies detected on the electrocardiogram were dominated by conduction disorders such as left anterior hemiblock (62.5%) and complete right bundle branch block (37.5%). Almost all patients had a normal left ventricular ejection fraction (LVEF) at 98.2%.
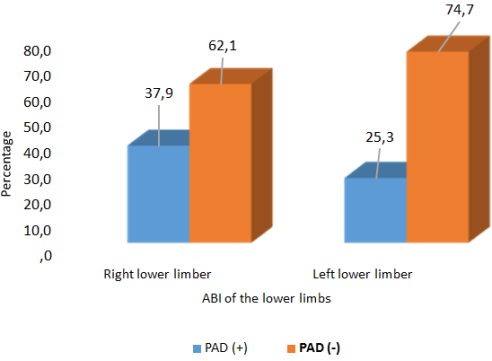
Figure 3. Distribution of the population based on the ABI of the lower limbs (n=150).
The ABI in patients living with HIV on ARV revealed a PAD frequency (ABI < 0.9) of 55.2%. Among these, 72.4% had well-compensated PAD and 37.6% had poorly compensated PAD. The right lower limb was most often affected, involving the anterior tibial artery in 37.9% of cases (40.5%). The left lower limb was affected in 25.3% of cases, predominantly involving the anterior tibial artery (35.5%) (Figure 3). PAD was more common in females, with a proportion of 68.8% and a sex ratio of 0.45. It was also more frequent among those under 50 years, with 50.8% of cases (p=0.46) (Table 1). All patients were on triple therapy with Tenofovir, Lamivudine, and Dolutegravir.
Table 1. Comparison between PAD and different age groups.
Years
PAD
Total
P
PAD (+)
PAD (-)
20 - 29
14.3%
12.5%
13.8%
0.57
30 - 39
9.5%
12.5%
10.3%
0.47
40 - 49
27%
29.2%
27.6%
0.84
50 - 59
36.5%
37.5%
36.8%
0.93
60 - 69
7.9%
4.2%
6.9%
0.47
70+
4.8%
4.2%
4.6%
0.7
Factors correlated with the occurrence of PAD were smoking (p= 0.03), dyslipidemia (p= 0.02) (Table 2), and the duration of HIV infection between six and ten years (p=0.04) (Table 3). There was no correlation between PAD and the duration of ARV (Table 4) or with other cardiovascular risk factors, electrocardiographic, and echocardiographic anomalies.
Table 2. Distribution of PAD according to cardiovascular risk factors.
Cardiovascular risk factors
PAD
Total
P
PAD (+)
PAD (-)
Tobacco
Yes
11.1%
29.2%
16.1%
0.04
No
88.9%
70.8%
83.9%
Dyslipidemia
Yes
68.6%
55%
70.5%
0.02
No
98.4%
100%
29.5%
Sedentary
Yes
27%
25%
26.4%
0.54
Lifestyle
No
73%
75%
73.6%
Diabetes
Yes
3.2%
4.2%
3.4%
0.62
No
96.8%
95.8%
96.6%
HTA
Yes
19%
20.8%
19.5%
0.53
No
81%
79.2%
80.5%
Obésity (BMI)
Yes
19%
4.2%
14.9%
0.07
No
81%
95.8%
85.1%
Table 3. Comparison between PAD and the duration of the Infection.
Durée d’infection
PAD
Total
P
Yes
No
≤ 5 yaers
45.0%
55.0%
100.0%
0.35
6 - 10 years
76.5%
23.5%
100.0%
0.04
11-15 years
56.3%
43.8%
100.0%
0.85
> 15 years
46.9%
53.1%
100.0%
0.3
Table 4. Comparison between PAD and the Duration of ART Treatment.
Duration of ART treaitment
PAD
Total
P
Yes
No
≤ 5 years
47.8%
52.2%
100.0%
0.41
6 - 10 years
70.0%
30.0%
100.0%
0.12
11 - 15 years
57.1%
42.9%
100.0%
0.86
> 15 years
47.8%
52.2%
100.0%
0.41
4. Discussion
This study faced limitations due to its non-comparative nature, notably the absence of a control group not exposed to antiretroviral (ARV) treatment, a situation complicated by the universal treatment policy in Senegal. Despite these limitations, our study sheds significant light on the prevalence of peripheral artery disease (PAD) among people living with HIV (PLWH) on ARV therapy. We observed a high prevalence of PAD, with 55.2% of participants presenting with an ankle-brachial pressure index (ABPI) below 0.9, indicative of obstructive artery disease. This prevalence significantly exceeds those reported in earlier studies, where rates varied from 2 to 10%
[6]
Fiorentini A. "QTc interval prolongation in HIV-infected patients: a case–control study by 24-hour Holter ECG recording." BMC Cardiovascular Disorders. 2012; 12: 1-6.
Capeau J, Caron M, Vigouroux C et al. Les lipodystrophies secondaires aux traitements antirétroviraux de l’infection par le VIH [Lipodystrophy Secondary to antiretroviral therapy for HIV infection]. Médecine/sciences. 2006; 22(5): 531-36. URI:
highlighted a prevalence rate of 20.7% of peripheral arterial disease in HIV patients on ARV therapy, thus underscoring the magnitude of the issue.
Our analysis also reveals that certain cardiovascular risk factors, such as dyslipidaemia (p=0.02) and smoking (p=0.04), were significantly associated with PAD in our study population. ARV treatments are known to impact the metabolism of triglyceride-rich lipoproteins
[4]
Fowkes FGR, Rudan D, Rudan I et al. Comparison of global estimates of prevalence and risk factors for peripheral artery disease in 2000 and 2010: a systematic review and analysis. Lancet. 2013; 382: 1329-40.
, which could explain the observed association. A study in Dakar also reported elevated levels of total cholesterol and LDL-cholesterol in PLWH, suggesting an increased risk of cardiovascular diseases
[11]
Mingou J, Aw F, Sarr SA et al. Dyslipidemia of Patients living with HIV in DAKAR Transversal study, Case-witnesses, Multicentric. Revue Africaine et Malgache pour la Recherche Scientifique / Sciences de la Santé / Vol. 1, N° 3, Décembre 2020.
Cheng S, Claggett B, Correia AW, et al. Temporal trends in the population attributable risk for cardiovascular disease: the Atherosclerosis Risk in Communities Study. Circulation. 2014; 130(10): 820-8.
. Regarding smoking, its strong epidemiological correlation with PAD has been established, with the risk being tripled for smokers, proportionally to the extent of exposure
[13]
Willey JZ, Moon YP, Kahn E, et al. Population attributable risks of hypertension and diabetes for cardiovascular disease and stroke in the northern Manhattan study. J Am Heart Assoc. 2014; 3(5): e001106.
Aboyans V, Ricco JB, Bartelink MEL, et al. 2017 ESC Guidelines on the Diagnosis and Treatment of Peripheral Arterial Diseases, in collaboration with the European Society for Vascular Surgery (ESVS). Eur J Vasc Endovasc Surg. 2017; Aug 26.
Although the association between PAD and other risk factors such as hypertension, obesity, diabetes, as well as demographic variables, was not significantly established, these elements contribute to a broader context of cardiovascular risk. Interestingly, our study indicates that HIV infection itself, independent of other cardiovascular risk factors, is a risk factor for the reduction of the ABPI, suggesting that HIV might promote atherosclerosis. This conclusion underscores the importance of not limiting atherosclerotic therapeutic strategies to the metabolic complications of ARVs alone but also considering HIV infection
[15]
Bernal E, Masiá M, Padilla S et al. Low prevalence of peripheral arterial disease in HIV-infected patients with multiple cardiovascular risk factors. J Acquir Immune Defic Syndr. 2008; 47(1): 126-7.
Global T, Extremity L, Study A. Epidemiology of lower extremity amputation in centres in Europe, North America and East Asia. The Global Lower Extremity Amputation Study group. Br J Surg. 2000; 87: 328-37.
From a clinical perspective, we found that 16% of patients presented with erectile dysfunction (p=0.03), a condition with varied pathophysiological mechanisms often associated with age and endothelial inflammation due to prolonged viral replication, thereby promoting atherosclerosis
[17]
Feinstein MJ, Bahiru E, Achenbach C et al. Patterns of cardiovascular, mortality for HIV-infected adults in the United States: 1999 to 2013. Am J Cardiol. 2016; 117: 214-20.
Finally, our study explored the correlation between PAD and other indicators of cardiovascular or systemic health, reaffirming the utility of the ECG as a screening tool in resource-limited settings, especially among seropositive patients. Although we did not observe any cases of prolonged QTc, a precursor sign of potentially fatal cardiac arrhythmias, monitoring these abnormalities remains crucial
[18]
Wang Q, Young J, Bernasconi E et al. The prevalence of erectile dysfunction and its association with antiretroviral therapy in HIV-infected men: the Swiss HIV Cohort Study. Antiviral therapy, 2013; 18(3): 337-44.
Soliman EZ, Prineas RJ, Roediger MP et al. Prevalence and prognostic significance of ECG abnormalities in HIV–infected patients: results from the Strategies for Management of Antiretroviral Therapy study. Journal of electrocardiology. 2011; 44(6): 779-85.
This study highlights the necessity of tailored screening and management of PAD among PLWH on ARV therapy.
5. Conclusion
This study underscores the significance of the socioeconomic context, comorbidities, and the comprehensive management of HIV patients. It stresses the importance of tailored prevention strategies and cardiovascular risk management for this specific population. The research has highlighted the utility of the Ankle-Brachial Pressure Index (ABPI) in screening for Peripheral Arterial Disease (PAD) in individuals living with HIV and has delineated the complexity of the various variables associated with the elevated risk of cardiovascular events in people living with HIV (PLWH). These include cardiovascular risk factors, inflammation, and the use of antiretrovirals (ARVs).
PAD in a confirmed seropositive patient could be considered merely anecdotal, lacking specific prognostic value and thus not having a particular impact. However, it is observed that regardless of the stage of HIV/AIDS, the presence of PAD constitutes a factor of poor prognosis or at least an exacerbating factor. Nonetheless, the practice of ABPI measurement remains limited due to a lack of awareness or knowledge among physicians.
6. Recommendations
To enhance the management of Peripheral Arterial Disease (PAD) among People Living with HIV (PLWH) in Africa, the following actions are recommended:
1) Strengthen early screening by integrating Ankle-Brachial Index (ABI) measurement into routine care and organizing community-based campaigns supported by community health workers.
2) Optimize cardiovascular management by actively addressing risk factors (smoking, dyslipidemia, hypertension) and tailoring antiretroviral therapy (ART) to minimize cardiovascular side effects.
3) Develop infrastructure and specialized care networks, including establishing integrated cardiovascular reference centers within HIV care facilities.
4) Train healthcare professionals on PAD and cardiovascular risks in PLWH while promoting local research to generate context-specific evidence.
5) Advocate to policymakers for the inclusion of PAD in national HIV programs and allocate resources for prevention campaigns.
6) Improve epidemiological surveillance by creating local registries to monitor PAD prevalence and inform public health strategies.
These measures aim to reduce cardiovascular complications, enhance the quality of life for PLWH, and strengthen the capacity of African healthcare systems.
Abbreviation
ABPI
Ankle-Brachial Pressure Index
ARV
Antiretroviral
CVD
Cardiovascular Disease
RRTC
Regional Research and Training Center
ECG
Electrocardiogram
LVEF
Left Ventricular Ejection Fraction
HAART
Highly Active Antiretroviral Therapy
HIV
Human Immunodeficiency Virus
AIDS
Acquired Immunodeficiency Syndrome
PAD
Peripheral Arterial Disease
PLWH
People Living with HIV
Authors Contributions
A.A.N, N.D.G, A.A, S.M.B, A.M, and A.K designed the study protocol, participated in the data collection and contributed in analysing the data and writing of the draft manuscript.
M.D, F.W, S.A.S, M.L and M.B oversaw the execution of the study, participated in data analysis and critically revised the manuscript for important intellectual content.
K.D, A.R.D, E.H.B.D, M.B.N and A.K participated in study design and in data analysis.
J.S.M, H.H, M.T.D and M.D participated in statistical analysis and interpretation of results.
All authors have read and approved the final version of the manuscript.
Funding
The study did not receive any funding.
Conflicts of Interest
The authors declare no conflicts of interest.
References
[1]
Masiá M, Padilla S, García JA et al. Evolving understanding of cardiovascular, cerebrovascular and peripheral arterial disease in people living with HIV and role of novel biomarkers. A study of the Spanish CoRIS cohort, 2004-2015. PLoS One. 2019; 14(4): 215-27.
Knudsen AD, Gelpi M, Afzal S et al. Brief Report: Prevalence of Peripheral Artery Disease Is Higher in Persons Living With HIV Compared With Uninfected Controls. J Acquir Immune Defic Syndr. 2018; 79(3): 381-5.
Aboyans V, Criqui MH, Abraham P et al. Measurement and interpretation of the Ankle-Brachial Index: a scientific statement from the American Heart Association. Circulation. 2012; 126: 2890-909.
Fowkes FGR, Rudan D, Rudan I et al. Comparison of global estimates of prevalence and risk factors for peripheral artery disease in 2000 and 2010: a systematic review and analysis. Lancet. 2013; 382: 1329-40.
Fiorentini A. "QTc interval prolongation in HIV-infected patients: a case–control study by 24-hour Holter ECG recording." BMC Cardiovascular Disorders. 2012; 12: 1-6.
Larifla L. Athérosclérose, hypertension, thrombose. Elsevier Masson; 2002: 1; 25-58.
[8]
Marcus JL, Chao CR, Leyden Wa et al. Narrowing the gap in life expectancy between HIV-infected and HIV-uninfected individuals with access to care. J Acquir Immune Defic Syndr. 2016; 58: 242-52.
Capeau J, Caron M, Vigouroux C et al. Les lipodystrophies secondaires aux traitements antirétroviraux de l’infection par le VIH [Lipodystrophy Secondary to antiretroviral therapy for HIV infection]. Médecine/sciences. 2006; 22(5): 531-36. URI:
Mingou J, Aw F, Sarr SA et al. Dyslipidemia of Patients living with HIV in DAKAR Transversal study, Case-witnesses, Multicentric. Revue Africaine et Malgache pour la Recherche Scientifique / Sciences de la Santé / Vol. 1, N° 3, Décembre 2020.
Cheng S, Claggett B, Correia AW, et al. Temporal trends in the population attributable risk for cardiovascular disease: the Atherosclerosis Risk in Communities Study. Circulation. 2014; 130(10): 820-8.
Willey JZ, Moon YP, Kahn E, et al. Population attributable risks of hypertension and diabetes for cardiovascular disease and stroke in the northern Manhattan study. J Am Heart Assoc. 2014; 3(5): e001106.
Aboyans V, Ricco JB, Bartelink MEL, et al. 2017 ESC Guidelines on the Diagnosis and Treatment of Peripheral Arterial Diseases, in collaboration with the European Society for Vascular Surgery (ESVS). Eur J Vasc Endovasc Surg. 2017; Aug 26.
Bernal E, Masiá M, Padilla S et al. Low prevalence of peripheral arterial disease in HIV-infected patients with multiple cardiovascular risk factors. J Acquir Immune Defic Syndr. 2008; 47(1): 126-7.
Global T, Extremity L, Study A. Epidemiology of lower extremity amputation in centres in Europe, North America and East Asia. The Global Lower Extremity Amputation Study group. Br J Surg. 2000; 87: 328-37.
Feinstein MJ, Bahiru E, Achenbach C et al. Patterns of cardiovascular, mortality for HIV-infected adults in the United States: 1999 to 2013. Am J Cardiol. 2016; 117: 214-20.
Wang Q, Young J, Bernasconi E et al. The prevalence of erectile dysfunction and its association with antiretroviral therapy in HIV-infected men: the Swiss HIV Cohort Study. Antiviral therapy, 2013; 18(3): 337-44.
Soliman EZ, Prineas RJ, Roediger MP et al. Prevalence and prognostic significance of ECG abnormalities in HIV–infected patients: results from the Strategies for Management of Antiretroviral Therapy study. Journal of electrocardiology. 2011; 44(6): 779-85.
Ngaïdé, A. A., Gaye, N. D., Mingou, J. S., Haimed, H., Diop, K., et al. (2025). Screening for Lower Limb Arterial Occlusive Disease in HIV Patients on Antiretroviral Therapy: A Monocentric Study of 150 Patients in Dakar, Senegal. International Journal of HIV/AIDS Prevention, Education and Behavioural Science, 11(1), 30-36. https://doi.org/10.11648/j.ijhpebs.20251101.14
Ngaïdé, A. A.; Gaye, N. D.; Mingou, J. S.; Haimed, H.; Diop, K., et al. Screening for Lower Limb Arterial Occlusive Disease in HIV Patients on Antiretroviral Therapy: A Monocentric Study of 150 Patients in Dakar, Senegal. Int. J. HIV/AIDS Prev. Educ. Behav. Sci.2025, 11(1), 30-36. doi: 10.11648/j.ijhpebs.20251101.14
Ngaïdé AA, Gaye ND, Mingou JS, Haimed H, Diop K, et al. Screening for Lower Limb Arterial Occlusive Disease in HIV Patients on Antiretroviral Therapy: A Monocentric Study of 150 Patients in Dakar, Senegal. Int J HIV/AIDS Prev Educ Behav Sci. 2025;11(1):30-36. doi: 10.11648/j.ijhpebs.20251101.14
@article{10.11648/j.ijhpebs.20251101.14,
author = {Aliou Alassane Ngaïdé and Ngoné Diaba Gaye and Joseph Salvador Mingou and Houda Haimed and Karim Diop and Amadou Rassoul Diouf and El Hadji Bara Diop and Marguerite Tennig Diouf and Momar Dioum and Fatou Aw and Simon Antoine Sarr and Alain Affangla and Serigne Mor Beye and Mouhamed Leye and Malick Bodian and Mouhamadou Bamba Ndiaye and Alassane Mbaye and Adama Kane and Maboury Diao and Abdoul Kane},
title = {Screening for Lower Limb Arterial Occlusive Disease in HIV Patients on Antiretroviral Therapy: A Monocentric Study of 150 Patients in Dakar, Senegal},
journal = {International Journal of HIV/AIDS Prevention, Education and Behavioural Science},
volume = {11},
number = {1},
pages = {30-36},
doi = {10.11648/j.ijhpebs.20251101.14},
url = {https://doi.org/10.11648/j.ijhpebs.20251101.14},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ijhpebs.20251101.14},
abstract = {Background: The aims of this study were to assess the frequency of lower extremity arterial occlusive disease in HIV-positive patients on antiretroviral therapy by measuring the ankle-brachial index (ABI) and to examine the links between the HIV condition, antiretroviral therapy administration, and associated cardiovascular risk factors. Methods: This was a descriptive and analytical cross-sectional study with prospective data collection, conducted from May 1st to June 30th, 2022. Included were HIV-positive patients on antiretroviral therapy after signing an informed consent. The collected data included particularly the systematic and bilateral measurement of the ankle-brachial index. Any difference less than 0.05 was considered statistically significant. Results: Our study was conducted on 150 patients. There was a female predominance with a sex ratio of 0.58. The average age was 46.78±12.37 years. The main cardiovascular risk factors identified were dyslipidemia (51.6%), hypertension (19.5%), smoking (6.9%), and diabetes (3.4%). The duration of HIV infection over 15 years was most represented at 37.6%. The frequency of PAD was 55.2%. Among these, 37.6% had poorly compensated PAD. There was a correlation between PAD and smoking (p=0.029), dyslipidemia (p=0.02), and the duration of HIV infection between 6 and 10 years (p=0.039). Conclusion: Our study shows a very high frequency of PAD in patients living with HIV and highlights the importance of the ABI in screening for PAD in this patient group.},
year = {2025}
}
TY - JOUR
T1 - Screening for Lower Limb Arterial Occlusive Disease in HIV Patients on Antiretroviral Therapy: A Monocentric Study of 150 Patients in Dakar, Senegal
AU - Aliou Alassane Ngaïdé
AU - Ngoné Diaba Gaye
AU - Joseph Salvador Mingou
AU - Houda Haimed
AU - Karim Diop
AU - Amadou Rassoul Diouf
AU - El Hadji Bara Diop
AU - Marguerite Tennig Diouf
AU - Momar Dioum
AU - Fatou Aw
AU - Simon Antoine Sarr
AU - Alain Affangla
AU - Serigne Mor Beye
AU - Mouhamed Leye
AU - Malick Bodian
AU - Mouhamadou Bamba Ndiaye
AU - Alassane Mbaye
AU - Adama Kane
AU - Maboury Diao
AU - Abdoul Kane
Y1 - 2025/03/18
PY - 2025
N1 - https://doi.org/10.11648/j.ijhpebs.20251101.14
DO - 10.11648/j.ijhpebs.20251101.14
T2 - International Journal of HIV/AIDS Prevention, Education and Behavioural Science
JF - International Journal of HIV/AIDS Prevention, Education and Behavioural Science
JO - International Journal of HIV/AIDS Prevention, Education and Behavioural Science
SP - 30
EP - 36
PB - Science Publishing Group
SN - 2575-5765
UR - https://doi.org/10.11648/j.ijhpebs.20251101.14
AB - Background: The aims of this study were to assess the frequency of lower extremity arterial occlusive disease in HIV-positive patients on antiretroviral therapy by measuring the ankle-brachial index (ABI) and to examine the links between the HIV condition, antiretroviral therapy administration, and associated cardiovascular risk factors. Methods: This was a descriptive and analytical cross-sectional study with prospective data collection, conducted from May 1st to June 30th, 2022. Included were HIV-positive patients on antiretroviral therapy after signing an informed consent. The collected data included particularly the systematic and bilateral measurement of the ankle-brachial index. Any difference less than 0.05 was considered statistically significant. Results: Our study was conducted on 150 patients. There was a female predominance with a sex ratio of 0.58. The average age was 46.78±12.37 years. The main cardiovascular risk factors identified were dyslipidemia (51.6%), hypertension (19.5%), smoking (6.9%), and diabetes (3.4%). The duration of HIV infection over 15 years was most represented at 37.6%. The frequency of PAD was 55.2%. Among these, 37.6% had poorly compensated PAD. There was a correlation between PAD and smoking (p=0.029), dyslipidemia (p=0.02), and the duration of HIV infection between 6 and 10 years (p=0.039). Conclusion: Our study shows a very high frequency of PAD in patients living with HIV and highlights the importance of the ABI in screening for PAD in this patient group.
VL - 11
IS - 1
ER -
Ngaïdé, A. A., Gaye, N. D., Mingou, J. S., Haimed, H., Diop, K., et al. (2025). Screening for Lower Limb Arterial Occlusive Disease in HIV Patients on Antiretroviral Therapy: A Monocentric Study of 150 Patients in Dakar, Senegal. International Journal of HIV/AIDS Prevention, Education and Behavioural Science, 11(1), 30-36. https://doi.org/10.11648/j.ijhpebs.20251101.14
Ngaïdé, A. A.; Gaye, N. D.; Mingou, J. S.; Haimed, H.; Diop, K., et al. Screening for Lower Limb Arterial Occlusive Disease in HIV Patients on Antiretroviral Therapy: A Monocentric Study of 150 Patients in Dakar, Senegal. Int. J. HIV/AIDS Prev. Educ. Behav. Sci.2025, 11(1), 30-36. doi: 10.11648/j.ijhpebs.20251101.14
Ngaïdé AA, Gaye ND, Mingou JS, Haimed H, Diop K, et al. Screening for Lower Limb Arterial Occlusive Disease in HIV Patients on Antiretroviral Therapy: A Monocentric Study of 150 Patients in Dakar, Senegal. Int J HIV/AIDS Prev Educ Behav Sci. 2025;11(1):30-36. doi: 10.11648/j.ijhpebs.20251101.14
@article{10.11648/j.ijhpebs.20251101.14,
author = {Aliou Alassane Ngaïdé and Ngoné Diaba Gaye and Joseph Salvador Mingou and Houda Haimed and Karim Diop and Amadou Rassoul Diouf and El Hadji Bara Diop and Marguerite Tennig Diouf and Momar Dioum and Fatou Aw and Simon Antoine Sarr and Alain Affangla and Serigne Mor Beye and Mouhamed Leye and Malick Bodian and Mouhamadou Bamba Ndiaye and Alassane Mbaye and Adama Kane and Maboury Diao and Abdoul Kane},
title = {Screening for Lower Limb Arterial Occlusive Disease in HIV Patients on Antiretroviral Therapy: A Monocentric Study of 150 Patients in Dakar, Senegal},
journal = {International Journal of HIV/AIDS Prevention, Education and Behavioural Science},
volume = {11},
number = {1},
pages = {30-36},
doi = {10.11648/j.ijhpebs.20251101.14},
url = {https://doi.org/10.11648/j.ijhpebs.20251101.14},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ijhpebs.20251101.14},
abstract = {Background: The aims of this study were to assess the frequency of lower extremity arterial occlusive disease in HIV-positive patients on antiretroviral therapy by measuring the ankle-brachial index (ABI) and to examine the links between the HIV condition, antiretroviral therapy administration, and associated cardiovascular risk factors. Methods: This was a descriptive and analytical cross-sectional study with prospective data collection, conducted from May 1st to June 30th, 2022. Included were HIV-positive patients on antiretroviral therapy after signing an informed consent. The collected data included particularly the systematic and bilateral measurement of the ankle-brachial index. Any difference less than 0.05 was considered statistically significant. Results: Our study was conducted on 150 patients. There was a female predominance with a sex ratio of 0.58. The average age was 46.78±12.37 years. The main cardiovascular risk factors identified were dyslipidemia (51.6%), hypertension (19.5%), smoking (6.9%), and diabetes (3.4%). The duration of HIV infection over 15 years was most represented at 37.6%. The frequency of PAD was 55.2%. Among these, 37.6% had poorly compensated PAD. There was a correlation between PAD and smoking (p=0.029), dyslipidemia (p=0.02), and the duration of HIV infection between 6 and 10 years (p=0.039). Conclusion: Our study shows a very high frequency of PAD in patients living with HIV and highlights the importance of the ABI in screening for PAD in this patient group.},
year = {2025}
}
TY - JOUR
T1 - Screening for Lower Limb Arterial Occlusive Disease in HIV Patients on Antiretroviral Therapy: A Monocentric Study of 150 Patients in Dakar, Senegal
AU - Aliou Alassane Ngaïdé
AU - Ngoné Diaba Gaye
AU - Joseph Salvador Mingou
AU - Houda Haimed
AU - Karim Diop
AU - Amadou Rassoul Diouf
AU - El Hadji Bara Diop
AU - Marguerite Tennig Diouf
AU - Momar Dioum
AU - Fatou Aw
AU - Simon Antoine Sarr
AU - Alain Affangla
AU - Serigne Mor Beye
AU - Mouhamed Leye
AU - Malick Bodian
AU - Mouhamadou Bamba Ndiaye
AU - Alassane Mbaye
AU - Adama Kane
AU - Maboury Diao
AU - Abdoul Kane
Y1 - 2025/03/18
PY - 2025
N1 - https://doi.org/10.11648/j.ijhpebs.20251101.14
DO - 10.11648/j.ijhpebs.20251101.14
T2 - International Journal of HIV/AIDS Prevention, Education and Behavioural Science
JF - International Journal of HIV/AIDS Prevention, Education and Behavioural Science
JO - International Journal of HIV/AIDS Prevention, Education and Behavioural Science
SP - 30
EP - 36
PB - Science Publishing Group
SN - 2575-5765
UR - https://doi.org/10.11648/j.ijhpebs.20251101.14
AB - Background: The aims of this study were to assess the frequency of lower extremity arterial occlusive disease in HIV-positive patients on antiretroviral therapy by measuring the ankle-brachial index (ABI) and to examine the links between the HIV condition, antiretroviral therapy administration, and associated cardiovascular risk factors. Methods: This was a descriptive and analytical cross-sectional study with prospective data collection, conducted from May 1st to June 30th, 2022. Included were HIV-positive patients on antiretroviral therapy after signing an informed consent. The collected data included particularly the systematic and bilateral measurement of the ankle-brachial index. Any difference less than 0.05 was considered statistically significant. Results: Our study was conducted on 150 patients. There was a female predominance with a sex ratio of 0.58. The average age was 46.78±12.37 years. The main cardiovascular risk factors identified were dyslipidemia (51.6%), hypertension (19.5%), smoking (6.9%), and diabetes (3.4%). The duration of HIV infection over 15 years was most represented at 37.6%. The frequency of PAD was 55.2%. Among these, 37.6% had poorly compensated PAD. There was a correlation between PAD and smoking (p=0.029), dyslipidemia (p=0.02), and the duration of HIV infection between 6 and 10 years (p=0.039). Conclusion: Our study shows a very high frequency of PAD in patients living with HIV and highlights the importance of the ABI in screening for PAD in this patient group.
VL - 11
IS - 1
ER -