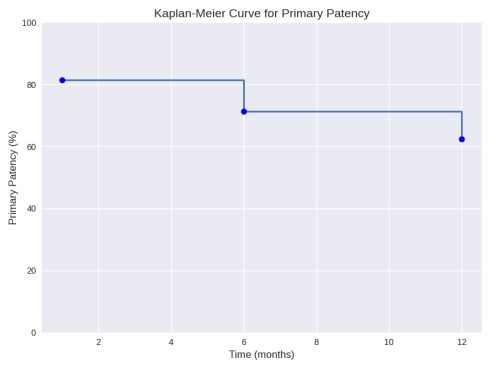
Background: Critical limb ischemia (CLI) represents the most advanced stage of peripheral arterial disease (PAD) and remains associated with substantial morbidity and mortality. Data from Sub-Saharan Africa are scarce despite a rapidly increasing burden of disease. Objective: To evaluate the epidemiological characteristics, therapeutic strategies, and outcomes of patients treated for CLI in a tertiary cardiovascular surgery center. Methods: A retrospective study was conducted from January 2020 to December 2023, including 65 patients managed for CLI. Epidemiological, clinical, imaging, therapeutic, and outcome variables were analyzed. Results: Mean age was 65.3 years; 54% were male. Hypertension (58%), smoking (38%), and diabetes (34%) were the most common risk factors. Trophic lesions were present in 80% of cases. Endovascular therapy was performed in 70.7% of patients, bypass surgery in 15.4%, and thrombo-endarterectomy in 13.8%. Perioperative complications occurred in 37%. Mortality reached 14%. A total of 56 amputations were performed (25 minor, 31 major). Diabetes was significantly associated with minor amputation, while diabetes, hypertension, and smoking predicted major amputation. Primary patency was 61.5% at 1 month and 52.3% at 1 year. Conclusion: CLI remains a severe condition with high rates of complications, amputation, and mortality. Endovascular therapy was the predominant strategy with acceptable early patency. Earlier diagnosis and improved cardiovascular risk management are essential to improve outcomes in Sub-Saharan Africa.
| Published in | International Journal of Cardiovascular and Thoracic Surgery (Volume 12, Issue 3) |
| DOI | 10.11648/j.ijcts.20261203.11 |
| Page(s) | 85-91 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2026. Published by Science Publishing Group |
Critical Limb Ischemia, Peripheral Arterial Disease, Endovascular Therapy, Bypass Surgery, Limb Salvage, Amputation Predictors, Sub-Saharan Africa
Variable | Value |
|---|---|
Mean age (years) | 65.3 ± 15.8 |
Male sex | 35 (54%) |
Hypertension | 38 (58%) |
Smoking | 25 (38%) |
Diabetes | 22 (34%) |
Clinical feature | n (%) |
|---|---|
Trophic lesions | 52 (80%) |
Ulcers | 29 (45%) |
Gangrene | 23 (35%) |
Absent popliteal pulse | 47 (73%) |
Absent distal pulses | 65 (100%) |
Procedure type | n (%) | Details |
|---|---|---|
Endovascular therapy | 46 (70.7%) | Balloon angioplasty (45), stent (1) |
Bypass surgery | 10 (15.4%) | Prosthetic grafts (80%), anatomical bypass (60%) |
Thromboendarterectomy | 9 (13.8%) | - |
Complication type | n (%) |
|---|---|
Metabolic | 10 (15%) |
Infectious | 9 (14%) |
Cerebral | 2 (3%) |
Cardiac | 2 (3%) |
Outcome | Value |
--- | --- |
Total mortality | 9 (14%) |
Minor amputations | 25 |
Major amputations | 31 |
Risk factor | Amputation type | No | Yes | Total | P value |
|---|---|---|---|---|---|
Hypertension (HTN) | Minor | 28 (73.6%) | 10 (23.4%) | 38 | 0.087 |
Major | 35 (92%) | 3 (8%) | 38 | 0.001 | |
Diabetes | Minor | 10 (45%) | 12 (55%) | 22 | 0.002 |
Major | 18 (81.8%) | 4 (18.2%) | 22 | 0.026 | |
Smoking | Minor | 22 (88%) | 3 (12%) | 25 | 0.774 |
Major | 18 (72%) | 7 (28%) | 25 | 0.025 |
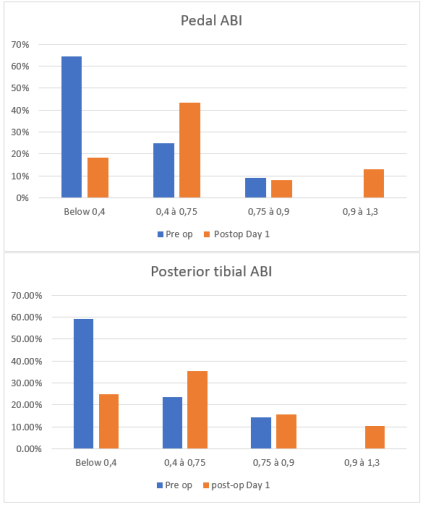
ABI | Ankle–Brachial Index |
CLI | Critical Limb Ischemia |
CT | Computed Tomography |
ESC | European Society of Cardiology |
ESVS | European Society for Vascular Surgery |
GVG | Global Vascular Guidelines |
HTN | Hypertension |
LV | Left Ventricular |
PAD | Peripheral Arterial Disease |
SPSS | Statistical Package for the Social Sciences |
WIfI | Wound, Ischemia, and Foot Infection Classification |
| [1] | Criqui MH, Matsushita K. Epidemiology of peripheral artery disease. Circ Res. 2021; 128(12): 1818-36. |
| [2] | Farber A, Eberhardt RT. The current state of critical limb ischemia. Circulation. 2022; 145(9): 687-705. |
| [3] | Conte MS, Bradbury AW, Kolh P, et al. Global vascular guidelines on the management of chronic limb-threatening ischemia. J Vasc Surg. 2019; 69(6S): 3S-125S. |
| [4] | GBD 2021 Peripheral Artery Disease Collaborators. Global burden of peripheral artery disease. Lancet. 2022; 400(10349): 123-40. |
| [5] | Ogu US, et al. Outcomes of critical limb ischemia in Sub-Saharan Africa. Vascular. 2020; 28(4): 345-52. |
| [6] | Ba PS, et al. Critical limb ischemia in Senegal: epidemiology and outcomes. Pan Afr Med J. 2021; 38: 112. |
| [7] | BEST-CLI Investigators. Surgical vs endovascular therapy for CLI. N Engl J Med. 2022; 387: 2305-16. |
| [8] | BASIL-2 Trial Investigators. Bypass vs endovascular therapy for infrapopliteal disease. Lancet. 2023; 402(10397): 145-56. |
| [9] | Aboyans V, et al. 2023 ESC Guidelines on peripheral artery disease. Eur Heart J. 2023; 44(1): 1-92. |
| [10] | ESVS Guidelines 2023. Management of PAD. Eur J Vasc Endovasc Surg. 2023; 65(1): 1-120. |
| [11] | Farber A. Mortality in chronic limb-threatening ischemia. J Vasc Surg. 2022; 75(4): 1234-45. |
| [12] | Hultgren R, et al. Sex differences in chronic limb-threatening ischemia. Eur J Vasc Endovasc Surg. 2020; 59(6): 789-97. |
| [13] | Armstrong DG, et al. Predictors of amputation in diabetic CLI. Diabetes Care. 2020; 43(1): 123-31. |
| [14] | Mustapha JA, et al. Outcomes of tibial interventions. J Endovasc Ther. 2021; 28(2): 123-34. |
| [15] | Kawarada O, et al. Tibial artery disease in diabetics. JACC Cardiovasc Interv. 2020; 13(20): 2341-52. |
| [16] | Hinchliffe RJ, et al. Diabetic foot and limb-threatening ischemia. Lancet Diabetes Endocrinol. 2021; 9(6): 327-39. |
| [17] | Mills JL, et al. WIfI classification update. J Vasc Surg. 2020; 72(1): 3-17. |
| [18] | Laird JR, et al. Endovascular therapy for CLI: contemporary outcomes. Circulation. 2020; 142(17): 1605-18. |
| [19] | VOYAGER PAD Trial Investigators. Rivaroxaban after lower-extremity revascularization. N Engl J Med. 2020; 382: 1994-2004. |
| [20] | Farber A, et al. Limb salvage strategies in CLI. J Vasc Surg. 2023; 77(2): 456-68. |
| [21] | Patel MR, et al. PAD as a systemic cardiovascular disease. Circulation. 2021; 144(8): 632-50. |
| [22] | Norgren L, et al. Advances in PAD management. Eur J Vasc Endovasc Surg. 2020; 59(6): 873-84. |
| [23] | Katsanos K, et al. Drug-coated balloons in PAD. JACC Cardiovasc Interv. 2020; 13(15): 1963-75. |
| [24] | Zeller T, et al. Drug-eluting stents for infrapopliteal disease. Circulation. 2021; 143(6): 604-15. |
| [25] | Bradbury AW, et al. Long-term outcomes in CLI. J Vasc Surg. 2020; 72(6): 2132-41. |
APA Style
Thiaw, A. A., Sow, N. F., Mbengue, A. L., Ba, D. I., Camara, M., et al. (2026). Revascularization Strategies and Outcomes in Critical Limb Ischemia: A Four-year Retrospective Study of 65 Patients in a Sub-Saharan Cardiovascular Surgery Center. International Journal of Cardiovascular and Thoracic Surgery, 12(3), 85-91. https://doi.org/10.11648/j.ijcts.20261203.11
ACS Style
Thiaw, A. A.; Sow, N. F.; Mbengue, A. L.; Ba, D. I.; Camara, M., et al. Revascularization Strategies and Outcomes in Critical Limb Ischemia: A Four-year Retrospective Study of 65 Patients in a Sub-Saharan Cardiovascular Surgery Center. Int. J. Cardiovasc. Thorac. Surg. 2026, 12(3), 85-91. doi: 10.11648/j.ijcts.20261203.11
AMA Style
Thiaw AA, Sow NF, Mbengue AL, Ba DI, Camara M, et al. Revascularization Strategies and Outcomes in Critical Limb Ischemia: A Four-year Retrospective Study of 65 Patients in a Sub-Saharan Cardiovascular Surgery Center. Int J Cardiovasc Thorac Surg. 2026;12(3):85-91. doi: 10.11648/j.ijcts.20261203.11
@article{10.11648/j.ijcts.20261203.11,
author = {Abdoul Aziz Thiaw and Ndeye Fatou Sow and Abdou Lahat Mbengue and Dialtabe Ibrahima Ba and Mory Camara and Moussa Mareme Samba and Abdou Khoudouss Diallo and Mareme Samba and Anta Mbaye Sall and Cheikh Abdou Khadre Faye and Amadou Dioulde Diallo and Mareme Soda Mbaye and Moussa Seck Diop and Pape Ousmane Ba and Papa Amath Diagne and Momar Sokhna Diop and Magaye Gaye and Souleymane Diatta and Papa Salmane Ba and Papa Adama Dieng and Amadou Gabriel Ciss},
title = {Revascularization Strategies and Outcomes in Critical Limb Ischemia: A Four-year Retrospective Study of 65 Patients in a Sub-Saharan Cardiovascular Surgery Center},
journal = {International Journal of Cardiovascular and Thoracic Surgery},
volume = {12},
number = {3},
pages = {85-91},
doi = {10.11648/j.ijcts.20261203.11},
url = {https://doi.org/10.11648/j.ijcts.20261203.11},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ijcts.20261203.11},
abstract = {Background: Critical limb ischemia (CLI) represents the most advanced stage of peripheral arterial disease (PAD) and remains associated with substantial morbidity and mortality. Data from Sub-Saharan Africa are scarce despite a rapidly increasing burden of disease. Objective: To evaluate the epidemiological characteristics, therapeutic strategies, and outcomes of patients treated for CLI in a tertiary cardiovascular surgery center. Methods: A retrospective study was conducted from January 2020 to December 2023, including 65 patients managed for CLI. Epidemiological, clinical, imaging, therapeutic, and outcome variables were analyzed. Results: Mean age was 65.3 years; 54% were male. Hypertension (58%), smoking (38%), and diabetes (34%) were the most common risk factors. Trophic lesions were present in 80% of cases. Endovascular therapy was performed in 70.7% of patients, bypass surgery in 15.4%, and thrombo-endarterectomy in 13.8%. Perioperative complications occurred in 37%. Mortality reached 14%. A total of 56 amputations were performed (25 minor, 31 major). Diabetes was significantly associated with minor amputation, while diabetes, hypertension, and smoking predicted major amputation. Primary patency was 61.5% at 1 month and 52.3% at 1 year. Conclusion: CLI remains a severe condition with high rates of complications, amputation, and mortality. Endovascular therapy was the predominant strategy with acceptable early patency. Earlier diagnosis and improved cardiovascular risk management are essential to improve outcomes in Sub-Saharan Africa.},
year = {2026}
}
TY - JOUR T1 - Revascularization Strategies and Outcomes in Critical Limb Ischemia: A Four-year Retrospective Study of 65 Patients in a Sub-Saharan Cardiovascular Surgery Center AU - Abdoul Aziz Thiaw AU - Ndeye Fatou Sow AU - Abdou Lahat Mbengue AU - Dialtabe Ibrahima Ba AU - Mory Camara AU - Moussa Mareme Samba AU - Abdou Khoudouss Diallo AU - Mareme Samba AU - Anta Mbaye Sall AU - Cheikh Abdou Khadre Faye AU - Amadou Dioulde Diallo AU - Mareme Soda Mbaye AU - Moussa Seck Diop AU - Pape Ousmane Ba AU - Papa Amath Diagne AU - Momar Sokhna Diop AU - Magaye Gaye AU - Souleymane Diatta AU - Papa Salmane Ba AU - Papa Adama Dieng AU - Amadou Gabriel Ciss Y1 - 2026/04/28 PY - 2026 N1 - https://doi.org/10.11648/j.ijcts.20261203.11 DO - 10.11648/j.ijcts.20261203.11 T2 - International Journal of Cardiovascular and Thoracic Surgery JF - International Journal of Cardiovascular and Thoracic Surgery JO - International Journal of Cardiovascular and Thoracic Surgery SP - 85 EP - 91 PB - Science Publishing Group SN - 2575-4882 UR - https://doi.org/10.11648/j.ijcts.20261203.11 AB - Background: Critical limb ischemia (CLI) represents the most advanced stage of peripheral arterial disease (PAD) and remains associated with substantial morbidity and mortality. Data from Sub-Saharan Africa are scarce despite a rapidly increasing burden of disease. Objective: To evaluate the epidemiological characteristics, therapeutic strategies, and outcomes of patients treated for CLI in a tertiary cardiovascular surgery center. Methods: A retrospective study was conducted from January 2020 to December 2023, including 65 patients managed for CLI. Epidemiological, clinical, imaging, therapeutic, and outcome variables were analyzed. Results: Mean age was 65.3 years; 54% were male. Hypertension (58%), smoking (38%), and diabetes (34%) were the most common risk factors. Trophic lesions were present in 80% of cases. Endovascular therapy was performed in 70.7% of patients, bypass surgery in 15.4%, and thrombo-endarterectomy in 13.8%. Perioperative complications occurred in 37%. Mortality reached 14%. A total of 56 amputations were performed (25 minor, 31 major). Diabetes was significantly associated with minor amputation, while diabetes, hypertension, and smoking predicted major amputation. Primary patency was 61.5% at 1 month and 52.3% at 1 year. Conclusion: CLI remains a severe condition with high rates of complications, amputation, and mortality. Endovascular therapy was the predominant strategy with acceptable early patency. Earlier diagnosis and improved cardiovascular risk management are essential to improve outcomes in Sub-Saharan Africa. VL - 12 IS - 3 ER -
Thoracic and Cardiovascular Surgery Department, National University Hospital Center of Fann, Dakar, Senegal
Thoracic and Cardiovascular Surgery Department, National University Hospital Center of Fann, Dakar, Senegal
Thoracic and Cardiovascular Surgery Department, National University Hospital Center of Fann, Dakar, Senegal
Thoracic and Cardiovascular Surgery Department, National University Hospital Center of Fann, Dakar, Senegal
Information