Abstract
Background: Approximately one third of all PLWHA are infected with latent TB infection and HIV`s attack on the immune system greatly increases the risk that latent tuberculosis infection (LTBI) will progress to active TB form. Implementation of a co-infection prevention intervention addresses the HIV counseling and testing for all TB patients and this allows individuals to access comprehensive health care services for both diseases. Recognizing and treating TB in people living with HIV can be advantage to prevent or reduce TB-related morbidity and mortality. General objective of the study: Assess the Anti-TB treatment outcome among HIV positive and negative TB patients. Method: This study was conducted in SNNPR, Hawassa city, Adare Hospital from February 20 to 28/2011. A retrospective comparative cross-sectional quantitative study was conducted on a total of 1000 TB patients (existing facility based secondary data from TB registry book). Data was entered and analyzed using SPSS version17 statistical package. Percentages were calculated to describe all the variables, odd ration with 95% confidence intervals were calculated to assess associations between independent and dependent variables. Result: Only 72.9% were tested for HIV and out of these 32.6% were HIV positive. Among HIV negative patients “treatment success” rate was 85.7% whereas among HIV positive patients was 77.1%. These indicate that individuals with HIV positive its anti-TB treatment outcome is more associated with its HIV sero-status. Conclusion: strengthening of implementation of TB/HIV co-infection intervention and giving attention to those co-infected patients for better quality of care is recommended.
Keywords
Treatment Success, Pulmonary TB- Smear-positive, Pulmonary TB-Smear-negative, Treatment Outcome, No-Treatment Success Rate, TB-HIV Co-Infection, Anti-TB Treatment, HIV Sero-status
1. Introduction
1.1. Background
Tuberculosis (TB) is one of the leading causes of morbidity and mortality among people living with human immunodeficiency virus/ acquired immunodeficiency syndrome (HIV/AIDS.
| [1] | Getahun, H. Synergies in TB/HIV control: what elements need to be included in TB and HIV proposals to the GF? Presentation At the Global Fund and Scientific Policy Seminar in Geneva, Switzerland. October 5, 2007. |
[1]
Despite its effect, the incidence of HIV triggering the rapid increases in the TB epidemic worldwide
| [2] | The World Bank. The World Bank’s Commitment to HIV/AIDS in Africa: Our Agenda for Action, 2007-2011. Washington, DC. The World Bank. 2008b. |
[2]
.
An estimated 2 billion people world-wide are infected with mycobacterium tuberculosis, although the vast majority never become sick or show any symptoms, but especially for people with compromised immune system
| [3] | Open society institute network public health programs. Integrating HIV/AIDS & TB Efforts, The Challenge for the President’s AIDS Initiative; Preliminary report for the U.S. Office of the Global AIDS Coordinator. Open Society Institute: 400 West 59th Street: 2004. New York, NY 10019 USA. |
[3]
.
Approximately one third of all PLWHA are infected with latent TB infection and HIV`s attack on the immune system greatly increases the risk that latent tuberculosis infection (LTBI) will progress to active TB- form 10% life time risk among those who are HIV-negative to 8-10% of PLWHA die within months of developing active TB diseases
| [4] | World Health Organization. Global Tuberculosis Control: a short update to the 2009 report. 2009. Geneva. |
[4]
. Based on the world health organization report; globally among incident TB cases, the estimated HIV prevalence and mortality is 15 and 26 percent respectively (4). Sub-Saharan African countries have the highest rate of TB/HIV co-infection. 70-80% of global TB/HIV co-infected patients are living in this part of the region
| [3] | Open society institute network public health programs. Integrating HIV/AIDS & TB Efforts, The Challenge for the President’s AIDS Initiative; Preliminary report for the U.S. Office of the Global AIDS Coordinator. Open Society Institute: 400 West 59th Street: 2004. New York, NY 10019 USA. |
| [4] | World Health Organization. Global Tuberculosis Control: a short update to the 2009 report. 2009. Geneva. |
[3, 4]
.
With a projected 65 percent of the world HIV/AIDs cases and almost 80 percent of all new case of TB-HIV co-infection, sub-Saharan Africa has borne a disproportionate burden of disease
| [3] | Open society institute network public health programs. Integrating HIV/AIDS & TB Efforts, The Challenge for the President’s AIDS Initiative; Preliminary report for the U.S. Office of the Global AIDS Coordinator. Open Society Institute: 400 West 59th Street: 2004. New York, NY 10019 USA. |
| [4] | World Health Organization. Global Tuberculosis Control: a short update to the 2009 report. 2009. Geneva. |
[3, 4]
.
The incidence rate of TB has been rising much faster in this region than rest of the world. The global incidence of TB is increasing at annual rate of only 0.4 percent. Relative to the global increasing rate; a high average annual increase in incidence over 5 percent is observed in 14 countries including Ethiopia
| [5] | World health organization. Global Tuberculosis Control: Surveillance, Planning, Financing. 2003 report. Geneva. |
[5]
.
TB is the opportunistic infection in HIV- infected patients, and more than 25% of TB patients are co- infected with HIV
| [6] | Odiaibo GN, Gboun MF, Ekanem EE, Gwarzo SN, Saliu L, Egbewunmi SA et al. HIV infection among patients with pulmonary tuberculosis in Nigeria. Afr J Med Sci 2006; 35 Suppl; 93-8. |
[6]
.
Responding to the intimidation posed by TB- HIV co-infection requires integrated service delivery and coordination between TB and HIV programs in endemic countries. Policy recommendations from international technical agencies in the last 1990s reinforced this framework, characterizing TB-HIV as a global health challenge that required “a dual strategy for a dual epidemic”
| [5] | World health organization. Global Tuberculosis Control: Surveillance, Planning, Financing. 2003 report. Geneva. |
[5]
.
Implementation of a co-infection prevention intervention addresses the HIV counseling and testing for all TB patients and this allows individuals to access comprehensive health care services for both diseases. Recognizing and treating TB in people living with HIV can an advantage to prevent or reduce TB-related morbidity and mortality. This creates an opportunity to HIV positive individuals to have an access for a better anti-retroviral treatment for the future
| [7] | Crofton, J. N. Horne, and F. Miller. Clinical Tuberculosis. 2nd ed. London: Macmillan Education LTD 1999. |
[7]
.
Despite these difficulties, organizations like WHO recommends providing appropriate TB therapy for all HIV positive people who test for either the latent or active forms of the disease
.
The stop TB strategy of directly observed therapy short-course (DOTs)-based TB programs help prevention of TB by reducing transmission through prompt identification, diagnosis, and successful treatment of TB
| [9] | World Health Organization. Global tuberculosis control: epidemiology, strategy, financing WHO report 2009. http://whqlibdoc.who.int/publications/2009/9789241598866_eng.pdf |
| [10] | Hanifa Y, Grant AD, Lewis J, Corbett EL, Fielding K, Churchyard G. Prevalence of latent tuberculosis infection among gold miners in South Africa. Int J Tuberc Lung Dis 2009; 13: 39-46. |
| [11] | Castro KG. Tuberculosis as an opportunistic disease in persons infected with human immunodeficiency virus. Clin Infect Dis 1995; 21(Suppl 1): S66-S71. |
[9-11]
. Also strong DOTs-based TB programs are essential, prevention of HIV infection is necessary to control TB in areas impacted by HIV.
Despite determining the prevalence of co-infections; for strengthening the provision of services; addressing factors related to adherence on TB treatment in patients with concomitant TB and HIV, and barriers for HIV testing and counseling on TB clinics/wards has important contribution. Study conducted by Mekides and et al also recommends further study on these barriers
| [12] | Mekdes K, Gunnar BA, Jan FC. Barriers and facilitators of adherence to TB treatment in patients on concomitant TB and HIV treatment: a qualitative study. |
[12]
. Documentation of these factors can create an opportunity for the future to sustain and improve the service delivery of the dual epidemics prevention intervention.
1.2. Statement of the Problem
The number of HIV-positive TB cases and deaths were estimated at 1.39 million cases (15% of all incident cases) and 0.48 million deaths, which was 24% of the estimated two million HIV deaths in 2007
| [4] | World Health Organization. Global Tuberculosis Control: a short update to the 2009 report. 2009. Geneva. |
[4]
. It also revealed that HIV infected patients had a significantly higher prevalence (20.2%) of tuberculosis compared to those individuals who were negative for HIV (3.2%)
| [13] | Maro I, Mgonda Y. Prevalence, Modes of Management, and Treatment outcomes among Patients with HIV/AIDS and Tuberculosis Co-infections in Dar es Salaam, 2005. Dar es Salaam: Tanzania. |
[13]
.
It is estimated that 33% of all AIDs deaths worldwide can be directly attributed to TB. In sub-Saharan Africa this increases to 50%
. About fifteen percent of the incident TB cases in 2008 are estimated to be co-infected with human immunodeficiency virus (HIV)
| [4] | World Health Organization. Global Tuberculosis Control: a short update to the 2009 report. 2009. Geneva. |
[4]
. TB is the leading direct cause of death among PLWH in Africa and a major cause of death elsewhere
| [15] | Munsiff SS, Alpert PL, Gourevitch MN, Chang CJ, Klein RS. A prospective study of tuberculosis and HIV disease progression. 1998. J Acquire Immune Defic Syndr Hum Retrovirol 19: 361–6. |
| [16] | Corbett EL, Watt CJ, Walker N, Maher D, Williams BG, et al. The growing burden of tuberculosis: global trends and interactions with the HIV epidemic. 2003. Arch Intern Med 163: 1009–21. |
[15, 16]
. In people living with HIV, HIV infection increases the risk of progressing from TB infection to TB disease
| [17] | Mendelson M. Diagnosing tuberculosis in HIV-infected patients: challenges and future prospects. 2007. Br Med Bull 81–82: 149–65. |
[17]
. Also there seems to be consensus that TB does accelerate HIV replication, the impact of TB disease on HIV disease progression at the population level is less clear
| [18] | Amo J, Perez-Hoyos S, Hernandez Aguado I, Diez M, Castilla J, et al. Impact of tuberculosis on HIV disease progression in persons with well-documented time of HIV sero-conversion. 2003. J Acquir Immune Defic Syndr 33: 184–90. |
[18]
.
An HIV negative person with a latent TB infection has a ten percent chance of progressing to active TB over his or her entire lifetime, whereas an HIV positive person has a ten percent chance of developing active TB each year
. These all studies indicate how much TB and HIV are associated and have dual impact on the health of the population.
HIV has an impact on TB by reactivating and progression of the disease and increasing mortality and morbidity. It also creates challenge on the diagnosis of TB diseases. Its impact is not only limited on these factors it is also the reason for treatment complication. In order to prevent the effect of HIV on TB the world health organization has launches the dual prevention intervention of both diseases in an integrated approach.
Some studies that were conducted in the region by B Shargie et al
| [20] | Estifanos S B, Bernt L. Determinants of Treatment Adherence among Smear-Positive Pulmonary Tuberculosis Patients in Southern Ethiopia. |
[20]
and in Gondar university teaching hospital of North Ethiopia
| [21] | Belay T, Abebe M, Assegedech B, Dieter R, Frank E Ulrich S. Treatment outcome of tuberculosis patients at Gondar University Teaching Hospital, Northwest Ethiopia. Gonder, Ethiopia. |
[21]
revealed that TB treatment success rate is not more than 50%. In addition of these; those all TB patients who registered for TB treatment are also offered HIV counseling and testing. But data obtained from the SNNPR health bureau revealed that from the total of 10,525 TB patients, only 6,520 (61%) were tested for HIV
| [22] | SNNPR RHB. 2109/10 annual regional health report. Hawassa, SNNPR. |
[22]
. The study in Gondar also indicated that a high proportion of patients died (10.1%) or defaulted (18.3%), these indicates that there is a need for strengthen the implementation of the dual infections intervention
| [21] | Belay T, Abebe M, Assegedech B, Dieter R, Frank E Ulrich S. Treatment outcome of tuberculosis patients at Gondar University Teaching Hospital, Northwest Ethiopia. Gonder, Ethiopia. |
[21]
. In order to improve the implementation of the co-infection prevention there is a need to describing factors affecting the implementation of the program and, further knowing the level of HIV prevalence among TB patients, and the effects of HIV on TB treatment outcome are necessary.
1.3. Rationale of the Research
Prevention of TB/HIV co-infection is one of the interventions used to reduce the prevalence of HIV among TB suspected individuals.
Responding to the threat posed by TB- HIV co-infection requires integrated service delivery and coordination between TB and HIV programs in endemic countries. Policy recommendations from international technical agencies in the last 1990s reinforced this framework, characterizing TB-HIV as a global health challenge that required “a dual strategy for a dual epidemic
| [22] | SNNPR RHB. 2109/10 annual regional health report. Hawassa, SNNPR. |
[22]
. However, there are only limited studies conducted in the assessment of these interrelated diseases and compliance of TB/HIV co-infected patients for TB treatment.
Therefore this study aimed to assess the Anti-TB treatment outcome among HIV positive TB patients in contrast to HIV negative TB patients. The findings of this research helped to identify barriers and gaps and add knowledge on the betterment of the implementation of the program in the study area and other part of the region as well as to generate hypothesis.
2. Objectives of the Research
2.1. General Objective
Assess the Anti-TB treatment outcome among HIV positive and negative TB patients
2.2. Specific Objectives
1) To assess the level of compliance of TB patients for HIV testing
2) Determine the magnitude of HIV prevalence among TB patients
3) To compare Anti-treatment outcome in terms of cure, default and death rates between HIV positive and negative TB patients.
3. Methods
3.1. Study Area and Design
This study was conducted in SNNPR, Hawassa city administrative zone, in Hawassa city, Adare Hospital from February 20 to 28/2011. Hawassa is the capital city of the southern nations, nationalities’ and people regional state and Hawassa city administration. Hawassa is 265 KMs far from Addis Ababa. Based on the 2007 national census result, in 2010/11 the total population of the Hawassa and its catchment is estimated to be 179,393
| [23] | Awassa city administration health Department. Hawassa city administration 2009/10 annual health report. Hawassa, SNNPR. |
[23]
.
Annually more than 179,393 new patients and 18,393 repeated patients were attended in the health facilities found in the city. In 2010 the health service utilization per capita of the zone was.99
| [23] | Awassa city administration health Department. Hawassa city administration 2009/10 annual health report. Hawassa, SNNPR. |
[23]
.
A total of 165 different health professionals are serving the zonal population. Based on the city health department profile; 1 physician serve for 70,567 peoples and 1 nurse for 2,918 people
| [23] | Awassa city administration health Department. Hawassa city administration 2009/10 annual health report. Hawassa, SNNPR. |
[23]
.
At city administrative level the leading cause responsible for morbidity and mortality is malaria. TB is one of the major public health problems in the city. Annually more than 420 new and repeated TB cases were reported from the Health facilities in the city administration.
A retrospective cross-sectional quantitative study was conducted on the existing facility based secondary data from TB registration book.
3.2. Study Population
3.2.1. Source Population
All TB patients registered at Adare hospital during the two years, from July 2008 to June 2010.
3.2.2. Sample Size
All 1000 TB patients registered at Adare hospital during the two years, from July 2008 to June 2010 who followed Dots treatment were included in the study.
3.3. Data Collection
3.3.1. Data Collection Procedure
TB registered book was retrieved from the records in the hospital. Two data Clarks were trained to collect the data from the records according to a checklist format prepared by the investigator. One supervisor was involved in the study in the day to day checking of the data.
3.3.2. Variables
Dependent variable was Anti-TB treatment outcome in terms of cure, default and death, treatment completed and transferred.
Independent variables were age, sex, and HIV status, TB classification.
3.3.3. Operational Definitions
According to the standard definitions of the National Tuberculosis and Leprosy Control Program guideline (NLCP) adopted from WHO
| [24] | Deribew A, Tesfaye M, Hailmichale Y, N Nebiyu, Daba S, Wogi A, Belachew T, Apers L, Colebunders R. Tuberculosis and HIV co-infection: its impact on quality of life. Published online 2009 December 29. https://doi.org/10.1186/1477-7525-7-105 |
[24]
, the following clinical case and treatment outcome definitions were used:
Pulmonary TB, smear-positive: A patient with at least two sputum specimens which were positive for acid-fast bacilli (AFB) by microscopy, or a patient with only one sputum specimen which was positive for AFB by microscopy, and chest radiographic abnormalities consistent with active pulmonary TB.
Pulmonary TB, smear-negative: A patient with symptoms suggestive of TB, with at least two sputum specimens which were negative for AFB by microscopy, and with chest radiographic abnormalities consistent with active pulmonary TB (including interstitial or miliary abnormal images), or a patient with two sets of at least two sputum specimens taken at least two weeks apart, and which were negative for AFB by microscopy, and radiographic abnormalities consistent with pulmonary TB and lack of clinical response to one week of broad spectrum antibiotic therapy.
Extra pulmonary TB (EPTB): This included tuberculosis of organs other than the lungs, such as lymph nodes, abdomen, genitourinary tract, skin, joints and bones, meninges, etc. Diagnosis of EPTB was based on fine needle aspiration cytology or biochemical analyses of cerebrospinal/pleural/ascetic fluid or histo-pathological examination or strong clinical evidence consistent with active extra-pulmonary tuberculosis, followed by a decision of a clinician to treat with a full course of anti-tuberculosis chemotherapy. In all the cases of EPTB, sputum examinations and chest radiographs were used to investigate the involvement of lung parenchyma. This hospital lacks the facilities for culture and drug susceptibility testing.
Treatment Outcome: The treatment outcome was divided into seven categories according to NTLCP guideline. These categories were: cured (finished treatment with negative bacteriology result at the end of treatment), completed treatment (finished treatment, but without bacteriology result at the end of treatment), failure (remaining smear positive at five months despite correct intake of medication), defaulted treatment (patients who interrupted their treatment for two consecutive months or more after registration), died (patients who died from any cause during the course of treatment), transferred out (patients whose treatment results are unknown due to transfer to another health facility) and successfully treated (A patient who was cured or completed treatment).
Treatment success rate: Is those complete their full course of DOTs treatment and cured from TB.
No-Treatment success rate: Is those individuals who were died, transferred, failure to respond to the treatment or transferred out to another health facility during follow DOTS treatment in the facility where they start treatment.
3.3.4. Data Processing and Analysis
Data was entered and analyzed using SPSS version17 statistical package. Percentages were calculated to describe all the variables, odd ration with 95% confidence intervals were calculated to assess associations between independent and dependent variables.
3.4. Ethical Consideration
Permission was obtained from the regional health bureau, health research and technology transfer process.
4. Result
Characteristics of study subjects
Table 1. Description of study subjects by Age, sex and TB types (n=1000).
Characteristics | Number (n) | Percentage (%) |
Age | | |
0-14 | 120 | 12 |
15-24 | 332 | 33.3 |
25-34 | 296 | 29.7 |
35-49 | 154 | 15.4 |
50 and above | 95 | 9.5 |
Mean (SD) | 27.52 (14.833) | |
Sex | | |
Male | 633 | 63.3 |
Female | 367 | 36.7 |
TB classification | | |
Smear negative PTB | 416 | 41.7 |
Smear Positive PTB | 340 | 34.1 |
EPTB | 241 | 24.2 |
HIV Tested | | |
Yes | 729 | 72.9 |
No | 271 | 27.1 |
As shown in
Table 1, 12% (120) of patients were in the age group 0-14, 33.3% (332) 15-24, 29.7% (296) 25-34, 15.4% (154) 35-49, 9.5% (95) 50 years and above. The mean age was 27.52 (SD=14.833). Concerning sex of the study subjects 63.3% (633) were males and 36.7% (367) females.
41.7% (416) were smear-negative PTB, 34.1% (340) smear-positive PTB and 24.2% (241) were EPTB by type. Of the total TB patients offered HIV test 729 (72.9%) were tested.
Table 2. HIV Sero-status of study subjects by age, sex and type of TB (n=729).
Characteristics | HIV negative (%) | HIV positive (%) |
491 (67.4) | 238 (32.6) |
Age | | |
0-14 | 51 (71.8) | 20 (28.2) |
15-24 | 199 (82.6) | 42 (17.4) |
25-34 | 130 (55.8) | 103 (44.2) |
35-49 | 57 (48.7) | 60 (51.3) |
50 and above | 54 (80.6) | 13 (19.4) |
Sex | | |
Male | 345 (73.7) | 123 (26.3) |
Female | 146 (55.9) | 115 (44.1) |
TB classification | | |
Smear negative PTB | 172 (57.7) | 126 (42.3) |
Smear Positive PTB | 193 (77.2) | 57 (22.8) |
EPTB | 125 (69.4) | 55 (30.6) |
Table 2 shows that those who were tested for HIV (n=729), 238 were HIV positive making the overall prevalence 32.6%.
The prevalence of HIV was higher (51.3%) in the age group 35-49 followed by age group 25-34 (44.2%) and age group 0-14 (28.2%). The lowest prevalence (17.4%) was in the age group 15-24. Females had higher HIV prevalence (44.1%) as compared to males (28.4%).
Higher HIV prevalence was observed in those smear negative PTB patients (42.3%) followed by EPTB (30.6%) and lower in smear positive PTB patients (22.8%). Percentage of HIV negative TB patients that are smear positive PTB was 39.4% and percentage of HIV positive TB patients that smear positive PTB was 23.9%.
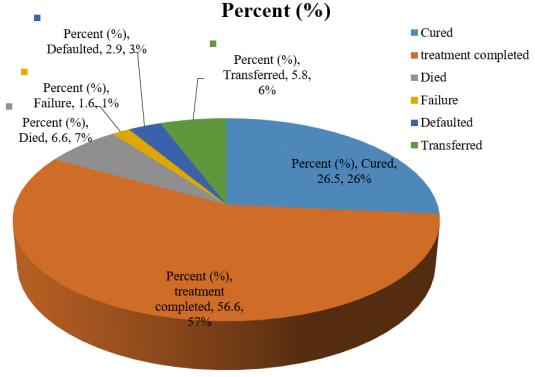
Figure 1. Anti-TB treatment outcome among study subjects (n=982).
As shown in the above figure; from the total of 982 study subjects; 26.5% (260) were cured from TB, 56.6% (556) were completed their full course of TB treatment, 6.6% (65) were “Died”, 1.6% (n=16) were failure to respond to their TB treatment 2.9% (28) were defaulted from their treatment, 5.8% (57) were transferred to other treatment centers. For Bivalent analysis these result was further regrouped and summarized as; 16.9% (66) taken as “no-treatment success” and 83.1% (816) were taken as “treatment success” regardless of their HIV sero-status.
Table 3. Anti-TB treatment outcome by HIV Sero-status (n=717).
HIV test result | TB treatment outcome |
Cured | Treatment completed | Died | Failure | Defaulted | Transferred | Total |
N | % | N | % | N | % | n | % | N | % | n | % | N | % |
Negative | 159 | (33.1) | 253 | (52.6) | 23 | (4.8) | 4 | (.8) | 9 | (1.9) | 33 | (6.9) | 481 | (100) |
Positive | 38 | (16.1) | 144 | (61.0) | 28 | (11.9) | 9 | (3.8) | 6 | (2.5) | 11 | (4.7) | 236 | (100) |
The above table shows that; 27.5% (197) their treatment outcome were cured, 55.4% (397) were treatment completed, 7.1% (51) were Died, 1.8% (13) were failed to respond to their TB treatment 2.1% (15) were Defaulted and 6.1% (44) were Transferred.
When we compare the anti-TB treatment outcome among HIV positive and HIV negative patients; the TB treatment cured rate was 16.1%(38) and 33.1%(159), the treatment complete rate was 61%(144) and 52.6%(253), Death rate was 11.9%(28) and 4.8%(23), treatment failure rate was 3.8% (9) and 8%(4), Defaulter rate was 2.5% (6) and 1.9% (9), Transfer rate was 4.7% (11) and 6.9%(33) respectively.
Table 4. Anti-TB treatment success by HIV status and patient characteristics.
Characteristics | Treatment success | No-treatment success | OR (95% CI) |
n (%) | n (%) |
HIV sero-status | | | |
Negative | 412 (85.7) | 69 (14.3) | 1 |
Positive | 182 (77.1) | 54 (22.9) | 0.564 (0.380, 0.839) |
Age | | | |
0-14 | 92 (80) | 23 (20) | 1 |
15-24 | 280 (85.9) | 46 (14.1) | 1.522 (0.875, 2.646) |
25-34 | 245 (83.3) | 49 (16.7) | 1.250 (0.721, 2.67) |
35-49 | 126 (82.4) | 27 (17.6) | 1.167 (0.629, 2.164) |
50 and above | 70 (76.9) | 21 (23.1) | 0.833 (0.427, 1.624) |
Sex | | | |
Male | 509 (81.3) | 117 (18.7) | 1 |
Female | 307 (86.2) | 49 (13.8) | 1.440 (1.002, 2.069) |
TB classification | | | |
Smear Negative PTB | 331 (81.1) | 77 (18.9) | 1 |
Smear Positive PTB | 271 (81.1) | 63 (18.9) | 1.001 (0.691, 1.448) |
EPTB | 212 (89.5) | 25 (10.5) | 1.973 (1.217, 3.198) |
As shown in the above table; anti-TB treatment success rate was higher (85.7%) among HIV negative than HIV positive TB patients (77.1%) OR=0.564: (95% CI: (0.564, 0.839).
Anti-TB treatment success rate was higher (85.9 %,) in age group 15-24, OR=1.522 (95% CI: 0.875, 2.646) followed by age groups 25-34 (83.3%, OR=1.25 (95% CI: 0.721, 2.67) and 35-49 (82.4%), OR=1.167 (95% CI: 0.629, 2.164) than under 15 age groups. The lowest treatment success rate (76.9%) was observed in age group of 50 and above OR= 0.833 (95% CI: 0.427, 1.624) relative to under 15 (80%).
Females had higher (86.2%) anti-TB treatment success rate as compared to males (81.3%), OR=1.440 (95% CI: 1.002, 2.069).
Concerning Anti-TB treatment outcome in relation to types of TB; higher treatment success rate (89.5%) was observed among EPTB patients, OR=1.973 (95% CI: 1.217, 3.198) than PTB negative patients. However there was no significance difference in treatment success rate among PTB positives (81.1%) and PTB negatives (81.1%) patients, OR=1.001 (95% CI: 0.691, 1.448).
5. Discussion
Based on TB/HIV co-infection prevention intervention all TB patients offered HIV testing. But only 72.9% were tested for knowing their HIV sero-status. This result is relatively higher than the data that obtained from the SNNPR regional health bureau (61%)
| [10] | Hanifa Y, Grant AD, Lewis J, Corbett EL, Fielding K, Churchyard G. Prevalence of latent tuberculosis infection among gold miners in South Africa. Int J Tuberc Lung Dis 2009; 13: 39-46. |
[10]
. In addition of this the rate of TB/HIV co-infection among the study subjects was 32.6%. This finding also supported by study conducted in Gondar University (30-39%)
| [21] | Belay T, Abebe M, Assegedech B, Dieter R, Frank E Ulrich S. Treatment outcome of tuberculosis patients at Gondar University Teaching Hospital, Northwest Ethiopia. Gonder, Ethiopia. |
[21]
. But higher than the Hosanna hospital study (12%)
| [20] | Estifanos S B, Bernt L. Determinants of Treatment Adherence among Smear-Positive Pulmonary Tuberculosis Patients in Southern Ethiopia. |
[20]
. And lower than other studies conducted in different part of Ethiopia (50%)
| [25] | Demissie, M., B. Lindtjon, and B. Tegbaru. 2000. Human immunodeficiency virus (HIV) infection in tuberculosis patients in Addis Ababa. Ethiopia. J. Health Dev. 14: 277–282. |
| [26] | Disease Prevention and Control Department, Ministry of Health, Ethiopia. 2002. Tuberculosis and leprosy prevention and control program manual, 2nd edition, p. 119–120. Ministry of Health, Addis Ababa, Ethiopia. |
| [27] | Eyob, G., S. Goshu, M. Girma, E. Lemma, and A. L. Fontanet. 2002. Increase in tuberculosis incidence among the staff working at the Tuberculosis Demonstration and Training Centre in Addis Ababa, Ethiopia: a retrospective cohort study (1989–1998). Int. J. Tuberc. Lung. Dis. 6: 85–88. |
[25-27]
. This shows that there is a need to strengthening the linkage of both interventions.
Higher prevalence of HIV observed in the age groups of 35-49 (51.3%) followed by 25-34 (44.2%). Comparing the prevalence of HIV among males and female; in females it was higher (44.1%) than males (28.4%). This is might be associated with females’ biological factors for high susceptibility for HIV infection.
A higher HIV prevalence was observed in those negative PTB patients (42.3%) followed by EPTB (30.6%) and positive PTB patients (22.8%). The larger proportion of HIV test reactivity among EPTB and smear negative PTB, and lower proportion among smear positive TB patients might be due to the co-infection effect on the TB diagnosis
| [28] | Harries A, Dye C: Tuberculosis. Annals of Tropical Medicine and Parasitology 2006, 100(5): 415-431. |
| [29] | Liberato IR, de Albuquerque Mde F, Campelo AR, de Melo HR: Characteristics of pulmonary tuberculosis in HIV seropositive and seronegative patients in a Northeastern region of Brazil. Rev Soc Bras Med Trop 2004, 37(1): 46-50. |
| [30] | Maher D, Harries A, Getahun H: Tuberculosis and HIV interaction in sub-Saharan Africa: impact on patients and programmes; implications for policies. Tropical Medicine and International Health 2005, 10: 734-742. |
[28-30]
. The Percentage of HIV negative TB patients that are smear positive PTB was 39.4%. This is lower than estimated proportion in developing countries (45%)
| [31] | Murray CJL, Styblo K, Rouillon A. Health sector priorities review: tuberculosis. In: Jamison DT, MosleyWH, eds. Disease Control Priorities in Developing Countries. New York, NY: Oxford University Press; 1993. |
[31]
. the percentage of HIV positive TB patients that smear positive PTB was 23.9%. This is lower than estimated proportion in developing countries (35%)
| [32] | Edlin BR, Tokars JI, Grieco MH, et al. An outbreak of multidrug-resistant tuberculosis among hospitalized patients with the acquired immunodeficiency syndrome. N Engl J Med. 1992; 326: 1514-1521. |
| [33] | Whalen C, Okwera A, Johnson J, et al. Predictors of survival in human immunodeficiency virus infected patients with pulmonary tuberculosis: the Makerere University-Case Western Reserve University Research Collaboration. AmJ Respir Crit Care Med. 1996; 153(6 pt 1): 1977-1981. |
| [34] | UNAIDS/World Health Organization. Report on the Global HIV/AIDS Epidemic, June 1998. Geneva, Switzerland: UNAIDS/World Health Organization; 1998. |
| [35] | US Bureau of the Census, Population Division, International Programs Center. HIV/AIDS Surveillance Database, January 1997. Washington, DC: United States Bureau of the Census; 1997. |
| [36] | Tuberculosis Control Service, Department of Health, Philippines. National Prevalence Survey, 1997. Manila, Philippines: Dept of Health; 1997. |
[32-36]
.
Regarding anti-TB treatment outcome; cure rate was 26.5%, treatment completed 56.6%, death rate 6.6%, failure 1.6% defaulted 2.9% and transferred rate was 5.8%. In general a high (83.1%) treatment success rate was observed in study subjects irrespective to their HIV sero-status. This treatment success rate is similar with average treatment success rate (83%) of 22 high TB burden countries (HBCs)
| [37] | World Health Organization: Global Tuberculosis Control: Surveillance, Planning, Financing. WHO Report 2005 Geneva: World Health Organization. |
[37]
. Death rate (6.6%) and transferred rate (5.8%) were the main factors for increasing a no-treatment success rate among study subjects. These findings are lower than that of the Gondar University study (died 10.1%, defaulted 18.3%)
| [21] | Belay T, Abebe M, Assegedech B, Dieter R, Frank E Ulrich S. Treatment outcome of tuberculosis patients at Gondar University Teaching Hospital, Northwest Ethiopia. Gonder, Ethiopia. |
[21]
.
The observation of each anti-TB treatment outcome among HIV positive and HIV negative patients shows that; a higher death rate (11.9%) and treatment failure rate (3.8%) were observed among HIV positive TB patients compared to 4.8% death rate and 0.8% treatment failure rate among HIV negative`s. the death rate is more than half of deaths among TB patients might be due to co-infection (4). In this study the death rate among HIV positive and negative TB patents is lower than study conducted in Malawi (29% and 8% respectively)
| [38] | Banerjee AA, Moyo S, Salaniponi F, Harrie A. HIV testing and tuberculosis treatment outcome in a rural district in Malawi. Royal Society of Tropical Medicine and Hygiene 1997; Vol. 91: pp. 707-708. |
[38]
. Cured rate among HIV positive TB patients was lower (16.1%) than that of HIV negative TB patients (33.1%). This finding is lower than that of Malawi study (59% and 84% respectively) (38). However a high treatment completed rate (61.0%) and low transferred rate (4.7%) were observed in HIV positive TB patients when compared to 52.6% treatment completed rate and 6.9% transferred rate among HIV negative TB patients.
HIV negative TB patients had higher (85.7%) treatment success rate than HIV positive TB patients (77.1%), OR=0.564 (95% CI: 0.564, 0.839). this shows that treatment success rate might be significantly affected by HIV sero-status.
Through age groups; high treatment success rate was observed among age groups 15-24 (85.9%), OR=1.522 (95% CI: 0.875, 2.646) followed by 25-34 (83.3%), OR=1.250 (95% CI: 0.721, 2.67). However there is no statistically significant association between anti-TB treatment outcome and age groups. Females had higher (86.2%) treatment success rate than males (81.3%) OR=1.440 (95% CI: 1.002, 2.069).
A higher treatment success rate (89.5%) was observed among EPTB patients OR=1.973 (95% CI: 1.217, 3.198) than both smear positive PTB (81.1%) and smear negative PTB (81.1%) patients, OR=1.001 (95% CI: 0.691, 1.448). These finding are higher than study conducted in Gondar (P/PTB=47.8%, N/PTB=25.7%, and EPTB=26.1%)
| [21] | Belay T, Abebe M, Assegedech B, Dieter R, Frank E Ulrich S. Treatment outcome of tuberculosis patients at Gondar University Teaching Hospital, Northwest Ethiopia. Gonder, Ethiopia. |
[21]
.
6. Conclusion and Recommendation
Based on TB/HIV co-infection prevention all TB patients are offered HIV testing. When we consider the stage of development of the implementation of co-infection prevention; the result which obtained from this study (72%) is promising. Despite this; HIV is one of the main reasons for increasing the rate of changing an individual who infected with latent TB infection to active TB form. Therefore the high prevalence of HIV among TB patients (32%) requires attention to strengthening collaborative approach for tackling the “dual” epidemics.
According to the WHO DOTs implementation strategy the treatment success rate that expected to achieve by developing countries is 85%. Based on the finding of this study; the Anti-TB treatment success rate (83.1%) is satisfactory. However factors contribute for increase in no-treatment success rate such as death and Transferred rate needs consideration.
HIV contributes for increasing TB incidence by affecting the immune system of an individual’s; it also negatively affects the Anti-TB treatment outcome among TB patients. Due to co-infection of HIV/TB; the high death, failure and defaulter rate and low cure rate needs attention for improvement. In addition of this co-infected individuals need more quality of care and service.
The effect of TB/HIV co-infection is not restricted to complicate the TB treatment it also affect the TB diagnosis. Therefore; during the diagnosis of TB in HIV infected individual’s needs special attention.
Finally further studies to determine Anti-TB treatment outcome among HIV positives and negative TB patients is recommended.
7. Possible Limitation of the Study
1) The required information’s/data were not fully registered or obtained from TB registry book.
2) Hence study design is cross-sectional; temporal relationships between exposure and disease were not determined.
Abbreviations
AFB | Acid Fast Bacilli |
AIDS | Acquired Immunodeficiency Syndrome |
ART | Anti Retroviral Treatment |
DOTs | Directly Observed Therapy Short Course |
EPTB | Extra Pulmonary Tuberculosis |
HIV | Human Immunodeficiency Virus |
LTBI | Latent TB Infection |
NTLCP | National Tuberculosis and Leprosy Control Program Guideline |
PLHIV | People Living with HIV/AIDS |
PTB | Pulmonary Tuberculosis |
TB | Tuberculosis |
Author Contributions
Samson Tadiwos is the sole author. The author read and approved the final manuscript.
Conflicts of Interest
The authors declare no conflicts of interest.
References
| [1] |
Getahun, H. Synergies in TB/HIV control: what elements need to be included in TB and HIV proposals to the GF? Presentation At the Global Fund and Scientific Policy Seminar in Geneva, Switzerland. October 5, 2007.
|
| [2] |
The World Bank. The World Bank’s Commitment to HIV/AIDS in Africa: Our Agenda for Action, 2007-2011. Washington, DC. The World Bank. 2008b.
|
| [3] |
Open society institute network public health programs. Integrating HIV/AIDS & TB Efforts, The Challenge for the President’s AIDS Initiative; Preliminary report for the U.S. Office of the Global AIDS Coordinator. Open Society Institute: 400 West 59th Street: 2004. New York, NY 10019 USA.
|
| [4] |
World Health Organization. Global Tuberculosis Control: a short update to the 2009 report. 2009. Geneva.
|
| [5] |
World health organization. Global Tuberculosis Control: Surveillance, Planning, Financing. 2003 report. Geneva.
|
| [6] |
Odiaibo GN, Gboun MF, Ekanem EE, Gwarzo SN, Saliu L, Egbewunmi SA et al. HIV infection among patients with pulmonary tuberculosis in Nigeria. Afr J Med Sci 2006; 35 Suppl; 93-8.
|
| [7] |
Crofton, J. N. Horne, and F. Miller. Clinical Tuberculosis. 2nd ed. London: Macmillan Education LTD 1999.
|
| [8] |
Treating TB and HIV – Healthlink Worldwide. 2003.
http://www.healthlink.org.uk/PDFs/tb‐hiv.pdf
|
| [9] |
World Health Organization. Global tuberculosis control: epidemiology, strategy, financing WHO report 2009.
http://whqlibdoc.who.int/publications/2009/9789241598866_eng.pdf
|
| [10] |
Hanifa Y, Grant AD, Lewis J, Corbett EL, Fielding K, Churchyard G. Prevalence of latent tuberculosis infection among gold miners in South Africa. Int J Tuberc Lung Dis 2009; 13: 39-46.
|
| [11] |
Castro KG. Tuberculosis as an opportunistic disease in persons infected with human immunodeficiency virus. Clin Infect Dis 1995; 21(Suppl 1): S66-S71.
|
| [12] |
Mekdes K, Gunnar BA, Jan FC. Barriers and facilitators of adherence to TB treatment in patients on concomitant TB and HIV treatment: a qualitative study.
|
| [13] |
Maro I, Mgonda Y. Prevalence, Modes of Management, and Treatment outcomes among Patients with HIV/AIDS and Tuberculosis Co-infections in Dar es Salaam, 2005. Dar es Salaam: Tanzania.
|
| [14] |
United Nations Acquired Immune Deficiency Syndrome. The Joint United Nations Programme on HIV/AIDS: 2008 Report on Global Epidemic.
http://www.unaids.org/en/KnowledgeCentre/HIVData/GlobalReport/2008/2008_Global_report.asp
, Accessed on February, 2011.
|
| [15] |
Munsiff SS, Alpert PL, Gourevitch MN, Chang CJ, Klein RS. A prospective study of tuberculosis and HIV disease progression. 1998. J Acquire Immune Defic Syndr Hum Retrovirol 19: 361–6.
|
| [16] |
Corbett EL, Watt CJ, Walker N, Maher D, Williams BG, et al. The growing burden of tuberculosis: global trends and interactions with the HIV epidemic. 2003. Arch Intern Med 163: 1009–21.
|
| [17] |
Mendelson M. Diagnosing tuberculosis in HIV-infected patients: challenges and future prospects. 2007. Br Med Bull 81–82: 149–65.
|
| [18] |
Amo J, Perez-Hoyos S, Hernandez Aguado I, Diez M, Castilla J, et al. Impact of tuberculosis on HIV disease progression in persons with well-documented time of HIV sero-conversion. 2003. J Acquir Immune Defic Syndr 33: 184–90.
|
| [19] |
Stop TB Partnership. Healthlink Worldwide. 2006.
http://www.healthlink.org.uk/PDFs/tb‐hiv.pdf
|
| [20] |
Estifanos S B, Bernt L. Determinants of Treatment Adherence among Smear-Positive Pulmonary Tuberculosis Patients in Southern Ethiopia.
|
| [21] |
Belay T, Abebe M, Assegedech B, Dieter R, Frank E Ulrich S. Treatment outcome of tuberculosis patients at Gondar University Teaching Hospital, Northwest Ethiopia. Gonder, Ethiopia.
|
| [22] |
SNNPR RHB. 2109/10 annual regional health report. Hawassa, SNNPR.
|
| [23] |
Awassa city administration health Department. Hawassa city administration 2009/10 annual health report. Hawassa, SNNPR.
|
| [24] |
Deribew A, Tesfaye M, Hailmichale Y, N Nebiyu, Daba S, Wogi A, Belachew T, Apers L, Colebunders R. Tuberculosis and HIV co-infection: its impact on quality of life. Published online 2009 December 29.
https://doi.org/10.1186/1477-7525-7-105
|
| [25] |
Demissie, M., B. Lindtjon, and B. Tegbaru. 2000. Human immunodeficiency virus (HIV) infection in tuberculosis patients in Addis Ababa. Ethiopia. J. Health Dev. 14: 277–282.
|
| [26] |
Disease Prevention and Control Department, Ministry of Health, Ethiopia. 2002. Tuberculosis and leprosy prevention and control program manual, 2nd edition, p. 119–120. Ministry of Health, Addis Ababa, Ethiopia.
|
| [27] |
Eyob, G., S. Goshu, M. Girma, E. Lemma, and A. L. Fontanet. 2002. Increase in tuberculosis incidence among the staff working at the Tuberculosis Demonstration and Training Centre in Addis Ababa, Ethiopia: a retrospective cohort study (1989–1998). Int. J. Tuberc. Lung. Dis. 6: 85–88.
|
| [28] |
Harries A, Dye C: Tuberculosis. Annals of Tropical Medicine and Parasitology 2006, 100(5): 415-431.
|
| [29] |
Liberato IR, de Albuquerque Mde F, Campelo AR, de Melo HR: Characteristics of pulmonary tuberculosis in HIV seropositive and seronegative patients in a Northeastern region of Brazil. Rev Soc Bras Med Trop 2004, 37(1): 46-50.
|
| [30] |
Maher D, Harries A, Getahun H: Tuberculosis and HIV interaction in sub-Saharan Africa: impact on patients and programmes; implications for policies. Tropical Medicine and International Health 2005, 10: 734-742.
|
| [31] |
Murray CJL, Styblo K, Rouillon A. Health sector priorities review: tuberculosis. In: Jamison DT, MosleyWH, eds. Disease Control Priorities in Developing Countries. New York, NY: Oxford University Press; 1993.
|
| [32] |
Edlin BR, Tokars JI, Grieco MH, et al. An outbreak of multidrug-resistant tuberculosis among hospitalized patients with the acquired immunodeficiency syndrome. N Engl J Med. 1992; 326: 1514-1521.
|
| [33] |
Whalen C, Okwera A, Johnson J, et al. Predictors of survival in human immunodeficiency virus infected patients with pulmonary tuberculosis: the Makerere University-Case Western Reserve University Research Collaboration. AmJ Respir Crit Care Med. 1996; 153(6 pt 1): 1977-1981.
|
| [34] |
UNAIDS/World Health Organization. Report on the Global HIV/AIDS Epidemic, June 1998. Geneva, Switzerland: UNAIDS/World Health Organization; 1998.
|
| [35] |
US Bureau of the Census, Population Division, International Programs Center. HIV/AIDS Surveillance Database, January 1997. Washington, DC: United States Bureau of the Census; 1997.
|
| [36] |
Tuberculosis Control Service, Department of Health, Philippines. National Prevalence Survey, 1997. Manila, Philippines: Dept of Health; 1997.
|
| [37] |
World Health Organization: Global Tuberculosis Control: Surveillance, Planning, Financing. WHO Report 2005 Geneva: World Health Organization.
|
| [38] |
Banerjee AA, Moyo S, Salaniponi F, Harrie A. HIV testing and tuberculosis treatment outcome in a rural district in Malawi. Royal Society of Tropical Medicine and Hygiene 1997; Vol. 91: pp. 707-708.
|
Cite This Article
-
APA Style
Tadiwos, S. (2025). Comparative Study on Anti-TB Treatment Outcome Among HIV Positive and HIV Negative TB Patients at Adare Hospital, Hawassa South Ethiopia. International Journal of HIV/AIDS Prevention, Education and Behavioural Science, 11(1), 9-17. https://doi.org/10.11648/j.ijhpebs.20251101.12
 Copy
|
Copy
|
 Download
Download
ACS Style
Tadiwos, S. Comparative Study on Anti-TB Treatment Outcome Among HIV Positive and HIV Negative TB Patients at Adare Hospital, Hawassa South Ethiopia. Int. J. HIV/AIDS Prev. Educ. Behav. Sci. 2025, 11(1), 9-17. doi: 10.11648/j.ijhpebs.20251101.12
Copy
|
Download
AMA Style
Tadiwos S. Comparative Study on Anti-TB Treatment Outcome Among HIV Positive and HIV Negative TB Patients at Adare Hospital, Hawassa South Ethiopia. Int J HIV/AIDS Prev Educ Behav Sci. 2025;11(1):9-17. doi: 10.11648/j.ijhpebs.20251101.12
Copy
|
Download
-
@article{10.11648/j.ijhpebs.20251101.12,
author = {Samson Tadiwos},
title = {Comparative Study on Anti-TB Treatment Outcome Among HIV Positive and HIV Negative TB Patients at Adare Hospital, Hawassa South Ethiopia
},
journal = {International Journal of HIV/AIDS Prevention, Education and Behavioural Science},
volume = {11},
number = {1},
pages = {9-17},
doi = {10.11648/j.ijhpebs.20251101.12},
url = {https://doi.org/10.11648/j.ijhpebs.20251101.12},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ijhpebs.20251101.12},
abstract = {Background: Approximately one third of all PLWHA are infected with latent TB infection and HIV`s attack on the immune system greatly increases the risk that latent tuberculosis infection (LTBI) will progress to active TB form. Implementation of a co-infection prevention intervention addresses the HIV counseling and testing for all TB patients and this allows individuals to access comprehensive health care services for both diseases. Recognizing and treating TB in people living with HIV can be advantage to prevent or reduce TB-related morbidity and mortality. General objective of the study: Assess the Anti-TB treatment outcome among HIV positive and negative TB patients. Method: This study was conducted in SNNPR, Hawassa city, Adare Hospital from February 20 to 28/2011. A retrospective comparative cross-sectional quantitative study was conducted on a total of 1000 TB patients (existing facility based secondary data from TB registry book). Data was entered and analyzed using SPSS version17 statistical package. Percentages were calculated to describe all the variables, odd ration with 95% confidence intervals were calculated to assess associations between independent and dependent variables. Result: Only 72.9% were tested for HIV and out of these 32.6% were HIV positive. Among HIV negative patients “treatment success” rate was 85.7% whereas among HIV positive patients was 77.1%. These indicate that individuals with HIV positive its anti-TB treatment outcome is more associated with its HIV sero-status. Conclusion: strengthening of implementation of TB/HIV co-infection intervention and giving attention to those co-infected patients for better quality of care is recommended.
},
year = {2025}
}
Copy
|
Download
-
TY - JOUR
T1 - Comparative Study on Anti-TB Treatment Outcome Among HIV Positive and HIV Negative TB Patients at Adare Hospital, Hawassa South Ethiopia
AU - Samson Tadiwos
Y1 - 2025/01/16
PY - 2025
N1 - https://doi.org/10.11648/j.ijhpebs.20251101.12
DO - 10.11648/j.ijhpebs.20251101.12
T2 - International Journal of HIV/AIDS Prevention, Education and Behavioural Science
JF - International Journal of HIV/AIDS Prevention, Education and Behavioural Science
JO - International Journal of HIV/AIDS Prevention, Education and Behavioural Science
SP - 9
EP - 17
PB - Science Publishing Group
SN - 2575-5765
UR - https://doi.org/10.11648/j.ijhpebs.20251101.12
AB - Background: Approximately one third of all PLWHA are infected with latent TB infection and HIV`s attack on the immune system greatly increases the risk that latent tuberculosis infection (LTBI) will progress to active TB form. Implementation of a co-infection prevention intervention addresses the HIV counseling and testing for all TB patients and this allows individuals to access comprehensive health care services for both diseases. Recognizing and treating TB in people living with HIV can be advantage to prevent or reduce TB-related morbidity and mortality. General objective of the study: Assess the Anti-TB treatment outcome among HIV positive and negative TB patients. Method: This study was conducted in SNNPR, Hawassa city, Adare Hospital from February 20 to 28/2011. A retrospective comparative cross-sectional quantitative study was conducted on a total of 1000 TB patients (existing facility based secondary data from TB registry book). Data was entered and analyzed using SPSS version17 statistical package. Percentages were calculated to describe all the variables, odd ration with 95% confidence intervals were calculated to assess associations between independent and dependent variables. Result: Only 72.9% were tested for HIV and out of these 32.6% were HIV positive. Among HIV negative patients “treatment success” rate was 85.7% whereas among HIV positive patients was 77.1%. These indicate that individuals with HIV positive its anti-TB treatment outcome is more associated with its HIV sero-status. Conclusion: strengthening of implementation of TB/HIV co-infection intervention and giving attention to those co-infected patients for better quality of care is recommended.
VL - 11
IS - 1
ER -
Copy
|
Download