Abstract
Background: Sarcopenia has emerged as an important prognostic factor in cirrhosis patients. A standardized definition of sarcopenia was not used in many of the studies. EWGSOP2 2019 guidelines define sarcopenia in an objective manner. Ultrasound-guided measurement of thigh muscle thickness is a validated and cost effective tool for the assessment of muscle quantity. Aim of the study was to evaluate the predictive role of sarcopenia on mortality and complications in cirrhosis patients. Methods: It was a prospective cohort study with 143 consecutive patients each in sarcopenia and no sarcopenia groups. Sarcopenia was diagnosed as per EWGSOP2 guidelines incorporating ultrasound-guided thigh muscle thickness measurement. They were studied at 6 months for development of complications and mortality. Kaplan-Meier analysis was used to compare survival and Cox proportional hazards model was used to determine risk factors of mortality. Results: Cirrhosis patients with sarcopenia [M:F=97:46] and without sarcopenia [M:F=111:32] were followed up for 6 months. Survival analysis showed a six-month cumulative survival of 58.0% (95%CI 57.92-58.08) and 76.2% (95% CI 76.13-76.27) in sarcopenia and no sarcopenia groups respectively (p-value 0.001). Six-month cumulative survival in patients with severe sarcopenia was 23.8% and in non-severe sarcopenia was 70.1% (p-value 0.001). Multivariate analysis showed sarcopenia (HR=1.498,95%CI 1.081-2.148), female sex (HR=1.86,95%CI 1.102-3.089), Child Pugh class C (HR=1.458,95%CI 1.214-1.775) and MELD-Na score>15 (HR=1.122,95%CI 1.068-2.212) as independent predictors of mortality. Complications like ascites, HE, Covid 19 infection and UGI bleed were significantly higher in the sarcopenia group. Conclusion: Sarcopenia is an independent prognostic marker of mortality in cirrhosis patients and is associated with an increased risk of complications. Severe sarcopenia has even poorer outcome.
Keywords
Cirrhosis, Sarcopenia, Ultrasound-guided Thigh Muscle Thickness Measurement
1. Introduction
Predicting prognosis is of utmost importance in the management of cirrhosis. Various prognostic models have been validated, of which the Child-Turcotte-Pugh (CTP) and Model for End-Stage Liver Disease (MELD) scores are commonly used. Since 2002, the MELD score has replaced the CTP score in prioritizing cirrhosis patients for liver transplantation due to its inclusion of only objective laboratory parameters and higher effectiveness in predicting short-term clinical outcomes.
Sarcopenia is a condition characterized by adverse muscle changes, either physiological or pathological, resulting in impaired muscle contractile strength, reduced muscle quantity or quality, and diminished muscle function. It is frequently observed in cirrhosis patients, and researchers have also investigated its potential role in predicting prognosis.
None of the aforementioned prognostication systems has included nutritional or muscle status. This may be attributed to the challenges posed by the heterogeneous definitions of malnutrition and sarcopenia, as well as the complexity of nutritional assessment in cirrhosis patients. Many previous studies did not utilize a standardized definition of sarcopenia and relied on CT or MRI for skeletal muscle measurement. However, the measurement of ultrasound-guided thigh muscle thickness (TMT) offers a validated, cost-effective, and easy method for assessing muscle quantity
| [1] | Tandon P, Low G, Mourtzakis M, Zenith L, Myers RP, Abraldes JG, et al. A Model to Identify Sarcopenia in Patients With Cirrhosis. Clin Gastroenterol Hepatol. 2016; 14(10): 1473-1480. e3. |
[1]
. The EWGSOP2 guidelines provide a comprehensive and easily reproducible definition of sarcopenia based on muscle strength, muscle quantity or quality, and physical performance
| [2] | Cruz-Jentoft AJ, Bahat G, Bauer J, Boirie Y, Bruyère O, Cederholm T, et al. Sarcopenia: Revised European consensus on definition and diagnosis. Age and Ageing. 2019; 48(1): 16-31. |
[2]
.
There is a paucity of Indian studies analysing the prognostic role of sarcopenia in cirrhosis. Only a few studies have defined sarcopenia according to the EWGSOP2 guidelines and utilized ultrasound-guided muscle measurements.
This study aimed to examine the prognostic value of sarcopenia, as assessed by the EWGSOP2 guidelines incorporating ultrasound-guided TMT measurements, in predicting mortality and complications in cirrhosis patients.
2. Methods
2.1. Study Population
This prospective cohort study was conducted in a tertiary care centre in Kerala, southern India. Institutional ethical committee approval was obtained before initiating the study. The total duration of the study was 1 year, which included a recruitment period of 6 months and a follow-up period of 6 months. Patients aged between 18 and 80 years with a diagnosis of cirrhosis were included in the study. Patients with hepatocellular carcinoma (HCC), other active malignancies, significant chronic diseases, bedridden patients, and patients with advanced grades of hepatic encephalopathy (HE) who were unable to undergo tests of physical performance were excluded. There were 143 consecutive patients in both the sarcopenia and no sarcopenia groups.
2.2. Assessment and Grading of Sarcopenia
The EWGSOP2 guidelines 2019 were utilized for the diagnosis and grading of sarcopenia. During the initial encounter in the outpatient department or ward, patients underwent an assessment of grip strength in their dominant hand using the PROSMART™ digital hand dynamometer. The peak value of three consecutive readings was used for analysis. Grip strength values below 27 kg in men and below 16 kg in women were considered indicative of probable sarcopenia. If the grip strength was normal, the patient was classified as having "no sarcopenia."
Patients with probable sarcopenia then underwent testing for muscle quantity to confirm the diagnosis. For this, the right TMT was measured in the supine position using ultrasound (MINDRAY™). Points were marked at one-third and one-half of the total distance from the top of the patella to the iliac crest. Featherweight readings were taken at each of these points, with the probe applied without pressure. These readings were averaged and corrected for height (divided by the square of height) to obtain the average feather index. Both the average feather index and body mass index (BMI) were used to determine sarcopenia based on sex-specific nomograms available
| [1] | Tandon P, Low G, Mourtzakis M, Zenith L, Myers RP, Abraldes JG, et al. A Model to Identify Sarcopenia in Patients With Cirrhosis. Clin Gastroenterol Hepatol. 2016; 14(10): 1473-1480. e3. |
[1]
. Patients with values within the normal range were classified as having "no sarcopenia."
Once the diagnosis was confirmed, the severity of sarcopenia was assessed through testing of physical performance. A gait speed test was utilized for this purpose. The patient's usual walking speed over a distance of 4 meters was measured using a stopwatch. A cutoff speed of ≤ 0.8 m/s was considered indicative of severe sarcopenia.
2.3. Outcome Measurement
Standard dietary and exercise advice was given to all patients at the time of enrolment. Patients were followed up for 6 months or until liver transplantation (LT) or death, whichever occurred first. They were assessed for 6-month mortality, as well as the development of complications such as variceal bleeding, HE, bacterial infections like spontaneous bacterial peritonitis (SBP), cellulitis, urinary tract infections (UTI), lower respiratory tract infections (LRTI), hepatorenal syndrome (HRS), acute on chronic liver failure (ACLF), and the development of HCC. These outcomes were compared between patients with sarcopenia and those without sarcopenia. Additionally, mortality and complications were compared between patients with non-severe sarcopenia and those with severe sarcopenia.
2.4. Statistical Analysis
The data were analysed using IBM SPSS statistics software for Windows, version 21.0. Patient characteristics were presented as frequencies, percentages and medians. Comparisons between groups were made with the Chi-square test and independent sample t-test as appropriate. Survival was estimated with the Kaplan-Meier survival method, and comparisons between groups were made with the log-rank test. The influence of sarcopenia on mortality was assessed with a Cox proportional hazards regression model. p values of less than 0.05 were considered to indicate statistical significance.
3. Results
3.1. Baseline Patient Characteristics
143 patients each were included in sarcopenia and no sarcopenia groups. The baseline characteristics of these patients are compared in
Table 1.
Table 1. Baseline Patient Characteristics.
Characteristics | Sarcopenia Group (N1=143) | No Sarcopenia Group (N2=143) |
MALE:FEMALE | 97:46 | 111:32 |
AGE IN YEARS | 58 (51-64) | 54 (46.25-60) |
AETIOLOGY (%) | | |
1. ALCOHOL | 40.55 | 58.04 |
2. NAFLD | 32.16 | 16.08 |
3. HBV | 6.29 | 9.79 |
4. AUTO IMMUNE | 4.19 | 5.59 |
5. HCV | 3.49 | 1.39 |
6. BUDD CHIARI | 2.09 | 5.59 |
7. WILSON | 0.69 | 0 |
8. CRYPTOGENIC | 6.99 | 3.49 |
9. OTHERS | 3.49 | 0 |
CORRECTED BMI (Kg/M2) | 19.93 (18.06-21.54) | 22.60 (19.81-24.84) |
HAND GRIP STRENGTH (Kg) | 17.82 ± 5.335 | 27.86 ± 8.916 |
BILIRUBIN (mg/dL) | 2.53 ± 1.889 | 2.84 ± 1.11 |
ALBUMIN (g/dL) | 2.84 ± 0.50 | 3.12 ± 1.06 |
INR | 1.84 ± 0.676 | 1.66 ± 0.55 |
SODIUM (mEq/L) | 133.45 ± 5.33 | 135.67 ± 3.42 |
CREATININE (mg/dL) | 1.28 ± 0.47 | 1.09 ± 0.45 |
MELD Na SCORE | 20.03 ± 7.42 | 16.87 ± 6.44 |
CTP CLASS (%) | | |
1. A | 8.39 | 26.57 |
2. B | 54.55 | 45.45 |
3. C | 37.06 | 27.97 |
Data presented as medians with IQR, mean ± SD or percentages |
3.2. Survival Analysis
Survival analysis was conducted on 143 patients each in the sarcopenia and no sarcopenia groups. Kaplan-Meier plot was utilized to estimate survival, while the Cox proportional hazards regression model was employed to assess how the covariates impact survival.
Overall Survival of the Study Population
During the 6-month follow-up period, a total of 60 patients in the sarcopenia group and 34 patients in the no sarcopenia group died. One patient from each group underwent LT.
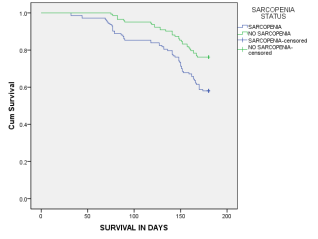
Figure 1 displays the survival curves based on the sarcopenia status.
Figure 1. Survival curves based on sarcopenia status.
The six-month cumulative survival rate in the sarcopenia group was 58.0% (95% CI 57.92-58.08), while in the no sarcopenia group, it was 76.2% (95% CI 76.129-76.271). The survival curves exhibit a significant separation, with a log rank p-value of 0.001, indicating high statistical significance.
3.3. Univariate Analysis of Other Covariates Predicting Mortality
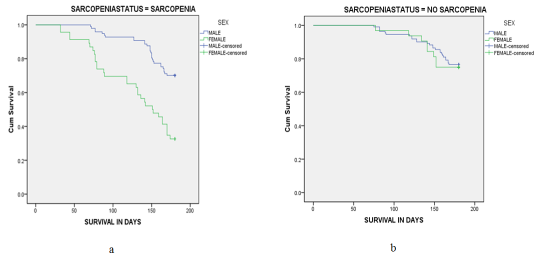
The six-month cumulative survival rate in males was 73.6% (95% CI 73.54-73.66), whereas in females was 50.0% (95% CI 49.81-50.11). The survival curves show a significant separation, with a log rank p-value of <0.001, indicating a strong statistical association between female gender and mortality. In subgroup analysis, it was observed that the six-month cumulative survival rate in males was 70.1% in the sarcopenia group and 76.6% in the no sarcopenia group. Among females, the six-month cumulative survival rate was 32.6% in the sarcopenia group and 75% in the no-sarcopenia group. Notably, females with sarcopenia had poorer survival compared to females without sarcopenia.
Figure 2 shows survival based on gender in both groups.
Figure 2. Survival curves based on gender in (a) sarcopenia group (b) no sarcopenia group.
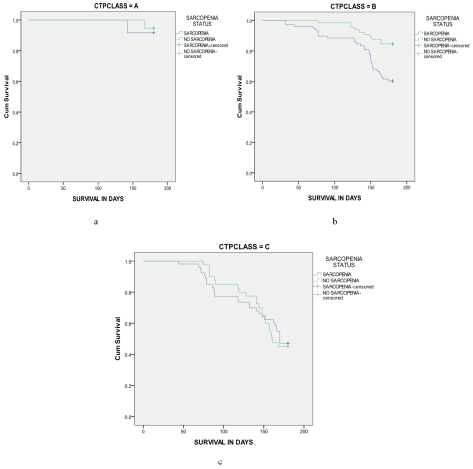
Figure 3. Child-Pugh class and survival a) CTP A b) CTP B c) CTP C.
The six-month cumulative survival rates were 94% (95% CI 93.93-94.06) in Child-Pugh class A, 71.3% (95% CI 71.22-71.37) in class B, and 46.2% (95% CI 45.89-46.30) in class C. The survival curves showed a significant separation, with a log rank p-value of <0.001, indicating a statistically significant association between mortality and the Child-Pugh class.
On analysing the survival functions of Child-Pugh classes separately, it was observed that the presence of sarcopenia was more statistically associated with mortality in patients with Child-Pugh class B than in those with class A or C with a log rank p-value of 0.035.
Figure 3 shows survival based on Child-Pugh class.
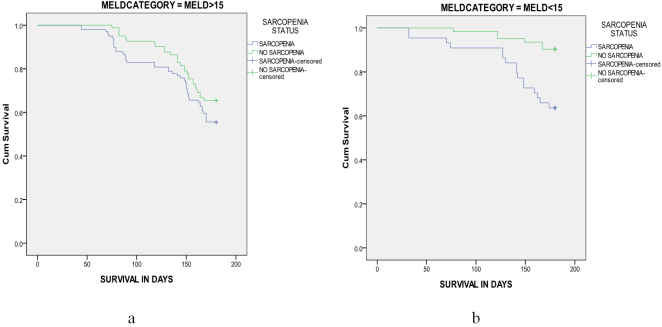
As expected, higher MELD-Na scores were associated with poorer survival. The six-month cumulative survival rate in patients with a MELD-Na score <15 was 79.2% (95% CI 79.12-79.28), while it was 60.0% (95% CI 59.92-60.07) in patients with a MELD-Na score >15. The survival curves displayed a significant separation, with a log rank p-value of 0.001, indicating a strong statistical association between mortality and higher MELD-Na scores.
The importance of sarcopenia as a prognostic marker of cirrhosis patients can be inferred by analysing the survival data of patients with MELD-Na score <15 and >15, considering the presence or absence of sarcopenia. The six-month cumulative survival rate significantly decreases in patients with a MELD-Na score <15 when sarcopenia is present. The survival curves show a substantial separation, with a log rank p-value of 0.004, indicating a significant statistical association. (
Figure 4)
Figure 4. MELD-Na score and survival (a) MELD-Na <15 (b) MELD-Na>15.
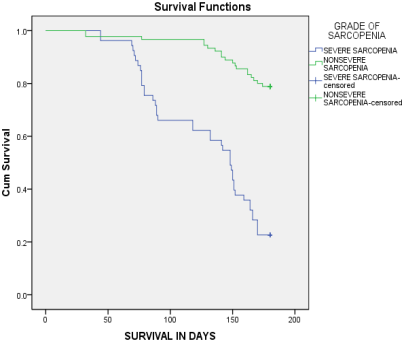
3.4. Grade of Sarcopenia and Mortality
In the sarcopenia group, 53 patients (37.1%) had severe sarcopenia, and 90 (62.9%) had non-severe sarcopenia. The six-month cumulative survival rate in the severe sarcopenia group was 23.8% (95% CI 23.6-23.9) and in the non-severe sarcopenia group was 70.1% (95% CI 70.01-70.18). The difference between the two groups was found to be statistically significant with a Log rank p-value of 0.001. (
Figure 5)
Figure 5. Survival curves based on grade of sarcopenia.
3.5. Multivariate Analysis of Factors Predicting Mortality
Multivariate analysis was done by Cox proportional hazards model. Multivariate analysis showed sarcopenia (HR=1.498, 95%CI 1.081-2.148, p=0.032), female sex (HR=1.860, 95%CI 1.102-3.089, p=0.018), CTP class C (HR=1.458, 95%CI 1.214-1.775, p=0.002) and MELD score > 15 (HR=1.122, 95%CI 1.068-2.212, p=0.05) as independent predictors of mortality. (
Table 2).
Table 2. Analysis Of Predictors Of Mortality.
Characteristic | Univariate Analysis | Multivariate Analysis |
6 month survival (%) | P value | Hazard ratio | P value |
1. SEX | | | | |
MALE | 73.6 | <0.001 | 1.860 (95%CI 1.102-3.089) | 0.018 |
FEMALE | 50.0 |
2. AETIOLOGY | | | | |
ALCOHOL | 68.3 | 0.068 | --- | --- |
NAFLD | 64.9 |
HEP B | 84.2 |
HEP C | 80.0 |
BUDD CHIARI | 50.0 |
AUTO IMMUNE | 66.7 |
CRYPTOGENIC | 50.0 |
3. NUTRITIONALSTATUS | | | | |
UNDERWEIGHT | 53.7 | 0.003 | 1.012 (95% CI 0.842-2.115) REFERENCE | 0.124 |
NORMALWEIGHT | 66.9 |
OVERWEIGHT | 90.9 |
OBESE | 71.4 |
4. SARCOPENIA STATUS | | | | 0.032 |
SARCOPENIA | 58.0 | 0.001 | 1.498 (95%CI 1.081-2.148) | |
NO SARCOPENIA | 76.2 |
5. BILIRUBIN | | | | |
<2 | 72.1 | 0.001 | 1.027 (95%CI 0.946-1.115) | 0.520 |
≥2 | 50.7 |
6. ALBUMIN | | | | |
<2.8 | 53.1 | 0.001 | 0.989 (95%CI 0.951-1.325) | 0.48 |
≥2.8 | 76.3 |
7. INR | | | | |
<1.7 | 76.2 | <0.001 | 1.112 (95%CI 0.754-1.821) | 0.098 |
≥1.7 | 54.2 |
8. CREATININE | | | | |
<1.5 | 68.8 | 0.49 | --- | --- |
≥1.5 | 59.2 |
9. SODIUM | | | | |
<130 | 46.3 | 0.001 | 0.978 (95%CI 0.854-1.235) | 0.229 |
≥130 | 70.6 |
| 94.0 | <0.001 | REFERENCE 1.458 (95%CI 1.214-1.775) | 0.002 |
B | 71.3 |
C | 46.2 |
11. MELD Na SCORE | | | | |
≤15 | 79.2 | 0.001 | 1.122 (95%CI 1.068-2.212) | 0.05 |
>15 | 60.0 |
3.6. Complications at 6 Months Follow up
Both the sarcopenia and the no sarcopenia groups were followed up for 6 months for various complications of cirrhosis. Development of complications like ascites, HE, SARS-CoV-2 (covid-19) infection and upper GI bleeding were significantly higher in the sarcopenia group, while SBP, HRS, cellulitis, UTI, HCC and ACLF were not statistically significant between the two groups. (
Table 3)
Table 3. Complications And Sarcopenia Status.
COMPLICATION | FREQUENCY (%) | P VALUE |
SARCOPENIA GROUP | NO SARCOPENIA GROUP |
ASCITES | 27.04 | 15.22 | 0.019 |
HEPATIC ENCEPHALOPATHY | 34.43 | 15.94 | 0.001 |
SBP | 20.49 | 15.21 | 0.266 |
HRS-AKI | 9.01 | 9.42 | 0.911 |
COVID 19 | 18.85 | 2.89 | <0.001 |
UTI | 1.63 | 2.17 | 0.754 |
CELLULITIS | 6.56 | 0.72 | 0.160 |
UGI BLEED | 11.48 | 6.52 | 0.010 |
ACLF | 1.64 | 1.47 | 0.895 |
HCC | 4.09 | 3.62 | 0.370 |
4. Discussion
This study was intended to assess the predictive role of sarcopenia in mortality and complications among patients with cirrhosis. The study population included 286 patients with liver cirrhosis, divided into two groups: one with sarcopenia and the other without sarcopenia, with 143 patients in each group.
Although there has been a recent surge in interest in utilizing sarcopenia to predict outcomes in cirrhosis patients, most studies did not use a standardized definition for sarcopenia. Many of these studies relied on cross-sectional imaging, which may not be easily accessible. In our study, a standardized algorithm was utilised for diagnosing sarcopenia and a novel method for assessing muscle quantity, that is ultrasound-guided TMT measurement.
Sarcopenia has a higher prevalence among males, a pattern observed in both cirrhotic and non-cirrhotic populations. In a study conducted by Peng et al., the prevalence of sarcopenia in males with cirrhosis was found to be 63%, while in females it was 28%
| [3] | Peng S, Plank LD, McCall JL, Gillanders LK, McIlroy K, Gane EJ. Body composition, muscle function, and energy expenditure in patients with liver cirrhosis: A comprehensive study. Am J Clin Nutr. 2007; 85(5): 1257-1266. |
[3]
. In males with cirrhosis, there is a significant decrease in testosterone and insulin-like growth factor-1 levels, leading to a rapid loss of muscle mass and strength. Conversely, women have adequate adipose tissue stores that can be utilized before the onset of sarcopenia
| [4] | Blaak E. Gender differences in fat metabolism. Current Opinion in Clinical Nutrition and Metabolic Care. 2001; 4(6): 499-502. |
[4]
.
The most common aetiology of cirrhosis in both sarcopenia and no sarcopenia groups was alcohol followed by NAFLD. 40.6% of patients in the sarcopenia group and 58.0% of patients in the no sarcopenia group had alcohol related liver disease. 32.1% of patients in the sarcopenia group had NAFLD, compared to 16% of patients in the no sarcopenia group.
Studies have shown that alcoholic and cholestatic liver diseases have severe muscle loss for similar severity of liver disease
| [5] | Periyalwar P, Dasarathy S. Malnutrition in Cirrhosis: Contribution and Consequences of Sarcopenia on Metabolic and Clinical Responses. Clinics in Liver Disease. 2012; 16(1): 95-131. |
[5]
. Muscle loss in ALD can be attributed to ongoing alcohol consumption, ethanol induced sensitisation of skeletal muscle to hyperammonemia and epigenetic changes. Prevalence of sarcopenia in NAFLD ranges from 35-63%
| [6] | Hong HC, Hwang SY, Choi HY, Yoo HJ, Seo JA, Kim SG, et al. Relationship between sarcopenia and nonalcoholic fatty liver disease: The Korean Sarcopenic Obesity Study. Hepatology. 2014; 59(5): 1772-1778. |
[6]
. Issa et al have shown that there is progressive muscle wasting in patients with NASH that precedes the development of cirrhosis and worsens with progression to cirrhosis
| [7] | Issa D, Alkhouri N, Tsien C, Shah S, Lopez R, Mccullough A, et al. Presence of sarcopenia (muscle wasting) in patients with nonalcoholic steatohepatitis. Hepatology. 2014; 60(1): 428-429. |
[7]
. NAFLD and sarcopenia share some common pathophysiological mechanisms like systemic inflammation, insulin resistance, myostatin and adiponectin dysregulation and alterations in the growth hormone/IGF-1 axis. However, a study done by D'Arcangelo et al did not show any association between the prevalence of sarcopenia and the aetiology of cirrhosis
| [8] | D’arcangelo F, Zanetto A, Aliberti C, Shalaby S, Pellone M, Sciarrone SS, et al. The impact of sarcopenia on the outcome of patients with cirrhosis with and without hepatocellular carcinoma who undergo liver transplantation. Hepatoma Res. 2021; 7: 4. |
[8]
.
The six-month cumulative survival in the sarcopenia group was 58.0%, and in the no sarcopenia group was 76.2%, with a log rank p-value of 0.001. This finding is in agreement with many previous studies. Hanai et al. have shown that the 1-, 3-, and 5-year survival rates in patients with sarcopenia and no sarcopenia were 85% and 97%, 63% and 79%, and 53% and 79%, respectively
| [9] | Hanai T, Shiraki M, Nishimura K, Ohnishi S, Imai K, Suetsugu A, et al. Sarcopenia impairs prognosis of patients with liver cirrhosis. Nutrition. 2015; 31(1): 193-199. |
[9]
. Data from Kim et al. show that the 1- and 2-year mortality rates in patients with psoas muscle thickness divided by height (PMTH) ≤ 14 mm/m and PMTH > 14 mm/m was 41.6% and 2.6%, and 66.8% and 15.2%, respectively
| [10] | Kim TY, Kim MY, Sohn JH, Kim SM, Ryu JA, Lim S, et al. Sarcopenia as a useful predictor for long-term mortality in cirrhotic patients with ascites. J Korean Med Sci. 2014; 29(9): 1253-1259. |
[10]
. Montano-Loza et al. found that the 6-month and 1-year survival rates in patients with sarcopenia and no sarcopenia were 71% and 90%, and 53% and 83%, respectively
| [11] | Montano-Loza AJ, Meza-Junco J, Prado CMM, Lieffers JR, Baracos VE, Bain VG, et al. Muscle Wasting Is Associated With Mortality in Patients With Cirrhosis. Clin Gastroenterol Hepatol. 2012; 10(2): 166-173. e1. |
[11]
. The 1-, 2-, and 3-year survival rates in patients with sarcopenia and no sarcopenia were 63% and 79%, 51% and 74%, and 51% and 70%, respectively, in a study conducted by Tandon et al
| [12] | Tandon P, Ney M, Irwin I, Ma MM, Gramlich L, Bain VG, et al. Severe muscle depletion in patients on the liver transplant wait list: Its prevalence and independent prognostic value. Liver Transplant. 2012; 18(10): 1209-1216. |
[12]
. An Indian study has shown that the 1-year mortality rates in patients with sarcopenia and without sarcopenia were 20% and 8.5%, respectively, but this study predominantly included Child A patients
| [13] | Anand A, Mohta S, Agarwal S, Sharma S, Gopi S, Gunjan D, et al. European Working Group on Sarcopenia in Older People (EWGSOP2) Criteria With Population-Based Skeletal Muscle Index Best Predicts Mortality in Asians With Cirrhosis. J Clin Exp Hepatol. 2022; 12(1): 52-60. |
[13]
.
The higher mortality rate in our study population could be explained by several factors. There was a higher number of patients in Child-Pugh classes B and C in the study groups. Our study included a larger proportion of hospitalized patients, who generally have a higher risk of mortality. The study period coincided with the Covid-19 pandemic, which could have contributed to increased mortality rates. It is also worth noting that only a small number of patients underwent LT during the study period, primarily due to financial constraints. These factors collectively help elucidate the higher mortality observed in our study population.
On univariate analysis of other covariates influencing mortality, increasing age, female sex, underweight, higher Child-Pugh score, a MELD-Na score of >15, serum bilirubin >2 mg/dL, serum albumin <2.8 g/dL, INR>1.7 and serum sodium <130 mEq/L were found to be significantly associated with mortality. On multivariate analysis, female sex, sarcopenia, Child-Pugh class C and MELD score >15 emerged as independent predictors of mortality.
Our study shows that sarcopenia is associated with an approximately 1.5 times increased risk of mortality in cirrhosis patients. This finding is consistent with a study conducted by Tandon et al., which identified sarcopenia as an independent predictor of mortality with a hazard ratio of 2.36
| [12] | Tandon P, Ney M, Irwin I, Ma MM, Gramlich L, Bain VG, et al. Severe muscle depletion in patients on the liver transplant wait list: Its prevalence and independent prognostic value. Liver Transplant. 2012; 18(10): 1209-1216. |
[12]
. A Korean study found that sarcopenia was associated with mortality with a hazard ratio of 2.253 in patients with compensated and early decompensated cirrhosis
| [14] | Kang SH, Jeong WK, Baik SK, Cha SH, Kim MY. Impact of sarcopenia on prognostic value of cirrhosis: going beyond the hepatic venous pressure gradient and MELD score. J Cachexia Sarcopenia Muscle. 2018; 9(5): 860-870. |
[14]
. Similarly, in a study by Montano-Loza et al., sarcopenia was identified as an independent predictor of mortality in cirrhosis patients evaluated for LT
| [11] | Montano-Loza AJ, Meza-Junco J, Prado CMM, Lieffers JR, Baracos VE, Bain VG, et al. Muscle Wasting Is Associated With Mortality in Patients With Cirrhosis. Clin Gastroenterol Hepatol. 2012; 10(2): 166-173. e1. |
[11]
.
An important point to note is that sarcopenia had the greatest impact on mortality in patients with a MELD-Na score of <15. In our study, the six-month cumulative survival rate in patients with a MELD-Na score <15 and sarcopenia was 63.6%, which was comparable to the survival rate of 60% in patients with a MELD-Na score >15, regardless of sarcopenia status. This finding is in concordance with a study conducted by Tandon et al
| [12] | Tandon P, Ney M, Irwin I, Ma MM, Gramlich L, Bain VG, et al. Severe muscle depletion in patients on the liver transplant wait list: Its prevalence and independent prognostic value. Liver Transplant. 2012; 18(10): 1209-1216. |
[12]
. A similar observation was also made by Kang et al
| [14] | Kang SH, Jeong WK, Baik SK, Cha SH, Kim MY. Impact of sarcopenia on prognostic value of cirrhosis: going beyond the hepatic venous pressure gradient and MELD score. J Cachexia Sarcopenia Muscle. 2018; 9(5): 860-870. |
[14]
. This highlights the significance of sarcopenia as a useful objective tool for prognosticating cirrhosis patients with low MELD scores. The outcomes in these patients may be improved through standardized nutritional therapy and exercise training. If they are not responding to these measures, MELD exception points can be granted to sarcopenic patients.
In a subgroup analysis using the Child-Pugh class, six-month cumulative survival was found to be higher in patients without sarcopenia than in patients with sarcopenia in Child-Pugh class B. There was no significant difference in survival between patients with or without sarcopenia in Child-Pugh class C, emphasizing the positive impact of early intervention on survival.
Sarcopenia assessment may be used for a more accurate selection of liver transplant patients and organ allocation in the future. However, further studies are needed to validate its utility in this regard. Currently, the selection of patients at risk for early mortality is probably not adequately identified by the MELD score alone. A study by Durand et al. found that 71% of patients who died on the LT waiting list had a MELD score ≤25 at registration
| [15] | Durand F, Buyse S, Francoz C, Laouénan C, Bruno O, Belghiti J, et al. Prognostic value of muscle atrophy in cirrhosis using psoas muscle thickness on computed tomography. J Hepatol. 2014; 60(6): 1151-1157. |
[15]
. In order to improve the prediction of mortality in patients with cirrhosis, especially those with low MELD scores, Montano-Loza et al. have proposed a MELD-sarcopenia score
| [16] | Montano-Loza AJ, Duarte-Rojo A, Meza-Junco J, Baracos VE, Sawyer MB, Pang JXQ, et al. Inclusion of sarcopenia within MELD (MELD-Sarcopenia) and the prediction of mortality in patients with cirrhosis. Clin Transl Gastroenterol. 2015; 6(7): e102. |
[16]
.
None of the previous studies have analysed the role of grading sarcopenia in predicting the prognosis of cirrhosis. In our study, sarcopenia was graded as severe and non-severe based on the EWGSOP2 guidelines. Our findings demonstrate that patients with severe sarcopenia have a poorer outcome, with a cumulative six-month survival of 23.8%, compared to 70.1% in those with non-severe sarcopenia. This highlights the importance of not only detecting sarcopenia but also grading its severity to effectively analyse its prognostic role. Grading of sarcopenia can be accomplished using simple bedside tests such as the 4-meter walk test.
During a follow-up period of 6 months, it was observed that complications such as new onset or worsening ascites, HE, Covid-19 infection, and upper gastrointestinal bleeding were significantly more common in the sarcopenia group compared to the no sarcopenia group. However, there was no statistically significant difference in the occurrence of other complications such as SBP, HRS, HCC, or ACLF. A study by Topan et al has reported increased incidence of ascites, HE, SBP, UTI, UGI bleed and HCC in cirrhosis patients with sarcopenia
| [17] | Topan MM, Sporea I, Dănilă M, Popescu A, Ghiuchici AM, Lupuşoru R, et al. Impact of Sarcopenia on Survival and Clinical Outcomes in Patients With Liver Cirrhosis. Front Nutr. 2021; 8. |
[17]
. As sarcopenia is associated with impaired immunity and deranged physiological functioning, it carries an increased risk of infections in cirrhosis patients. Sepsis is one of the leading causes of death in sarcopenic cirrhosis patients
| [18] | Merli M, Lucidi C, Giannelli V, Giusto M, Riggio O, Falcone M, et al. Cirrhotic patients are at risk for health care-associated bacterial infections. Clin Gastroenterol Hepatol. 2010; 8(11): 979-985. |
[18]
. It has also been shown that pretransplant sarcopenia is associated with adverse post transplant outcomes like prolonged hospital stay, post transplant infections and mortality
| [19] | DiMartini A, Cruz RJ Jr, Dew MA, et al. Muscle mass predicts outcomes following liver transplantation. Liver Transpl. 2013; 19(11): 1172-1180. |
| [20] | Krell RW, Kaul DR, Martin AR, et al. Association between sarcopenia and the risk of serious infection among adults undergoing liver transplantation. Liver Transpl. 2013; 19(12): 1396-1402. |
[19, 20]
.
Traditionally, sarcopenia has been assessed using cross-sectional imaging techniques like CT or MRI, which may not always be easily accessible. Many previous studies lacked a standardized definition of sarcopenia, hindering comparability. The EWGSOP2 guidelines offer a simplified and objective method for diagnosis and grading, but their adoption in prior research has been limited. Assessment of muscle quantity is an important step in diagnosing sarcopenia and tools like CT, MRI, DEXA or BIA can be used in this regard. An innovative approach is ultrasound-guided TMT measurement. Tandon et al. proposed a model incorporating ultrasound-guided TMT and BMI to identify sarcopenia, alongside sex-specific nomograms for diagnosis
| [1] | Tandon P, Low G, Mourtzakis M, Zenith L, Myers RP, Abraldes JG, et al. A Model to Identify Sarcopenia in Patients With Cirrhosis. Clin Gastroenterol Hepatol. 2016; 14(10): 1473-1480. e3. |
[1]
. Thigh ultrasound is a low cost, reliable, reproducible, and accurate measure of muscle quantity that can be performed at the bedside and can be repeated without concern of radiation exposure. This novel method was used in our study to confirm sarcopenia and a probability of more than 80% in sex specific nomograms was used as an arbitrary cutoff. However, further Asian studies are needed for identifying cutoffs and validating this method in our population.
This study highlights the importance of sarcopenia as diagnosed by a standardised definition using a novel method of ultrasound-guided TMT measurement in predicting prognosis in cirrhosis patients. Our study is the first of its kind in an Indian setting.
Our study is not without limitations. The study had a short follow up period of only six months. The study was conducted during Covid 19 pandemic which might have influenced the incidence of mortality and complications in some patients. Because of financial constraints, most of our patients did not undergo LT which might have influenced the outcome and survival. We used cutoff scores that were validated in a different population for the diagnosis of sarcopenia.
5. Conclusion
Sarcopenia is an independent prognostic marker of mortality in cirrhosis patients. Severe sarcopenia has an even poorer outcome when compared to non severe sarcopenia. Female patients with sarcopenia has a lower cumulative survival when compared to males with sarcopenia. Sarcopenia had the greatest impact on mortality in patients with MELD-Na score <15. Sarcopenia is associated with an increased risk of complications like new onset or worsening ascites, hepatic encephalopathy, Covid 19 infection and Upper GI bleed. Ultrasound-guided TMT measurement is an easy and reliable measure of diagnosing sarcopenia and can be used in cirrhosis patients for predicting mortality. Adding sarcopenia to existing cirrhosis scoring systems may improve prognostication.
Abbreviations
ACLF | Acute on Chronic Liver Failure |
ALD | Alcohol Related Liver Disease |
BMI | Body Mass Index |
BIA | Bioelectrical Impedance Analysis |
CTP | Child-Turcotte-Pugh |
DEXA | Dual Energy X-ray Absorptiometry |
EWGSOP2 | European Working Group on Sarcopenia in Older People |
HCC | Hepatocellular Carcinoma |
HE | Hepatic Encephalopathy |
HRS | Hepatorenal Syndrome |
LRTI | Lower Respiratory Tract Infection |
LT | Liver Transplantation |
MELD | Model for end Stage Liver Disease |
MRI | Magnetic Resonance Imaging |
NAFLD | Non Alcoholic Fatty Liver Disease |
NASH | Non Alcoholic Steatohepatitis |
SBP | Spontaneous Bacterial Peritonitis |
TMT | Thigh Muscle Thickness |
UTI | Urinary Tract Infection |
Acknowledgments
Not applicable.
Ethics Approval and Consent to Participate
All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2008 (5). Informed consent was obtained from all patients for being included in the study.
Consent for Publication
Not applicable.
Availability of Data and Material
The datasets used and analysed during the current study are available from corresponding author on reasonable request.
Author Contributions
Nidhin Devadas: Conceptualization, Data curation, Formal Analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Software, Validation, Visualization, Writing – original draft, Writing – review & editing
Kadavanoor Srijith: Supervision, Validation
Sunil Kumar Kandiyil: Investigation, Supervision, Validation
Sithara Balagopal: Supervision
Sandesh Kolassery: Supervision
Funding
Authors declare that no funds, grants, or other support were received during the preparation of this manuscript.
Conflicts of Interests
The authors declare no conflicts of interest.
References
| [1] |
Tandon P, Low G, Mourtzakis M, Zenith L, Myers RP, Abraldes JG, et al. A Model to Identify Sarcopenia in Patients With Cirrhosis. Clin Gastroenterol Hepatol. 2016; 14(10): 1473-1480. e3.
|
| [2] |
Cruz-Jentoft AJ, Bahat G, Bauer J, Boirie Y, Bruyère O, Cederholm T, et al. Sarcopenia: Revised European consensus on definition and diagnosis. Age and Ageing. 2019; 48(1): 16-31.
|
| [3] |
Peng S, Plank LD, McCall JL, Gillanders LK, McIlroy K, Gane EJ. Body composition, muscle function, and energy expenditure in patients with liver cirrhosis: A comprehensive study. Am J Clin Nutr. 2007; 85(5): 1257-1266.
|
| [4] |
Blaak E. Gender differences in fat metabolism. Current Opinion in Clinical Nutrition and Metabolic Care. 2001; 4(6): 499-502.
|
| [5] |
Periyalwar P, Dasarathy S. Malnutrition in Cirrhosis: Contribution and Consequences of Sarcopenia on Metabolic and Clinical Responses. Clinics in Liver Disease. 2012; 16(1): 95-131.
|
| [6] |
Hong HC, Hwang SY, Choi HY, Yoo HJ, Seo JA, Kim SG, et al. Relationship between sarcopenia and nonalcoholic fatty liver disease: The Korean Sarcopenic Obesity Study. Hepatology. 2014; 59(5): 1772-1778.
|
| [7] |
Issa D, Alkhouri N, Tsien C, Shah S, Lopez R, Mccullough A, et al. Presence of sarcopenia (muscle wasting) in patients with nonalcoholic steatohepatitis. Hepatology. 2014; 60(1): 428-429.
|
| [8] |
D’arcangelo F, Zanetto A, Aliberti C, Shalaby S, Pellone M, Sciarrone SS, et al. The impact of sarcopenia on the outcome of patients with cirrhosis with and without hepatocellular carcinoma who undergo liver transplantation. Hepatoma Res. 2021; 7: 4.
|
| [9] |
Hanai T, Shiraki M, Nishimura K, Ohnishi S, Imai K, Suetsugu A, et al. Sarcopenia impairs prognosis of patients with liver cirrhosis. Nutrition. 2015; 31(1): 193-199.
|
| [10] |
Kim TY, Kim MY, Sohn JH, Kim SM, Ryu JA, Lim S, et al. Sarcopenia as a useful predictor for long-term mortality in cirrhotic patients with ascites. J Korean Med Sci. 2014; 29(9): 1253-1259.
|
| [11] |
Montano-Loza AJ, Meza-Junco J, Prado CMM, Lieffers JR, Baracos VE, Bain VG, et al. Muscle Wasting Is Associated With Mortality in Patients With Cirrhosis. Clin Gastroenterol Hepatol. 2012; 10(2): 166-173. e1.
|
| [12] |
Tandon P, Ney M, Irwin I, Ma MM, Gramlich L, Bain VG, et al. Severe muscle depletion in patients on the liver transplant wait list: Its prevalence and independent prognostic value. Liver Transplant. 2012; 18(10): 1209-1216.
|
| [13] |
Anand A, Mohta S, Agarwal S, Sharma S, Gopi S, Gunjan D, et al. European Working Group on Sarcopenia in Older People (EWGSOP2) Criteria With Population-Based Skeletal Muscle Index Best Predicts Mortality in Asians With Cirrhosis. J Clin Exp Hepatol. 2022; 12(1): 52-60.
|
| [14] |
Kang SH, Jeong WK, Baik SK, Cha SH, Kim MY. Impact of sarcopenia on prognostic value of cirrhosis: going beyond the hepatic venous pressure gradient and MELD score. J Cachexia Sarcopenia Muscle. 2018; 9(5): 860-870.
|
| [15] |
Durand F, Buyse S, Francoz C, Laouénan C, Bruno O, Belghiti J, et al. Prognostic value of muscle atrophy in cirrhosis using psoas muscle thickness on computed tomography. J Hepatol. 2014; 60(6): 1151-1157.
|
| [16] |
Montano-Loza AJ, Duarte-Rojo A, Meza-Junco J, Baracos VE, Sawyer MB, Pang JXQ, et al. Inclusion of sarcopenia within MELD (MELD-Sarcopenia) and the prediction of mortality in patients with cirrhosis. Clin Transl Gastroenterol. 2015; 6(7): e102.
|
| [17] |
Topan MM, Sporea I, Dănilă M, Popescu A, Ghiuchici AM, Lupuşoru R, et al. Impact of Sarcopenia on Survival and Clinical Outcomes in Patients With Liver Cirrhosis. Front Nutr. 2021; 8.
|
| [18] |
Merli M, Lucidi C, Giannelli V, Giusto M, Riggio O, Falcone M, et al. Cirrhotic patients are at risk for health care-associated bacterial infections. Clin Gastroenterol Hepatol. 2010; 8(11): 979-985.
|
| [19] |
DiMartini A, Cruz RJ Jr, Dew MA, et al. Muscle mass predicts outcomes following liver transplantation. Liver Transpl. 2013; 19(11): 1172-1180.
|
| [20] |
Krell RW, Kaul DR, Martin AR, et al. Association between sarcopenia and the risk of serious infection among adults undergoing liver transplantation. Liver Transpl. 2013; 19(12): 1396-1402.
|
Cite This Article
-
APA Style
Devadas, N., Srijith, K., Kandiyil, S. K., Balagopal, S., Kolassery, S. (2024). Sarcopenia as a Predictor of Mortality and Complications in Cirrhosis Patients-A Prospective Cohort Study. International Journal of Gastroenterology, 8(2), 85-95. https://doi.org/10.11648/j.ijg.20240802.15
 Copy
|
Copy
|
 Download
Download
ACS Style
Devadas, N.; Srijith, K.; Kandiyil, S. K.; Balagopal, S.; Kolassery, S. Sarcopenia as a Predictor of Mortality and Complications in Cirrhosis Patients-A Prospective Cohort Study. Int. J. Gastroenterol. 2024, 8(2), 85-95. doi: 10.11648/j.ijg.20240802.15
Copy
|
Download
AMA Style
Devadas N, Srijith K, Kandiyil SK, Balagopal S, Kolassery S. Sarcopenia as a Predictor of Mortality and Complications in Cirrhosis Patients-A Prospective Cohort Study. Int J Gastroenterol. 2024;8(2):85-95. doi: 10.11648/j.ijg.20240802.15
Copy
|
Download
-
@article{10.11648/j.ijg.20240802.15,
author = {Nidhin Devadas and Kadavanoor Srijith and Sunil Kumar Kandiyil and Sithara Balagopal and Sandesh Kolassery},
title = {Sarcopenia as a Predictor of Mortality and Complications in Cirrhosis Patients-A Prospective Cohort Study},
journal = {International Journal of Gastroenterology},
volume = {8},
number = {2},
pages = {85-95},
doi = {10.11648/j.ijg.20240802.15},
url = {https://doi.org/10.11648/j.ijg.20240802.15},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ijg.20240802.15},
abstract = {Background: Sarcopenia has emerged as an important prognostic factor in cirrhosis patients. A standardized definition of sarcopenia was not used in many of the studies. EWGSOP2 2019 guidelines define sarcopenia in an objective manner. Ultrasound-guided measurement of thigh muscle thickness is a validated and cost effective tool for the assessment of muscle quantity. Aim of the study was to evaluate the predictive role of sarcopenia on mortality and complications in cirrhosis patients. Methods: It was a prospective cohort study with 143 consecutive patients each in sarcopenia and no sarcopenia groups. Sarcopenia was diagnosed as per EWGSOP2 guidelines incorporating ultrasound-guided thigh muscle thickness measurement. They were studied at 6 months for development of complications and mortality. Kaplan-Meier analysis was used to compare survival and Cox proportional hazards model was used to determine risk factors of mortality. Results: Cirrhosis patients with sarcopenia [M:F=97:46] and without sarcopenia [M:F=111:32] were followed up for 6 months. Survival analysis showed a six-month cumulative survival of 58.0% (95%CI 57.92-58.08) and 76.2% (95% CI 76.13-76.27) in sarcopenia and no sarcopenia groups respectively (p-value 0.001). Six-month cumulative survival in patients with severe sarcopenia was 23.8% and in non-severe sarcopenia was 70.1% (p-value 0.001). Multivariate analysis showed sarcopenia (HR=1.498,95%CI 1.081-2.148), female sex (HR=1.86,95%CI 1.102-3.089), Child Pugh class C (HR=1.458,95%CI 1.214-1.775) and MELD-Na score>15 (HR=1.122,95%CI 1.068-2.212) as independent predictors of mortality. Complications like ascites, HE, Covid 19 infection and UGI bleed were significantly higher in the sarcopenia group. Conclusion: Sarcopenia is an independent prognostic marker of mortality in cirrhosis patients and is associated with an increased risk of complications. Severe sarcopenia has even poorer outcome.},
year = {2024}
}
Copy
|
Download
-
TY - JOUR
T1 - Sarcopenia as a Predictor of Mortality and Complications in Cirrhosis Patients-A Prospective Cohort Study
AU - Nidhin Devadas
AU - Kadavanoor Srijith
AU - Sunil Kumar Kandiyil
AU - Sithara Balagopal
AU - Sandesh Kolassery
Y1 - 2024/12/30
PY - 2024
N1 - https://doi.org/10.11648/j.ijg.20240802.15
DO - 10.11648/j.ijg.20240802.15
T2 - International Journal of Gastroenterology
JF - International Journal of Gastroenterology
JO - International Journal of Gastroenterology
SP - 85
EP - 95
PB - Science Publishing Group
SN - 2640-169X
UR - https://doi.org/10.11648/j.ijg.20240802.15
AB - Background: Sarcopenia has emerged as an important prognostic factor in cirrhosis patients. A standardized definition of sarcopenia was not used in many of the studies. EWGSOP2 2019 guidelines define sarcopenia in an objective manner. Ultrasound-guided measurement of thigh muscle thickness is a validated and cost effective tool for the assessment of muscle quantity. Aim of the study was to evaluate the predictive role of sarcopenia on mortality and complications in cirrhosis patients. Methods: It was a prospective cohort study with 143 consecutive patients each in sarcopenia and no sarcopenia groups. Sarcopenia was diagnosed as per EWGSOP2 guidelines incorporating ultrasound-guided thigh muscle thickness measurement. They were studied at 6 months for development of complications and mortality. Kaplan-Meier analysis was used to compare survival and Cox proportional hazards model was used to determine risk factors of mortality. Results: Cirrhosis patients with sarcopenia [M:F=97:46] and without sarcopenia [M:F=111:32] were followed up for 6 months. Survival analysis showed a six-month cumulative survival of 58.0% (95%CI 57.92-58.08) and 76.2% (95% CI 76.13-76.27) in sarcopenia and no sarcopenia groups respectively (p-value 0.001). Six-month cumulative survival in patients with severe sarcopenia was 23.8% and in non-severe sarcopenia was 70.1% (p-value 0.001). Multivariate analysis showed sarcopenia (HR=1.498,95%CI 1.081-2.148), female sex (HR=1.86,95%CI 1.102-3.089), Child Pugh class C (HR=1.458,95%CI 1.214-1.775) and MELD-Na score>15 (HR=1.122,95%CI 1.068-2.212) as independent predictors of mortality. Complications like ascites, HE, Covid 19 infection and UGI bleed were significantly higher in the sarcopenia group. Conclusion: Sarcopenia is an independent prognostic marker of mortality in cirrhosis patients and is associated with an increased risk of complications. Severe sarcopenia has even poorer outcome.
VL - 8
IS - 2
ER -
Copy
|
Download