Background: Solitary fibrous tumors (SFTs) are rare mesenchymal neoplasms initially described as pleural tumors but now recognized as ubiquitous lesions with variable biological behavior, and intrapericardial SFTs represent an exceptional subset with fewer than a dozen well-documented cases in the literature, their clinical presentation often being nonspecific while life-threatening complications such as cardiac tamponade remain exceedingly rare. Case presentation: A 72-year-old man presented with progressive dyspnea, dry cough, and retrosternal chest pain evolving over three months, culminating in cardiorespiratory distress; clinical examination revealed cardiac tamponade. Echocardiography demonstrated a regular iso-echogenic intrapericardial mass compressing the left cardiac chambers, measuring 12.6 × 9.6 cm, and thoracic CT scan showed a large, well-defined hypodense mass in the anterior mediastinum adjacent to the left cardiac border. A monobloc surgical excision was performed via median sternotomy, and tumor removal resulted in abrupt re-expansion of the cardiac chambers with sudden hypotension requiring fluid resuscitation and vasopressor support. Postoperative evolution was marked by cardiogenic shock on day 1, managed with dobutamine and norepinephrine, followed by progressive improvement allowing discharge on postoperative day 10. Histopathological analysis confirmed an intrapericardial solitary fibrous tumor. Conclusion: Intrapericardial SFTs are extremely rare, complete surgical resection remains the treatment of choice, and long?term imaging follow-up is essential due to the potential for recurrence or malignant transformation.
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited.
Solitary Fibrous Tumor, Pericardium, Cardiac Tamponade, Mediastinal Tumor, Surgery
1. Introduction
Solitary fibrous tumors (SFTs) are rare mesenchymal neoplasms first described by Klemperer and Rabin in 1931 as “localized mesotheliomas” originating from the pleura
[1]
Kallen ME, Hornick JL. The 2020 WHO classification: what’s new in soft tissue tumor pathology? Am J Surg Pathol. 2021; 45: e1–e23.
[2]
Czimbalmos C, Csecs I, Polos M, et al. Uncommon presentation of a rare tumour—incidental finding in an asymptomatic patient: case report and comprehensive review of the literature on intrapericardial solitary fibrous tumours. BMC Cancer. 2017; 17: 612.
[1, 2]
. Initially considered exclusively pleural, these tumors were later recognized as ubiquitous lesions capable of arising in virtually any anatomical site, leading to their reclassification in modern WHO (World Health Organization) classifications
[1]
Kallen ME, Hornick JL. The 2020 WHO classification: what’s new in soft tissue tumor pathology? Am J Surg Pathol. 2021; 45: e1–e23.
[1]
. Histologically, SFTs are characterized by spindle‑cell proliferation within a collagenous stroma and a distinctive “patternless pattern.” The discovery of the NAB2‑STAT6 gene fusion has since become a defining molecular hallmark of SFTs, supporting their unified pathogenesis
[3]
Geramizadeh B, Marzban M, Churg A. Role of immunohistochemistry in the diagnosis of solitary fibrous tumor: a review. Iran J Pathol. 2016; 11(3): 195‑203.
[3]
.
Although the pleura remains the most common site, extrapleural SFTs have been reported in the mediastinum, peritoneum, meninges, orbit, and soft tissues
[2]
Czimbalmos C, Csecs I, Polos M, et al. Uncommon presentation of a rare tumour—incidental finding in an asymptomatic patient: case report and comprehensive review of the literature on intrapericardial solitary fibrous tumours. BMC Cancer. 2017; 17: 612.
[4]
Szot M, Zub A, Kurzawa P, et al. Cardiac solitary fibrous tumor—an extremely rare but potentially fatal diagnosis. Kardiochir Torakochirurgia Pol. 2024; 21: 39–42.
[2, 4]
. Cardiac and pericardial localizations are exceptionally rare. The first well‑documented intrapericardial SFTs were reported in the late 1980s and early 1990s, notably by El‑Naggar et al.
[5]
El‑Naggar AK, Ro JY, Ayala AG, et al. Localized fibrous tumor of the serosal cavities: immunohistochemical, electron‑microscopic, and flow‑cytometric DNA study. Am J Clin Pathol. 1989; 92(5): 561‑5.
[5]
and Bortolotti et al.
[6]
Bortolotti U, Calabrò F, Loy M, et al. Giant intrapericardial solitary fibrous tumor. Ann Thorac Surg. 1992; 54(6): 1219‑20.
[6]
, who described large benign tumors compressing cardiac structures.
Clinically, intrapericardial SFTs may remain asymptomatic for long periods or present with nonspecific symptoms such as dyspnea, chest pain, or signs of right‑sided compression. Life‑threatening complications, including cardiac tamponade, are extremely uncommon but have been reported in a handful of cases
[2]
Czimbalmos C, Csecs I, Polos M, et al. Uncommon presentation of a rare tumour—incidental finding in an asymptomatic patient: case report and comprehensive review of the literature on intrapericardial solitary fibrous tumours. BMC Cancer. 2017; 17: 612.
[7]
Shao D, Wang SX. Pericardial solitary fibrous tumor on FDG PET/CT. Clin Nucl Med. 2019; 44(1): 85‑7.
[8]
Zhang LP, Zhang L, Wang G, et al. Pericardial malignant solitary fibrous tumour with right atrial invasion. J Int Med Res. 2019; 47(6): 2716‑22.
[2, 7, 8]
. Imaging modalities such as echocardiography, CT, and MRI play a central role in detection and characterization, but definitive diagnosis relies on histopathology and immunohistochemistry, particularly STAT6 nuclear positivity
[3]
Geramizadeh B, Marzban M, Churg A. Role of immunohistochemistry in the diagnosis of solitary fibrous tumor: a review. Iran J Pathol. 2016; 11(3): 195‑203.
[3]
.
Given the scarcity of reported cases and the potential for malignant transformation or recurrence even after complete resection intrapericardial SFTs warrant careful documentation. We report a case of a large intrapericardial SFT revealed by cardiac tamponade in a 72‑year‑old patient.
2. Case Presentation
A 72‑year‑old man, chronic smoker of traditional tobacco and without significant medical history, presented with exertional dyspnea (NYHA class III), dry cough, and retrosternal chest pain evolving over three months. Symptoms occurred in a context of general deterioration, unquantified weight loss, and physical asthenia. The onset of cardiorespiratory distress prompted urgent consultation.
On admission, the patient was hemodynamically unstable: blood pressure 80/54 mmHg, heart rate 102 bpm, oxygen saturation 94%. Heart sounds were muffled and irregular. Breath sounds were decreased bilaterally, while thoracic expansion remained normal. The remainder of the examination was unremarkable. Given the clinical suspicion of cardiac tamponade, the patient was transferred to the intensive care unit for stabilization and urgent evaluation.
Electrocardiogram showed an irregular sinus rhythm (92 bpm), attenuation of R waves in V1–V3, polymorphic ventricular extrasystoles, and low peripheral voltage.
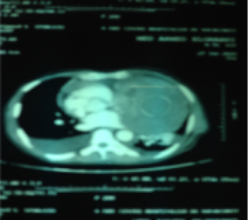
Transthoracic echocardiography revealed a regular iso‑echogenic intrapericardial mass compressing the left cardiac chambers, measuring 12.6 × 9.6 cm (LVEF 54%, TAPSE 16 mm, PASP 28 mmHg). Thoracic CT scan demonstrated a large, well‑defined hypodense mass in the anterior mediastinum adjacent to the left cardiac border. Laboratory tests, including AFP, were normal.
Figure 1. Thoracic CT angiography showing a mediastinal mass compressing the left cardiac chambers.
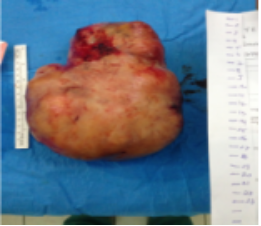
Surgical Management: Median sternotomy revealed a pearly‑white, solid, hemorrhagic intrapericardial mass displacing the heart and compressing the left chambers. A monobloc excision was performed. Tumor removal caused sudden re‑expansion of the cardiac chambers and abrupt hypotension, requiring aggressive fluid resuscitation and vasopressor support. Accidental opening of both pleural cavities required placement of four drains (two pleural, one pericardial, one retrosternal).
Postoperative echocardiography showed severe left ventricular dysfunction. On postoperative day 1, the patient developed cardiogenic shock requiring dobutamine and norepinephrine, followed by gradual improvement. He was discharged on postoperative day 10.
Histopathological examination confirmed an intrapericardial solitary fibrous tumor.
Solitary fibrous tumors (SFTs) are rare mesenchymal neoplasms most frequently diagnosed in individuals between 50 and 62 years of age
[9]
Gold JS, Antonescu CR, Hajdu C, et al. Clinicopathologic correlates of solitary fibrous tumors. Cancer. 2002; 94(4): 1057‑68.
[9]
. Although the pleura represents the most common site of origin, extrapleural locations including the mediastinum, pericardium, and peritoneum have been documented
[2]
Czimbalmos C, Csecs I, Polos M, et al. Uncommon presentation of a rare tumour—incidental finding in an asymptomatic patient: case report and comprehensive review of the literature on intrapericardial solitary fibrous tumours. BMC Cancer. 2017; 17: 612.
[2]
. Tumor size typically ranges from 7 to 10 cm, consistent with the dimensions observed in our patient
[10]
Demicco EG, Park MS, Araujo DM, et al. Solitary fibrous tumor: a clinicopathological study of 110 cases and proposed risk assessment model. Mod Pathol. 2012; 25(9): 1298‑306.
[10]
.
Intrapericardial SFTs are exceptionally rare. Dyspnea is the predominant symptom due to the mass effect exerted on the heart
[5]
El‑Naggar AK, Ro JY, Ayala AG, et al. Localized fibrous tumor of the serosal cavities: immunohistochemical, electron‑microscopic, and flow‑cytometric DNA study. Am J Clin Pathol. 1989; 92(5): 561‑5.
[6]
Bortolotti U, Calabrò F, Loy M, et al. Giant intrapericardial solitary fibrous tumor. Ann Thorac Surg. 1992; 54(6): 1219‑20.
[7]
Shao D, Wang SX. Pericardial solitary fibrous tumor on FDG PET/CT. Clin Nucl Med. 2019; 44(1): 85‑7.
[8]
Zhang LP, Zhang L, Wang G, et al. Pericardial malignant solitary fibrous tumour with right atrial invasion. J Int Med Res. 2019; 47(6): 2716‑22.
[9]
Gold JS, Antonescu CR, Hajdu C, et al. Clinicopathologic correlates of solitary fibrous tumors. Cancer. 2002; 94(4): 1057‑68.
[10]
Demicco EG, Park MS, Araujo DM, et al. Solitary fibrous tumor: a clinicopathological study of 110 cases and proposed risk assessment model. Mod Pathol. 2012; 25(9): 1298‑306.
[11]
Andreani SM, Tavecchio L, Giardini R, et al. Extrapericardial solitary fibrous tumour of the pericardium. Eur J Cardiothorac Surg. 1998; 14(1): 98‑100.
[5-11]
. Additional manifestations may include anemia, precordial pain, and peripheral edema. Only a limited number of cases have been reported in the literature
[7]
Shao D, Wang SX. Pericardial solitary fibrous tumor on FDG PET/CT. Clin Nucl Med. 2019; 44(1): 85‑7.
[8]
Zhang LP, Zhang L, Wang G, et al. Pericardial malignant solitary fibrous tumour with right atrial invasion. J Int Med Res. 2019; 47(6): 2716‑22.
Table 1. The case of pericardial solitary fibrous tumor in other reported cases.
Author
Year
Age
Sex
Malignancy
Tumor size (cm)
El-Naggar et al
1989
56
F
Benign
13
Bortolotti et al
1992
60
M
Benign
14x7
Andreani et al
1998
60
M
Benign
20x18
Shao et al
2019
51
F
Benign
6.8x7.5
Zhang et al
2019
64
F
Maligant
7.5x3.4
Diagnosis relies on multimodal imaging. Echocardiography often reveals a hyperechogenic mass, sometimes containing small calcifications11. Magnetic resonance imaging (MRI) typically demonstrates low signal intensity on T1‑ and T2‑weighted sequences, with homogeneous enhancement following contrast administration, reflecting the fibrous composition of the tumor
[12]
Maleszewski JJ, Bois MC, Bois JP, et al. Neoplasia and the heart: pathological review with clinical and radiological correlation. J Am Coll Cardiol. 2018; 72(2): 202‑27.
[13]
Maleszewski JJ, Anavekar NS, Moynihan TJ, et al. Pathology, imaging, and treatment of cardiac tumours. Nat Rev Cardiol. 2017; 14(9): 536‑49.
[12, 13]
.
Histopathological examination remains the gold standard for diagnosis. SFTs are composed of spindle‑shaped fibroblasts embedded in collagen, occasionally with calcifications in older lesions. Immunohistochemistry is essential for confirmation, with typical positivity for CD34, CD99, Bcl‑2, and STAT‑6, and negativity for EMA and S100
[3]
Geramizadeh B, Marzban M, Churg A. Role of immunohistochemistry in the diagnosis of solitary fibrous tumor: a review. Iran J Pathol. 2016; 11(3): 195‑203.
[3]
.
Although most SFTs are benign, malignant variants have been reported. This underscores the importance of complete surgical resection and long‑term follow‑up to detect recurrence or metastasis.
4. Conclusion
Intrapericardial solitary fibrous tumors are extremely rare. Complete surgical excision is the treatment of choice. Long‑term follow‑up using computed tomography and magnetic resonance imaging is essential to detect recurrence or malignant transformation.
Pape Amath Diagne: Formal Analysis, Validation, Visualization
Conflicts of Interest
The authors declare no conflicts of interest.
References
[1]
Kallen ME, Hornick JL. The 2020 WHO classification: what’s new in soft tissue tumor pathology? Am J Surg Pathol. 2021; 45: e1–e23.
[2]
Czimbalmos C, Csecs I, Polos M, et al. Uncommon presentation of a rare tumour—incidental finding in an asymptomatic patient: case report and comprehensive review of the literature on intrapericardial solitary fibrous tumours. BMC Cancer. 2017; 17: 612.
[3]
Geramizadeh B, Marzban M, Churg A. Role of immunohistochemistry in the diagnosis of solitary fibrous tumor: a review. Iran J Pathol. 2016; 11(3): 195‑203.
[4]
Szot M, Zub A, Kurzawa P, et al. Cardiac solitary fibrous tumor—an extremely rare but potentially fatal diagnosis. Kardiochir Torakochirurgia Pol. 2024; 21: 39–42.
[5]
El‑Naggar AK, Ro JY, Ayala AG, et al. Localized fibrous tumor of the serosal cavities: immunohistochemical, electron‑microscopic, and flow‑cytometric DNA study. Am J Clin Pathol. 1989; 92(5): 561‑5.
[6]
Bortolotti U, Calabrò F, Loy M, et al. Giant intrapericardial solitary fibrous tumor. Ann Thorac Surg. 1992; 54(6): 1219‑20.
[7]
Shao D, Wang SX. Pericardial solitary fibrous tumor on FDG PET/CT. Clin Nucl Med. 2019; 44(1): 85‑7.
[8]
Zhang LP, Zhang L, Wang G, et al. Pericardial malignant solitary fibrous tumour with right atrial invasion. J Int Med Res. 2019; 47(6): 2716‑22.
[9]
Gold JS, Antonescu CR, Hajdu C, et al. Clinicopathologic correlates of solitary fibrous tumors. Cancer. 2002; 94(4): 1057‑68.
[10]
Demicco EG, Park MS, Araujo DM, et al. Solitary fibrous tumor: a clinicopathological study of 110 cases and proposed risk assessment model. Mod Pathol. 2012; 25(9): 1298‑306.
[11]
Andreani SM, Tavecchio L, Giardini R, et al. Extrapericardial solitary fibrous tumour of the pericardium. Eur J Cardiothorac Surg. 1998; 14(1): 98‑100.
[12]
Maleszewski JJ, Bois MC, Bois JP, et al. Neoplasia and the heart: pathological review with clinical and radiological correlation. J Am Coll Cardiol. 2018; 72(2): 202‑27.
[13]
Maleszewski JJ, Anavekar NS, Moynihan TJ, et al. Pathology, imaging, and treatment of cardiac tumours. Nat Rev Cardiol. 2017; 14(9): 536‑49.
Thiaw, A. A., Diatta, S., Sow, N. F., Diagne, P. A., Mbengue, A. L., et al. (2026). Intrapericardial Solitary Fibrous Tumor Unmasked by Life-threatening Cardiac Tamponade: A Case Report. International Journal of Cardiovascular and Thoracic Surgery, 12(2), 59-62. https://doi.org/10.11648/j.ijcts.20261202.16
Thiaw, A. A.; Diatta, S.; Sow, N. F.; Diagne, P. A.; Mbengue, A. L., et al. Intrapericardial Solitary Fibrous Tumor Unmasked by Life-threatening Cardiac Tamponade: A Case Report. Int. J. Cardiovasc. Thorac. Surg.2026, 12(2), 59-62. doi: 10.11648/j.ijcts.20261202.16
@article{10.11648/j.ijcts.20261202.16,
author = {Abdoul Aziz Thiaw and Souleymane Diatta and Ndeye Fatou Sow and Papa Amath Diagne and Abdou Lahat Mbengue and Moussa Mareme Samba and Dialtabe Ibrahima Ba and Mareme Soda Mbaye and Moussa Seck Diop and Abdou Khoudouss Diallo and Mory Camara and Momar Sokhna Diop and Papa Salmane Ba and Papa Adama Dieng and Amadou Gabriel Ciss},
title = {Intrapericardial Solitary Fibrous Tumor Unmasked by Life-threatening Cardiac Tamponade: A Case Report},
journal = {International Journal of Cardiovascular and Thoracic Surgery},
volume = {12},
number = {2},
pages = {59-62},
doi = {10.11648/j.ijcts.20261202.16},
url = {https://doi.org/10.11648/j.ijcts.20261202.16},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ijcts.20261202.16},
abstract = {Background: Solitary fibrous tumors (SFTs) are rare mesenchymal neoplasms initially described as pleural tumors but now recognized as ubiquitous lesions with variable biological behavior, and intrapericardial SFTs represent an exceptional subset with fewer than a dozen well-documented cases in the literature, their clinical presentation often being nonspecific while life-threatening complications such as cardiac tamponade remain exceedingly rare. Case presentation: A 72-year-old man presented with progressive dyspnea, dry cough, and retrosternal chest pain evolving over three months, culminating in cardiorespiratory distress; clinical examination revealed cardiac tamponade. Echocardiography demonstrated a regular iso-echogenic intrapericardial mass compressing the left cardiac chambers, measuring 12.6 × 9.6 cm, and thoracic CT scan showed a large, well-defined hypodense mass in the anterior mediastinum adjacent to the left cardiac border. A monobloc surgical excision was performed via median sternotomy, and tumor removal resulted in abrupt re-expansion of the cardiac chambers with sudden hypotension requiring fluid resuscitation and vasopressor support. Postoperative evolution was marked by cardiogenic shock on day 1, managed with dobutamine and norepinephrine, followed by progressive improvement allowing discharge on postoperative day 10. Histopathological analysis confirmed an intrapericardial solitary fibrous tumor. Conclusion: Intrapericardial SFTs are extremely rare, complete surgical resection remains the treatment of choice, and long?term imaging follow-up is essential due to the potential for recurrence or malignant transformation.},
year = {2026}
}
TY - JOUR
T1 - Intrapericardial Solitary Fibrous Tumor Unmasked by Life-threatening Cardiac Tamponade: A Case Report
AU - Abdoul Aziz Thiaw
AU - Souleymane Diatta
AU - Ndeye Fatou Sow
AU - Papa Amath Diagne
AU - Abdou Lahat Mbengue
AU - Moussa Mareme Samba
AU - Dialtabe Ibrahima Ba
AU - Mareme Soda Mbaye
AU - Moussa Seck Diop
AU - Abdou Khoudouss Diallo
AU - Mory Camara
AU - Momar Sokhna Diop
AU - Papa Salmane Ba
AU - Papa Adama Dieng
AU - Amadou Gabriel Ciss
Y1 - 2026/03/23
PY - 2026
N1 - https://doi.org/10.11648/j.ijcts.20261202.16
DO - 10.11648/j.ijcts.20261202.16
T2 - International Journal of Cardiovascular and Thoracic Surgery
JF - International Journal of Cardiovascular and Thoracic Surgery
JO - International Journal of Cardiovascular and Thoracic Surgery
SP - 59
EP - 62
PB - Science Publishing Group
SN - 2575-4882
UR - https://doi.org/10.11648/j.ijcts.20261202.16
AB - Background: Solitary fibrous tumors (SFTs) are rare mesenchymal neoplasms initially described as pleural tumors but now recognized as ubiquitous lesions with variable biological behavior, and intrapericardial SFTs represent an exceptional subset with fewer than a dozen well-documented cases in the literature, their clinical presentation often being nonspecific while life-threatening complications such as cardiac tamponade remain exceedingly rare. Case presentation: A 72-year-old man presented with progressive dyspnea, dry cough, and retrosternal chest pain evolving over three months, culminating in cardiorespiratory distress; clinical examination revealed cardiac tamponade. Echocardiography demonstrated a regular iso-echogenic intrapericardial mass compressing the left cardiac chambers, measuring 12.6 × 9.6 cm, and thoracic CT scan showed a large, well-defined hypodense mass in the anterior mediastinum adjacent to the left cardiac border. A monobloc surgical excision was performed via median sternotomy, and tumor removal resulted in abrupt re-expansion of the cardiac chambers with sudden hypotension requiring fluid resuscitation and vasopressor support. Postoperative evolution was marked by cardiogenic shock on day 1, managed with dobutamine and norepinephrine, followed by progressive improvement allowing discharge on postoperative day 10. Histopathological analysis confirmed an intrapericardial solitary fibrous tumor. Conclusion: Intrapericardial SFTs are extremely rare, complete surgical resection remains the treatment of choice, and long?term imaging follow-up is essential due to the potential for recurrence or malignant transformation.
VL - 12
IS - 2
ER -
Thiaw, A. A., Diatta, S., Sow, N. F., Diagne, P. A., Mbengue, A. L., et al. (2026). Intrapericardial Solitary Fibrous Tumor Unmasked by Life-threatening Cardiac Tamponade: A Case Report. International Journal of Cardiovascular and Thoracic Surgery, 12(2), 59-62. https://doi.org/10.11648/j.ijcts.20261202.16
Thiaw, A. A.; Diatta, S.; Sow, N. F.; Diagne, P. A.; Mbengue, A. L., et al. Intrapericardial Solitary Fibrous Tumor Unmasked by Life-threatening Cardiac Tamponade: A Case Report. Int. J. Cardiovasc. Thorac. Surg.2026, 12(2), 59-62. doi: 10.11648/j.ijcts.20261202.16
@article{10.11648/j.ijcts.20261202.16,
author = {Abdoul Aziz Thiaw and Souleymane Diatta and Ndeye Fatou Sow and Papa Amath Diagne and Abdou Lahat Mbengue and Moussa Mareme Samba and Dialtabe Ibrahima Ba and Mareme Soda Mbaye and Moussa Seck Diop and Abdou Khoudouss Diallo and Mory Camara and Momar Sokhna Diop and Papa Salmane Ba and Papa Adama Dieng and Amadou Gabriel Ciss},
title = {Intrapericardial Solitary Fibrous Tumor Unmasked by Life-threatening Cardiac Tamponade: A Case Report},
journal = {International Journal of Cardiovascular and Thoracic Surgery},
volume = {12},
number = {2},
pages = {59-62},
doi = {10.11648/j.ijcts.20261202.16},
url = {https://doi.org/10.11648/j.ijcts.20261202.16},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ijcts.20261202.16},
abstract = {Background: Solitary fibrous tumors (SFTs) are rare mesenchymal neoplasms initially described as pleural tumors but now recognized as ubiquitous lesions with variable biological behavior, and intrapericardial SFTs represent an exceptional subset with fewer than a dozen well-documented cases in the literature, their clinical presentation often being nonspecific while life-threatening complications such as cardiac tamponade remain exceedingly rare. Case presentation: A 72-year-old man presented with progressive dyspnea, dry cough, and retrosternal chest pain evolving over three months, culminating in cardiorespiratory distress; clinical examination revealed cardiac tamponade. Echocardiography demonstrated a regular iso-echogenic intrapericardial mass compressing the left cardiac chambers, measuring 12.6 × 9.6 cm, and thoracic CT scan showed a large, well-defined hypodense mass in the anterior mediastinum adjacent to the left cardiac border. A monobloc surgical excision was performed via median sternotomy, and tumor removal resulted in abrupt re-expansion of the cardiac chambers with sudden hypotension requiring fluid resuscitation and vasopressor support. Postoperative evolution was marked by cardiogenic shock on day 1, managed with dobutamine and norepinephrine, followed by progressive improvement allowing discharge on postoperative day 10. Histopathological analysis confirmed an intrapericardial solitary fibrous tumor. Conclusion: Intrapericardial SFTs are extremely rare, complete surgical resection remains the treatment of choice, and long?term imaging follow-up is essential due to the potential for recurrence or malignant transformation.},
year = {2026}
}
TY - JOUR
T1 - Intrapericardial Solitary Fibrous Tumor Unmasked by Life-threatening Cardiac Tamponade: A Case Report
AU - Abdoul Aziz Thiaw
AU - Souleymane Diatta
AU - Ndeye Fatou Sow
AU - Papa Amath Diagne
AU - Abdou Lahat Mbengue
AU - Moussa Mareme Samba
AU - Dialtabe Ibrahima Ba
AU - Mareme Soda Mbaye
AU - Moussa Seck Diop
AU - Abdou Khoudouss Diallo
AU - Mory Camara
AU - Momar Sokhna Diop
AU - Papa Salmane Ba
AU - Papa Adama Dieng
AU - Amadou Gabriel Ciss
Y1 - 2026/03/23
PY - 2026
N1 - https://doi.org/10.11648/j.ijcts.20261202.16
DO - 10.11648/j.ijcts.20261202.16
T2 - International Journal of Cardiovascular and Thoracic Surgery
JF - International Journal of Cardiovascular and Thoracic Surgery
JO - International Journal of Cardiovascular and Thoracic Surgery
SP - 59
EP - 62
PB - Science Publishing Group
SN - 2575-4882
UR - https://doi.org/10.11648/j.ijcts.20261202.16
AB - Background: Solitary fibrous tumors (SFTs) are rare mesenchymal neoplasms initially described as pleural tumors but now recognized as ubiquitous lesions with variable biological behavior, and intrapericardial SFTs represent an exceptional subset with fewer than a dozen well-documented cases in the literature, their clinical presentation often being nonspecific while life-threatening complications such as cardiac tamponade remain exceedingly rare. Case presentation: A 72-year-old man presented with progressive dyspnea, dry cough, and retrosternal chest pain evolving over three months, culminating in cardiorespiratory distress; clinical examination revealed cardiac tamponade. Echocardiography demonstrated a regular iso-echogenic intrapericardial mass compressing the left cardiac chambers, measuring 12.6 × 9.6 cm, and thoracic CT scan showed a large, well-defined hypodense mass in the anterior mediastinum adjacent to the left cardiac border. A monobloc surgical excision was performed via median sternotomy, and tumor removal resulted in abrupt re-expansion of the cardiac chambers with sudden hypotension requiring fluid resuscitation and vasopressor support. Postoperative evolution was marked by cardiogenic shock on day 1, managed with dobutamine and norepinephrine, followed by progressive improvement allowing discharge on postoperative day 10. Histopathological analysis confirmed an intrapericardial solitary fibrous tumor. Conclusion: Intrapericardial SFTs are extremely rare, complete surgical resection remains the treatment of choice, and long?term imaging follow-up is essential due to the potential for recurrence or malignant transformation.
VL - 12
IS - 2
ER -