Abstract
Background: Acute heart failure represents a significant public health concern worldwide, posing a considerable burden on healthcare systems and often leading to adverse clinical outcomes, including high mortality rates. Thus, this study aimed to describe the in-hospital outcomes and associated factors for patients with acute heart failure. Which is vital for improving the quality of care and patient management. Objective: To determine clinical characteristics and in hospital outcome of acute heart failure patient admitted at Asella teaching and referral hospital. Methodology: The study employed an institution-based retrospective cohort design and assessed the clinical characteristics and in-hospital outcomes of acute heart failure (AHF) patients admitted to Asella Teaching and Referral Hospital. Data were collected from all patients admitted between September 2022 and September 2023. After manual checks for completeness, the data were coded and entered using Epi Info version 7.2 and analyzed with SPSS version 28. Descriptive statistics were used, presenting continuous variables as mean standard deviation or median (interquartile range) based on distribution either normal or not, respectively. In addition, categorical variables were presented as frequency and percentages. Kaplan-Meier method estimated and graphed survival probabilities over time and a Log-rank hypothesis test to compare survival functions of explanatory variables was utilized. Significant predictor variables were identified by fitting a semi parametric Cox’s proportional hazard model using a method of forward stepwise and statistical significance variables were declared based on a p-value less than 0.05. Result: Two hundred thirty one (231) patients were included in the study, with 121 (52.4%) being female. The median age of patients with acute heart failure was 56 years (IQR = 28 to 70). The commonest underlying disease and precipitating factor identified at admission was ischemic heart disease (36.4%) and pneumonia (24.68%) respectively. Out of the 231 patients, 13.4% died in the hospital. In the survival analysis the hazard ratios for precipitant factor pneumonia, acute kidney injury, lack of health insurance and age were identified 3.07 (95% CI: 1.40, 6.74, p = 0.005), 2.98 (95% CI: 1.31, 6.75, p = 0.009), 3.46 (95% CI: 1.51, 7.95, p = 0.003), and 2.81 (95% CI: 1.18, 6.72, p = 0.020), respectively as predictors of poor treatment outcome. Conclusion: Unfortunately, the in-hospital mortality rate for acute heart failure proved to be high in this study. The identified independent predictors of in-hospital mortality included pneumonia, acute kidney injury, lack of active health insurance coverage and age. The principal precipitating factors leading to hospitalization were pneumonia. Ischemic heart disease was identified as the most common underlying cardiac disease. Recommendation: Improve the consistency and availability of essential investigations. work on improving drug adherence and health insurance coverage.
Keywords
Acute Heart Failure, Clinical Characteristics, In Hospital Outcome, Asella, Ethiopia and Sub-Saharan Africa
1. Introduction
Heart failure is a clinical syndrome where the heart is unable to pump enough blood to meet the body's demand, resulting in observable symptoms and signs. Acute heart failure refers to the sudden or rapid onset of symptoms and signs of heart failure that require urgent medical attention
| [1] | McDonagh TA, Metra M, Adamo M, Gardner RS, Baumbach A, Böhm M, et al. 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur Heart J. 2021; 42(36): 3599-726. |
| [2] | Campos-Arjona R, García-Pinilla JM, de Teresa-Galván E. Acute heart failure. Med. 2019; 12(89): 5237-44. |
[1, 2]
.
Commonly presented symptoms include dyspnea during exercise or at rest, orthopnea, fatigue, and reduced exercise tolerance. Clinical signs of congestion, such as peripheral edema, jugular vein distension, and S3 gallop, often accompany symptoms. AHF is classified into two groups according to the presence or absence of previous HF: Worsening (decompensated) preexisting stable HF suddenly or progressively described as decompensated AHF, and New (de novo) HF, where there is no known previous HF
| [1] | McDonagh TA, Metra M, Adamo M, Gardner RS, Baumbach A, Böhm M, et al. 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur Heart J. 2021; 42(36): 3599-726. |
| [5] | Gallagher J, McDonald K, Ledwidge M, Watson CJ. Heart Failure in Sub-Saharan Africa. Card Fail Rev. 2018; 4(1): 1. |
| [3] | Ural D, Çavuşoğlu Y, Eren M, Karaüzüm K, Temizhan A, Yılmaz MB, et al. Akut kalp yetersizliği tanı ve tedavisi. Anatol J Cardiol. 2015; 15(11): 860-89. |
[1, 5, 3]
.
Based on the presence of signs of congestion and/or peripheral hypo perfusion, there are four major clinical presentations of acute heart failure, with possible overlaps between them: Acutely decompensated heart failure, acute pulmonary edema, Isolated right ventricular failure, and Cardiogenic shock
| [1] | McDonagh TA, Metra M, Adamo M, Gardner RS, Baumbach A, Böhm M, et al. 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur Heart J. 2021; 42(36): 3599-726. |
[1]
.
The diagnosis requires the presence of symptoms and/or signs of AHF and supporting evidence from investigations such as signs of pulmonary edema and cardiomegaly on chest X-ray, echocardiogram (ECHO) findings, and elevated cardiac biomarkers like BNP (≥100 pg/mL), NT-proBNP (≥300 pg/mL), MR-proANP (≥120 pg/mL), and ECG
| [1] | McDonagh TA, Metra M, Adamo M, Gardner RS, Baumbach A, Böhm M, et al. 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur Heart J. 2021; 42(36): 3599-726. |
[1]
.
The goal of treatment should be to reverse acute hemodynamic abnormalities, quickly relieve symptoms, and initiate treatments that will decrease disease progression and improve survival. The management can be simplified and improved by assessing the most likely hemodynamic profile based on clinical signs and symptoms
| [1] | McDonagh TA, Metra M, Adamo M, Gardner RS, Baumbach A, Böhm M, et al. 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur Heart J. 2021; 42(36): 3599-726. |
| [4] | Heidenreich PA, Bozkurt B, Aguilar D, Allen LA, Byun JJ, Colvin MM, et al. 2022 AHA/ACC/HFSA Guideline for the Management of Heart Failure: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Vol. 145, Circulation. 2022. 895-1032 p. |
[1, 4]
.
Patients with heart failure who are admitted with evidence of significant fluid overload should be treated with intravenous loop diuretics to improve symptoms and reduce morbidity. In addition, vasodilation therapy may be considered an adjuvant to diuretic therapy for the relief of dyspnea. In patients with cardiogenic shock, intravenous inotropic support should be used to maintain systemic perfusion and preserve end-organ perfusion. It is also important to monitor the patient's oxygen levels and provide oxygen for patient with hypoxia. In addition Hospitalization is a critical opportunity to continue, initiate, and further optimize GDMT
| [4] | Heidenreich PA, Bozkurt B, Aguilar D, Allen LA, Byun JJ, Colvin MM, et al. 2022 AHA/ACC/HFSA Guideline for the Management of Heart Failure: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Vol. 145, Circulation. 2022. 895-1032 p. |
[4]
.
A significant public health issue that affects millions of people worldwide, with a high rate of hospitalization, readmissions, and mortality. In contrast to the substantial improvements in the treatment of chronic HF, AHF is still associated with poor outcomes, with 90-day readmission rates and 1-year mortality reaching 10-30%. There are also significant variations in the etiology, clinical presentation, treatment, and outcome of heart failure globally
| [8] | Dokainish H, Teo K, Zhu J, Roy A, Alhabib KF, Elsayed A, et al. Heart Failure in Africa, Asia, the Middle East and South America: The INTER-CHF study. Int J Cardiol. 2016; 204: 133-41. Available from: http://dx.doi.org/10.1016/j.ijcard.2015.11.183 |
[8]
.
In developed countries, AHF is common in the seventh decade of life and is associated with high mortality and re-hospitalization rates. In-hospital mortality ranges from 4% to 10%, and post-discharge 1-year mortality can be 25-30%, with up to more than 45% deaths or readmission rates
| [1] | McDonagh TA, Metra M, Adamo M, Gardner RS, Baumbach A, Böhm M, et al. 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur Heart J. 2021; 42(36): 3599-726. |
[1]
.
In Africa, the incidence is increasing, this is mainly due to increase in cardio vascular risk factors, including an aging population, hypertension and diabetes, and limited access to healthcare services. The reported hospital prevalence studies indicate that HF is responsible for 9.4-42.5% of all medical admissions
| [9] | S. Ogah O, Adebiyi A, Sliwa K. Heart Failure in Sub-Saharan Africa. Top Hear Fail Manag. 2019. |
| [10] | Olatayo Adeoti A, Adekunle Ajayi E, Oladimeji Ajayi A, Ayokunle Dada S, Olusesan Fadare J, Akolawole M, et al. Pattern and Outcome of Medical Admissions in Ekiti State University Teaching Hospital, Ado-Ekiti-A 5 Year Review. Am J Med Med Sci. 2015; 2015(2): 92-8. Available from: http://journal.sapub.org/ajmms |
| [11] | Elyamani R, Soulaymani A, Hami H. Epidemiology of Cardiovascular Diseases in Morocco: A Systematic Review. Rev Diabet Stud. 2021; 17(2): 57-67. |
[9-11]
. Moreover, most of these patients are young. Therefore strikes patients in the prime of their lives, with major economic implications because it affects the generation of breadwinners and caregivers. In addition, most of patients live in rural areas where health care access is limited and transportation is difficult. Therefore, they present late with sever symptom. There is varying gender distribution. It is more common in men, where hypertensive heart disease is the commonest etiology. In women, rheumatic heart disease and cardiomyopathies (such as peripartum cardiomyopathy) are predominant
| [6] | Damasceno A, Mayosi BM, Sani M, Ogah OS, Mondo C, Ojji D, et al. The causes, treatment, and outcome of acute heart failure in 1006 Africans from 9 countries: Results of the sub-Saharan Africa survey of heart failure. Arch Intern Med. 2012; 172(18): 1386-94. |
| [8] | Dokainish H, Teo K, Zhu J, Roy A, Alhabib KF, Elsayed A, et al. Heart Failure in Africa, Asia, the Middle East and South America: The INTER-CHF study. Int J Cardiol. 2016; 204: 133-41. Available from: http://dx.doi.org/10.1016/j.ijcard.2015.11.183 |
| [12] | Ogah OS, Stewart S, Falase AO, Akinyemi JO, Adegbite GD, Alabi AA, et al. Contemporary profile of acute heart failure in Southern Nigeria: Data from the abeokuta heart failure clinical registry. JACC Hear Fail. 2014; 2(3): 250-9. |
| [13] | Makubi A, Hage C, Lwakatare J, Kisenge P, Makani J, Rydén L, et al. Contemporary aetiology, clinical characteristics and prognosis of adults with heart failure observed in a tertiary hospital in Tanzania: The prospective Tanzania Heart Failure (TaHeF) study. Heart. 2014; 100(16): 1235-41. |
| [14] | Okello S, Rogers O, Byamugisha A, Rwebembera J, Buda AJ. Characteristics of acute heart failure hospitalizations in a general medical ward in Southwestern Uganda. Int J Cardiol. 2014; 176(3): 1233-4. Available from: http://dx.doi.org/10.1016/j.ijcard.2014.07.212 |
| [15] | Tirfe M, Nedi T, Mekonnen D, Berha AB. Treatment outcome and its predictors among patients of acute heart failure at a tertiary care hospital in Ethiopia: a prospective observational study. BMC Cardiovasc Disord. 2020; 20(1): 16. Available from: https://doi.org/10.1186/s12872-019-01318-x |
| [16] | Tirfe M, Nedi T MD. Treatment outcome and associated factors in acute heart failure patients at Tikur Anbessa Specialized Hospital, Addis Ababa, Ethiopia. BMC Cardiovasc Disord. 2018; 20(1): 1-10. |
| [17] | Mwita JC, Dewhurst MJ, Magafu MGMD, Goepamang M, Omech B, Majuta KL, et al. Presentation and mortality of patients hospitalised with acute heart failure in Botswana. Cardiovasc J Afr. 2017; 28(2): 112-7. |
[6, 8, 12-17]
.
The burden becomes even more significant when we consider that most of the patients hospitalized with AHF are readmitted shortly after hospital discharge, and that hospital readmission is one of the main risk factors for death in this syndrome. A number of factors have been identified as precipitating acute HF hospitalizations. These include: pneumonia, atrial fibrillation, anemia, and drug discontinuation
| [6] | Damasceno A, Mayosi BM, Sani M, Ogah OS, Mondo C, Ojji D, et al. The causes, treatment, and outcome of acute heart failure in 1006 Africans from 9 countries: Results of the sub-Saharan Africa survey of heart failure. Arch Intern Med. 2012; 172(18): 1386-94. |
[6]
. Understanding the precipitating factors that lead to acute HF hospitalizations, particularly those that are avoidable, is of great importance in reducing the HF disease burden and improve outcomes
| [11] | Elyamani R, Soulaymani A, Hami H. Epidemiology of Cardiovascular Diseases in Morocco: A Systematic Review. Rev Diabet Stud. 2021; 17(2): 57-67. |
[11]
.
The cost of HF in Nigeria in the year 2009 was estimated at 508,595 USD, translating to 2128 USD per patient per year. In-patient and outpatient care cost constituted 46 and 54% of total care cost, respectively. The relatively higher cost of outpatient care cost was attributed to the cost of transportation for monthly follow-up visits. Payment for the care of HF is out-of-pocket in most parts of SSA
| [9] | S. Ogah O, Adebiyi A, Sliwa K. Heart Failure in Sub-Saharan Africa. Top Hear Fail Manag. 2019. |
[9]
.
The management of AHF in Africa is also complicated by a lack of access to diagnostic and therapeutic resources. Many hospitals in Africa lack the equipment and personnel necessary for the proper diagnosis and management. This can lead to a delay in the diagnosis and treatment, which can worsen the outcomes for patients. Additionally, the limited availability of medical treatments, further exacerbates the problem
| [7] | Gtif I, Bouzid F, Charfeddine S, Abid L, Kharrat N. Heart failure disease: An African perspective. Arch Cardiovasc Dis. 2021; 114(10): 680-90. |
| [8] | Dokainish H, Teo K, Zhu J, Roy A, Alhabib KF, Elsayed A, et al. Heart Failure in Africa, Asia, the Middle East and South America: The INTER-CHF study. Int J Cardiol. 2016; 204: 133-41. Available from: http://dx.doi.org/10.1016/j.ijcard.2015.11.183 |
| [18] | Carlson S, Duber HC, Achan J, Ikilezi G, Mokdad AH, Stergachis A, et al. Capacity for diagnosis and treatment of heart failure in sub-Saharan Africa. Heart. 2017; 103(23): 1874-9. |
| [19] | Talle MA, Bonny A, Scholtz W, Chin A, Nel G, Karaye KM, et al. Status of cardiac arrhythmia services in Africa in 2018: A PAsCAr sudden Cardiac death task Force report. Cardiovasc J Afr. 2018; 29(2): 115-21. |
| [20] | Bukhman AK, Nsengimana VJP, Lipsitz MC, Henwood PC, Tefera E, Rouhani SA, et al. Diagnosis and Management of Acute Heart Failure in Sub-Saharan Africa. Curr Cardiol Rep. 2019; 21(10). |
| [23] | Tigabe M, Fentahun A, Getawa S, Gelaye KA, Gebreyohannes EA. Clinical Characteristics and In-Hospital Outcome of Acute Heart Failure Patients Admitted to the Medical Ward of University of Gondar Comprehensive Specialized Hospital, Northwest Ethiopia. Vasc Health Risk Manag. 2021; 17: 581-90. Available from: https://www.tandfonline.com/doi/abs/10.2147/VHRM.S322493 |
[7, 8, 18-20, 23]
.
Furthermore, studies have shown that African patients with AHF are more likely to have comorbidities such as hypertension, diabetes, and chronic kidney disease, which can exacerbate the symptoms of AHF and make treatment more complex. These comorbidities are often poorly controlled, which further increases the risk of poor outcomes in this population. The high rates of hospitalization is a significant burden on the healthcare system, which is already stretched due to limited resources and a shortage of healthcare professionals
| [6] | Damasceno A, Mayosi BM, Sani M, Ogah OS, Mondo C, Ojji D, et al. The causes, treatment, and outcome of acute heart failure in 1006 Africans from 9 countries: Results of the sub-Saharan Africa survey of heart failure. Arch Intern Med. 2012; 172(18): 1386-94. |
| [9] | S. Ogah O, Adebiyi A, Sliwa K. Heart Failure in Sub-Saharan Africa. Top Hear Fail Manag. 2019. |
| [12] | Ogah OS, Stewart S, Falase AO, Akinyemi JO, Adegbite GD, Alabi AA, et al. Contemporary profile of acute heart failure in Southern Nigeria: Data from the abeokuta heart failure clinical registry. JACC Hear Fail. 2014; 2(3): 250-9. |
| [13] | Makubi A, Hage C, Lwakatare J, Kisenge P, Makani J, Rydén L, et al. Contemporary aetiology, clinical characteristics and prognosis of adults with heart failure observed in a tertiary hospital in Tanzania: The prospective Tanzania Heart Failure (TaHeF) study. Heart. 2014; 100(16): 1235-41. |
| [14] | Okello S, Rogers O, Byamugisha A, Rwebembera J, Buda AJ. Characteristics of acute heart failure hospitalizations in a general medical ward in Southwestern Uganda. Int J Cardiol. 2014; 176(3): 1233-4. Available from: http://dx.doi.org/10.1016/j.ijcard.2014.07.212 |
| [24] | James SL, Abate D, Abate KH, Abay SM, Abbafati C, Abbasi N, et al. Global, regional, and national incidence, prevalence, and years lived with disability for 354 Diseases and Injuries for 195 countries and territories, 1990-2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet. 2018; 392(10159): 1789-858. |
[6, 9, 12-14, 24]
.
A study conducted in Uganda has shown a higher mortality rate (18.3%) and a thirty-day readmission rate (35%) for acute heart failure. This might be attributed to poor utilization of evidence-based therapies. Hypertension (HTN) was the most common comorbidity identified, followed by chronic kidney disease (CKD)
| [22] | Boombhi J, Moampea M, Kuate L, Menanga A, Hamadou B, Kingue S. Clinical Pattern and Outcome of Acute Heart Failure at the Yaounde Central Hospital. OALib. 2017; 04(03): 1-8. |
| [25] | Groenewegen A, Rutten FH, Mosterd A, Hoes AW. Epidemiology of heart failure Measuring an epidemic. 2020; 7-9. |
[22, 25]
.
Similarly, in studies conducted at Jimma and Gondar hospitals, the mortality rate during admission is 20.4% and 17%, respectively. The presence of smoking, diabetes mellitus, pulmonary hypertension, and the occurrence of adverse drug events have been associated with poor in-hospital outcomes
| [15] | Tirfe M, Nedi T, Mekonnen D, Berha AB. Treatment outcome and its predictors among patients of acute heart failure at a tertiary care hospital in Ethiopia: a prospective observational study. BMC Cardiovasc Disord. 2020; 20(1): 16. Available from: https://doi.org/10.1186/s12872-019-01318-x |
| [13] | Makubi A, Hage C, Lwakatare J, Kisenge P, Makani J, Rydén L, et al. Contemporary aetiology, clinical characteristics and prognosis of adults with heart failure observed in a tertiary hospital in Tanzania: The prospective Tanzania Heart Failure (TaHeF) study. Heart. 2014; 100(16): 1235-41. |
[15, 13]
.
This study fills a notable gap in the literature, as there is currently no published research on acute heart failure conducted in Asella. The research aimed to evaluate the clinical characteristics and in-hospital outcomes of acute heart failure patients admitted to Asella Referral and Teaching Hospital.
2. Method and Materials
2.1. Study Area and Period
The hospital is located in Asella town. Arsi zone, Oromia. The town is located 175 km southeast of the capital Addis Ababa. The estimated population at mid-2022 was 139,537, of whom 69,459 were male and 70,078 were female
| [45] | CSA ECSA. Ethiopian 2022 Project Population Census. 2022; (July). |
[45]
. Asella referral and teaching hospital is administered by Arsi University and serves a catchment population of 3.5 million. It has 52 beds in the medical ward, 6 bed in ICU, 4 in HDU.
2.2. Study Design
Institution-based retrospective cohort study was utilized to evaluate clinical characteristics and in hospital outcomes of acute heart failure patients admitted to ARTH.
2.3. Source and Study Population
2.3.1. Source Population
The source population was patients admitted to medical ward, ICU and HDU of ARTHfrom September -, 2022 and August -, 2023.
2.3.2. Study Population
The study population was patients admitted to medical ward, ICU and HDU of ARTH with a diagnosis of AHF during from September -, 2022 and August -, 2023.
2.4. Study Period
Study was conducted from November 1, 2023 to January 31, 2024 at ARTH.
2.5. Eligibility Criteria
2.5.1. Inclusion Criteria
Diagnosis of AHF
Age > 15
Patients who stay for more than 24 hr
2.5.2. Exclusion Criteria
Patients with unknown outcome
Advanced malignancy
Stage 4 HIV
2.5.3. Sample Size Determination
Sample size was determined based on time period of admission, all patients admitted for one year from September, 2022 to August, 2023.
2.6. Variables of the Study
2.6.1. Dependent Variable
The primary outcome of our research is in-hospital mortality. Secondary outcomes include patients leaving against medical advice and improvements in health status at discharge, measured by improved NYHA functional class and resolution of edema. The study endpoint is the duration in days from admission to events such as death, discharge with the same condition, improvement, or leaving against medical advice.
2.6.2. Independent Variables
1) Socio-demographic: age, gender, insurance coverage.
2) Life-styles variables: smoking, alcohol drinking.
3) Vital signs (PR, BP, PR, SPo2, Temperature, Urine output).
4) Framingham major (Acute pulmonary edema, cardiomegaly, neck vein distension, paroxysmal nocturnal dyspnea, orthopnea, rales and S3 gallop).
5) Minor criteria (Nocturnal cough, hepatomegaly, pleural effusion, decrease in vital capacity by one third from maximum recorded, tachycardia (heart rate>120 beats/min).
6) Heart failure syndrome (De novo, worsening of chronic heart failure).
7) Hemodynamic profile (CS, PE, ADHF, RHF).
8) Number of readmission.
9) Imaging study (ECHO, ECG, CXR).
10) Laboratory values (serum Na, serum K, creatinine, BUN, Hemoglobin, Troponin).
11) Precipitating factors: infection, noncompliance with medication, noncompliance with salt restriction, anemia, ACS, uncontrolled HTN, arrhythmia, pulmonary embolism, pregnancy, worsening of renal function.
12) Underlying disease: IHD, VHD, cardiomyopathy, HHD, Cor-pulmonale, degenerative valvular heart disease, congenital heart disease.
13) Co-morbid variables: CKD, DM, HIV/AIDS, HTN, COPD, Dyslipidemia, Cancer, Arrhythmia.
14) Drug use assessment: the medication the patient is on before admission, during admission and discharge (beta blocker, ACEI, ARBS, Aspirin, Atorvastatin, Mineralocorticoid receptor antagonist, Adenosine, Amiodarone, Calcium channel blocker, Digoxin, Diuretics, Dopamine, Labetalol, Norepinephrine, Vasodilator) and adverse drug reactions/side-effect.
2.7. Operational Definitions
Acute heart failure: sign and symptoms of new onset of HF and/or decompensation or worsening of chronic stable HF
| [1] | McDonagh TA, Metra M, Adamo M, Gardner RS, Baumbach A, Böhm M, et al. 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur Heart J. 2021; 42(36): 3599-726. |
| [30] | Kurmani S, Squire I. Acute Heart Failure: Definition, Classification and Epidemiology. Curr Heart Fail Rep. 2017; 14(5): 385-92. |
[1, 30]
.
AKI: defined as any of the following: Increase in Cr by ≥0.3 mg/dl within 48 hours or increase in Cr to ≥1.5 times baseline, which is known or presumed to have occurred within the prior 7 days; or urine volume <0.5 ml/kg/h for 6 hours
| [46] | Chen X. Chinese clinical practice guideline for acute kidney injury. Natl Med J China. 2023; 103(42): 3332-66. |
[46]
.
Improved: is defined as hemodynamically stable, decongested, started on oral evidence based medications and tolerated at least for 24 hr before discharge
| [1] | McDonagh TA, Metra M, Adamo M, Gardner RS, Baumbach A, Böhm M, et al. 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur Heart J. 2021; 42(36): 3599-726. |
[1]
.
In hospital mortality: defined as death occurring during hospitalization for acute heart failure.
Heavy drinking: for men consuming more than 15 drinks per week, for women more than 8 drinks per weak
| [47] | Is H, Use A. Preventing Cancer by Reducing Excessive Alcohol Use How Is Alcohol Use Defined ? What Is Considered One Drink ? What Are the Guidelines for Alcohol Use ?: 23-4. |
[47]
.
Moderate drinking: 2 drinks or less in a day for men, 1 drink or less in day for women
| [47] | Is H, Use A. Preventing Cancer by Reducing Excessive Alcohol Use How Is Alcohol Use Defined ? What Is Considered One Drink ? What Are the Guidelines for Alcohol Use ?: 23-4. |
[47]
.
Poor outcome: the attainment of one of the following end results; death and self-discharge against medical advice with no improvement.
Readmission: is when the same patient was admitted within in the one year period from September 2022 to August 2023.
Smoker: A patient who has smoked 100 cigarettes or more in his or her lifetime and who currently smokes cigarettes
| [48] | Keller K. National Center for Health Statistics. Encycl Obes. 2014; 23-4. |
[48]
.
The same: if there is no significant change in hemodynamic status (requiring IV diuretics, vasopressor, inotropes, HR>100 beat/min or patient in shock) or congested during discharge.
Treatment outcome: the attainment of a specified end result measured using parameters such as improved and/or died.
2.8. Data Collection Procedures
The data extraction checklist for this study were meticulously designed in accordance with established guidelines, including the Ethiopian National Guideline on major non-communicable diseases (2016), the European Society of Cardiology (ESC) guidelines from 2021, and the ACC/AHA guidelines and definitions
| [1] | McDonagh TA, Metra M, Adamo M, Gardner RS, Baumbach A, Böhm M, et al. 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur Heart J. 2021; 42(36): 3599-726. |
| [31] | Bocchi EA. Heart Failure in South America. 2013; 147-56. |
| [4] | Heidenreich PA, Bozkurt B, Aguilar D, Allen LA, Byun JJ, Colvin MM, et al. 2022 AHA/ACC/HFSA Guideline for the Management of Heart Failure: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Vol. 145, Circulation. 2022. 895-1032 p. |
| [49] | Survey H. Ethiopia. 2016. |
[1, 31, 4, 49]
. This comprehensive checklist include a range of crucial elements such as socio-demographic details, clinical characteristics, precipitating factors, underlying diseases, co-morbidities, and imaging studies, including chest X-ray, electrocardiogram, and echocardiography. Additionally, the checklist captures essential information on the treatment administered and the duration of hospital stay. Furthermore, the data extraction process involved the systematic collection of vital signs and laboratory values, including serum sodium, potassium, hemoglobin, serum creatinine, blood urea nitrogen (BUN), troponin, and the estimated glomerular filtration rate (GFR) based on the CKD-EPI derived formula. We evaluate the outcome from the last admission. Data was collected using pretested format, by two trained Nurses. Relevant clinical information and data was obtained from patient charts.
2.9. Data Quality Assurance
One day training was given for data collector before entering into data collection process on the objective and relevance of the study, how to gather the appropriate information, procedures of data collection techniques and the whole contents of the checklist. The data collection process and completeness was closely supervised. Pre-test was done to assure clarity, avoidance of ambiguity, comprehensiveness and content uniformity.
2.10. Data Processing and Analysis
The collected data after manually checked for completeness was entered and coded using Epi info version 5.0 and analyzed using Statistical Package for Social Sciences (SPSS) version 28. Continuous variables was presented as mean (SD) for normal distributed, otherwise median (inter-quartile range) for non-normal distributed variables. Categorical variables were reported as percentages and frequency tables. Kaplan-Meier method estimated and graphed survival probabilities over time and a Log-rank hypothesis test to compare survival functions of explanatory variables was utilized. Significant predictor variables were identified by fitting a semi parametric Cox’s proportional hazard model using a method of forward stepwise and statistical significance variables were declared based on a p-value less than 0.05.
2.11. Ethical Considerations
Proposal approval was obtained before the beginning of data collection from the Departmental Research and Promotion Committee (DRPC) of the Department of internal medicine, CHS. Permission for data collection was obtained from hospital administrative body. Confidentiality and anonymity of the client’s information was ensured throughout the execution of the study by taking only the required information without using the name of the client. Identification numbers was used rather than names to identify patients.
3. Result
3.1. Socio-Demographic Characteristics and Lifestyle Factors
From September 2022 to August 2023 at Asela Referral Hospital, 262 patients where admitted with the diagnosis of acute heart failure. Data was extracted from 231 patients’ medical record following the exclusion of 12 individuals based on predetermined criteria. Among those excluded, four patients exhibited stage 4 RVI, while three presented with advanced malignancies, including two cases of stage 4 cervical cancer and one case of stage 4 lung cancer. An additional five patients were discharged within 24 hours of admission, and records for 19 cases were inaccessible, having been misplaced from the medical record repository.
Within the group of 231 admitted patients with acute heart failure, more than half (52.4%) of admitted patients were females and majority (72.4%) are rural residents. One hundred forty two (61.5%) patients had active health insurance coverage. Around twelve percent (11.6%) of individuals reported a history of cigarette smoking, and among them, 40.7% were active smokers upon admission. For those classified as former smokers, the average duration since discontinuation was 2.9 years. Additionally, 22 participants (9.5%) had a history of alcohol intake, and considerable portion of these individuals (81%) reported heavy alcohol consumption (
Table 1).
Table 1. Sociodemographic characteristics and lifestyle factors of patient admitted with acute heart failure to Asella referral and teaching hospital, Asella 2024.
Variables | Frequency (%) | Mean | SD | Median | Q1 | Q3 |
Age | | 51 | 24 | 56 | 28 | 70 |
15-40 | 88 (38.1%) | | | | | |
40-64 | 60 (26.0%) | | | | | |
≥65 | 83 (35.9%) | | | | | |
Sex | | | | | | |
female | 121 (52.4%) | | | | | |
Male | 110 (47.6%) | | | | | |
Address | | | | | | |
Urban | 64 (27.7%) | | | | | |
Rural | 167 (72.3%) | | | | | |
Active health insurance | | | | | | |
Yes | 142 (61.5%) | | | | | |
No | 89 (38.5%) | | | | | |
Smoking | | | | | | |
Yes | 27 (11.7%) | | | | | |
Active smoker | 11 (40.7%) | | | | | |
Ex-smoker | 16 (59.3) | | | | | |
No | 203 (87.9%) | | | | | |
Alcohol | | | | | | |
Yes | 22 (9.5%) | | | | | |
Moderate | 4 (18.2) | | | | | |
Heavy | 18 (81.8) | | | | | |
No | 209 (90.5%) | | | | | |
Key: SD = standard deviation; Q1. = 25th percentile, Q3 = 75th percentile
3.2. Clinical Characteristics of Patients at Admission
Among 231 patients admitted with acute heart failure during study interval, more than half of the patient 143 (61.9%) had worsening of preexisting chronic heart failure, 88 (38.1%) had de novo heart failure at admission. More than two-thirds of the patients 187 (81.0%) present with NYHA class IV, 44 (19.0%) NYHA class III. Upon admission 180 (97.8%) were classified as having stage C heart failure, while four (2.2%) were categorized as stage D. The hemodynamic profiles were categorized as follows: 149 cases (64.5%) exhibited a warm and wet profile, 64 cases (27.7%) presented as warm and dry, 13 cases (5.6%) demonstrated a cold and wet profile, and five cases (2.2%) were characterized as cold and dry (
Table 2).
Table 2. Clinical characteristics of acute heart failure patients admitted to Asella referral and teaching hospital, Asella 2024.
Classification | | Frequency (%) |
Heart failure syndrome | Chronic HF worsens | 143 (61.9%) |
New ‘de novo’ | 88 (38.1%) |
Functional class | NYHA class III | 44 (19.0%) |
NYHA class IV | 187 (81.0%) |
Heart failure stage | Stage C | 180 (97.8%) |
Stage D | 4 (2.2%) |
Congestion/hypoperfusion | Warm and wet | 149 (64.5%) |
Warm and dry | 64 (27.7%) |
Cold and wet | 13 (5.6%) |
Cold and dry | 5 (2.2%) |
Hemodynamic profile | ADHF | 148 (64.1%) |
RHF | 36 (15.6%) |
PE | 28 (12.1%) |
CS | 19 (8.2%) |
Key: ADHF = Acute decompensated heart failure, NYHA = New York Heart Association, RHF: Right-Sided Heart Failure, PE: Pulmonary Embolism, CS: Cardiogenic Shock, HF= heart failure
The average systolic admission blood pressure (SBP) recorded was 111 ± 27 mmHg. According to the ACC/AHA 2017 guidelines on hypertension, 131 patients (56.7%) out of the total 231 presented with a normal SBP upon admission, while 12 (5.2%), 19 (8.2%), and 26 (11.3%) presented with elevated, Stage I, and Stage II blood pressure, respectively. Additionally, 43 patients (18.61%) had systolic blood pressure below 90 mmHg. Furthermore, thirty-eight individuals (16.45%) had a diastolic blood pressure below 60 mmHg, whereas the majority of patients (63.63%) presented with a normal diastolic blood pressure. The mean pulse rate was 105 ± 48 beats per minute, with 102 patients (44.2%) exhibiting an admission pulse rate exceeding 100 beats per minute. Urine output data were documented for 201 patients, revealing a mean ± (SD) value of 2.1 ± 1.03 (
Table 3).
Table 3. Blood pressure, pulse rate and urine output, length of hospital stay and readmission of acute heart failure patients admitted to Asella referral and teaching hospital, Asella 2024.
Variable | Frequency (%) | Mean | SD | Median | Q1 | Q2 |
Systolic blood pressure, mmHg (N=231) | | 111 | 27 | 106 | 99 | 125 |
Normal (<120 mmHg) | 131 (56.7%) | | | | | |
Elevated (120 to 129) | 12 (5.2%) | | | | | |
Stage I (130 to 139) | 19 (8.2%) | | | | | |
Stage II (>140) | 26 (11.3%) | | | | | |
Hypotensive (<90) | 43 (18.6%) | | | | | |
Diastolic blood pressure, mmHg (N=231) | | 71 | 14 | 70 | 60 | 80 |
Normal (< 80) | 147 (63.63%) | | | | | |
Stage I (80 to 89) | 12 (5.63%) | | | | | |
Stage II (≥ 90) | 34 (14.71%) | | | | | |
Hypotensive (<60) | 38 (16.45%) | | | | | |
Pulse rate (beats/minute) (N=231) | | 105 | 48 | 100 | 88 | 113 |
Normal | 127 (55.0%) | | | | | |
Less than 60 bpm | 2 (0.90%) | | | | | |
Above 100 bpm | 102 (44.2%) | | | | | |
Urine output (L/24hr) (N=201) | | 2.1 | 1.03 | 2 | 1 | 3 |
Length of hospital stay | | 12 | 8 | 7 | 5 | 12 |
Readmission within? | | | | | | |
Yes | 73 (31.6%) | | | | | |
No | 158 (68.4%) | | | | | |
Key: SD = standard deviation; Q1. = 25th percentile, Q3 = 75th percentile
Orthopnea and paroxysmal nocturnal dyspnea were the two common major Framingham criteria at admission accounting for 63.2% and 61.5% respectively.
Table 4. Framingham major criteria and minor of acute heart failure patients admitted to Asella referral and teaching hospital, Asella 2024 (n=231).
Framingham criteria | Frequency (%) |
Major criteria | |
Orthopnea | 146 (63.2%) |
Paroxysmal nocturnal dyspnea | 142 (61.47%) |
Rales | 112 (48.48%) |
Acute pulmonary edema | 72 (31.17%) |
Neck vein distension | 47 (20.35%) |
Cardiomegaly | 39 (16.88%) |
S3 gallop | 8 (3.46%) |
Minor criteria | |
Dyspnea on ordinary exertion | 204 (83.1%) |
Nocturnal cough | 186 (80.5%) |
Bilateral ankle edema | 153 (66.2%) |
Hepatomegaly | 67 (29.0%) |
Tachycardia (heart rate>120 beats/min) | 31 (13.4%) |
Pleural effusion | 26 (11.3%) |
Serum electrolyte levels were done for 170 patients. Wherein 97 individuals (42%) presented with hyponatremia, while seven patients (3%) exhibited hypernatremia (>135 mEq/L). Similarly, serum potassium levels were determined for 170 patients. Among these, 78 individuals (33.8%) presented with hypokalemia, and 10 cases (4%) had hyperkalemia (>5.5 mEq/L) which was diagnosis by treating Physician.
Complete blood count (CBC) was done for all patients admitted with AHF, with 113 (48.9%) patients having hemoglobin level less than 13 mg/dl. Among these cases, 88 patients (77.9%) experienced moderate anemia, while 14 patients (12%) were diagnosed with severe anemia.
Serum creatinine levels were determined for 199 individuals, of which 87 (43.7%) diagnosed with acute kidney injury (AKI), with 17 cases (8.5%) developing AKI as a complication of treatment.
Table 5. Laboratory values of acute heart failure patients admitted to Asella referral and teaching hospital, Asella 2024.
Variables | N | Frequency (%) | Mean | SD | Median | Q1 | Q3 |
Serum sodium (mEq/L) | 170 | | 133.24 | 8.8 | 135 | 126 | 140 |
Hyponatremia (<135 mEq/L) | | 97 (42%) | | | | | |
Normal (135-145 mEq/L) | | 66 (28.6%) | | | | | |
Hypernatremia (>135 mEq/L) | | 7 (3%) | | | | | |
Serum potassium (mEq/L) | 170 | | 3.7 | 0.95 | 3.6 | 3.2 | 4.2 |
Normal | | 82 (35.5%) | | | | | |
Hypokalemia (< 3.5 mEq/L) | | 78 (33.8%) | | | | | |
Hyperkalemia (> 5.5 mEq/L) | | 10 (4%) | | | | | |
Hemoglobin (g/dL) | 231 | | 12.79 | 3.3 | 12.7 | 10.1 | 14.9 |
Mild anemia: Hb 12.0-12.9 g/dL | | 11 (9.7%) | | | | | |
Moderate anemia: Hb 8-11.9 g/dL | | 88 (77.9%) | | | | | |
Severe anemia: Hb<8.0 g/L | | 14 (12%) | | | | | |
Serum creatinine (mg/dL) | 199 | | 1.3 | 0.93 | 1 | 0.7 | 1.5 |
AKI | | 87 (43.7%) | | | | | |
Key: SD = standard deviation; Q1 = 25th percentile, Q3 = 75th percentile, AKI = acute kidney injury
Chest X-ray findings were documented for 185 patients (80.09%). The most prevalent X-ray finding was pulmonary edema, observed in 70 cases (37.8%), and followed by pneumonia in 45 instances (24.3%).
All 231 patients underwent echocardiography, revealing ischemic heart disease in 84 cases (36.36%), chronic rheumatic heart disease in 66 patients (28.57%), and cor-pulmonale in 44 instances (19.05%) as the three most prevalent findings.
Among the 231 patients, only 149 individuals had electrocardiogram. Atrial fibrillation was the predominant finding, present in 61 cases (40.9%).
Table 6. Imaging findings of acute heart failure patients admitted to Asella referral and teaching hospital, Asella 2024.
Imaging | Imaging Finding | Frequency (%) |
Chest X-ray | Pulmonary edema | 70 (37.8%) |
Pneumonia | 45 (24.3%) |
Pleural effusion | 41 (22.1%) |
Cardiomegaly | 34 (18.3%) |
Normal | 25 (13.5%) |
Fibrotic change | 12 (6.4%) |
Echocardiography (N = 231) | Ischemic heart disease | 84 (36.36%) |
Chronic rheumatic heart disease | 66 (28.57%) |
Cor-pulmonale | 42 (18.2%) |
Hypertensive heart disease | 22 (9.52%) |
Congenital heart disease | 6 (2.6%) |
Degenerative heart disease | 4 (1.73) |
Pericarditis | 5 (2.2%) |
Postpartal cardiomyopathy | 2 (0.86%) |
Ejection fraction | Preserved EF (≥ 50%) | 117 (50.6%) |
Reduced EF (≤ 40%) | 87 (37.7%) |
Mid-range EF (41 to 49%) | 27 (11.7%) |
Electrocardiogram (N = 149) | Atrial fibrillation | 61 (40.9%) |
Normal | 28 (18.8%) |
Sinus tachycardia | 20 (13.4%) |
LVH | 16 (10.7%) |
Acute coronary syndrome | 8 (5.4% |
Other | 16 (10.73%) |
Key: LVH = Left ventricular hypertrophy, other = (AV block, RBB, LBB), EF= ejection fraction
Among the various underlining cardiac diseases identified, ischemic heart disease was the most prevalent, accounting for more than three five percent (36.36%) followed by chronic rheumatic heart disease which contributed for more than one forth (28.6%) in this study. Cor-pulmonale ranked third, with 44 cases (19.05%).
The three common precipitant factors that lead to hospitalization are; pneumonia, atrial fibrillation, noncompliance with medications accounting for 84 cases (36.36%), 66 cases (28.57%), and 44 cases (19.05%) respectively.
Hypertension was the most common comorbidity identified, presented in 54 (41.2%) cases, followed by diabetes in 32 (24.4%) cases, and dyslipidemia in 25 (19%) cases.
Table 7. Precipitating factors and Co-morbidity of acute heart failure patients admitted to Asella referral and teaching hospital, Asella 2024.
| Factors / diseases | Frequency (%) |
Precipitating factors (n = 231) | Pneumonia | 57 (24.68%) |
Atrial fibrillation | 42 (18.18%) |
Noncompliance with medications | 33 (14.29%) |
Unknown | 31 (13.42%) |
Anemia | 17 (7.36%) |
Urinary tract infection | 13 (5.63%) |
Infective endocarditis | 12 (5.19%) |
Pregnancy | 8 (3.46%) |
Uncontrolled hypertension | 7 (3.03%) |
Acute coronary syndrome | 4 (1.73%) |
Co-morbidity (n = 131) | Hypertension | 54 (41.2%) |
Diabetes | 32 (24.4%) |
Dyslipidemia | 25 (19%) |
Asthma | 20 (15.2%) |
CKD | 20 (15.2%) |
Hyperthyroidism | 13 (10%) |
COPD | 16 (12.2%) |
Cerebrovascular disease | 9 (6.9%) |
HIV/AIDS | 5 (3.8%) |
Hypothyroidism | 3 (2.3%) |
ACO | 12 (9.2%) |
Key: COPD = Chronic obstructive pulmonary disease, ACO = asthma COPD overlap,
HIV/AIDS = Human Immunodeficiency Virus/Acquired Immunodeficiency Syndrome,
CKD = Chronic Kidney Disease
The management of patients with acute heart failure (AHF) involved a notable consumption of specific drug classes. The drugs with higher rates of utilization included furosemide which was prescribed in 220 patients (95.2%), followed by spironolactone in 99 cases (82.25%), statin in 77 cases (33.3%), and aspirin in 70 cases (30.3%) (
Table 8).
Table 8. Drugs used in the treatment of acute heart failure patients admitted to Asella referral and teaching hospital, Asella 2024.
Drug (pharmacologic class) | Frequency (%) |
Furosemide | 220 (95.24%) |
Spironolactone | 190 (82.25%) |
Statins | 77 (33.33%) |
Aspirin | 70 (30.3%) |
Angiotensin converting enzyme inhibitor | 51 (22.08%) |
Digoxin | 49 (21.21%) |
Beta-blocker | 43 (18.61) |
Oral anticoagulant / Warfarin | 31 (13.42%) |
Epinephrine | 24 (10.39%) |
Calcium channel blocker | 16 (6.93%) |
Amiodarone | 2 (0.87) |
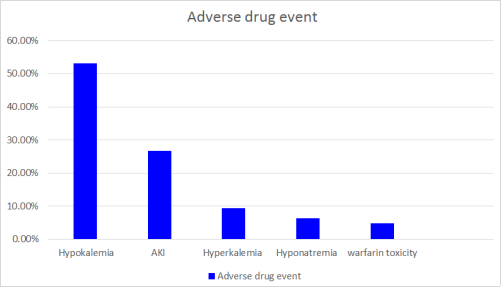
As illustrated in the
Figure 1, 64 patients (27.7%) admitted developed treatment-related adverse drug effects. Within this subset, hypokalemia was observed in 34 patients (53.1%), acute kidney injury (AKI) in 17 patients (26.6%), and hyperkalemia in 6 patients (9.3%). Notably, among those who developed warfarin toxicity, two out of the three patients had supra-therapeutic international normalized ratios (INR), while one experienced bleeding. These findings underscore the importance of vigilant monitoring for potential adverse effects associated with the pharmacological interventions used in the treatment of acute heart failure.
Figure 1. Adverse drug event among acute heart failure patients admitted to Asella referral and teaching hospital, Asella 2024.
Ninety-three patients (40.3%) required non-pharmacologic treatment, with all 93 individuals receiving intra-nasal oxygen. Moreover, 40 patients (43%) were additionally treatment with facemask, while four patients (4%) required mechanical ventilation.
3.3. Clinical Condition at Discharge
Table 9. Clinical condition at discharge of acute heart failure patients admitted to Asella referral and teaching hospital, Asella 2024.
Variable | Frequency (%) | Mean | SD | Median | Q1 | Q2 |
Systolic blood pressure, mmHg (N=160) | | 105 | 14 | 100 | 99 | 110 |
Normal | 137 (86.25%) | | | | | |
Hypotensive | 5 (3.13%) | | | | | |
Diastolic blood pressure, mmHg (N=160) | | 70 | 10 | 64 | 60 | 70 |
Normal | 135 (84.38%) | | | | | |
Hypotensive | 4 (2.50%) | | | | | |
Pulse rate (beats/minute) (N=160) | | 84 | 18 | 88 | 80 | 92 |
Normal | 127 (79.34%) | | | | | |
Above 100 bpm | 14 (8.75%) | | | | | |
The mean systolic blood pressure (SBP) was 105 ± 14 mmHg. In compare to the admission figures where 128 patients (55.41%) presenting with normal SBP, during discharge 137 patients (86.25%) had normal blood pressure. This indicates an improvement in systolic blood pressure levels for a majority of patients during the course of their hospitalization.
In comparison, at discharge, there was a significant improvement in NYHA class. With only two patients (1.25%). Additionally, at discharge, Grade I edema was observed in one patient (0.63%), and Grade II edema in two patients (1.25%). These are patients who were discharged without significant improvement, and they had stage D cardiac disease at admission. The underlying cardiac disease in these patients was identified as chronic rheumatic valvular heart disease (CRVHD).
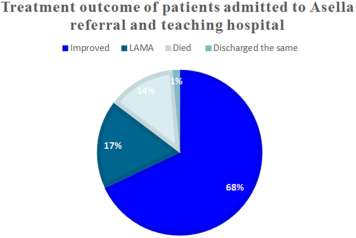
3.4. Treatment Outcome
Among the 231 admitted patients with acute heart failure, 157 (68.0%) were discharged with improvement, 40 (17.3%) left against medical advice, and 31 (13.4%) patients succumbed during their hospital stay (
Figure 3).
Figure 2. Treatment outcome of acute heart failure patients admitted to Asella referral and teaching hospital, Asella 2024.
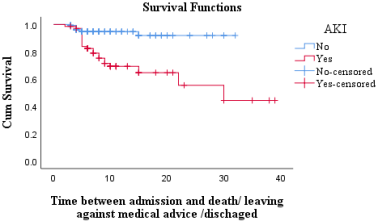
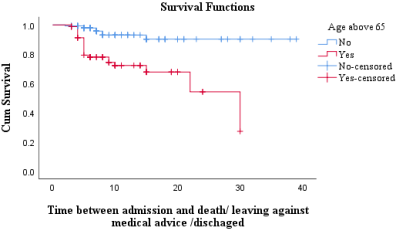
3.5. Predictors of in Hospital Outcome
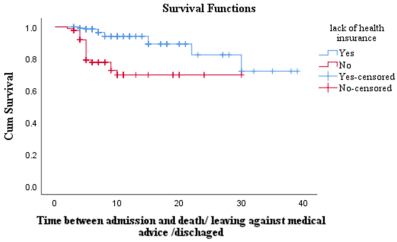
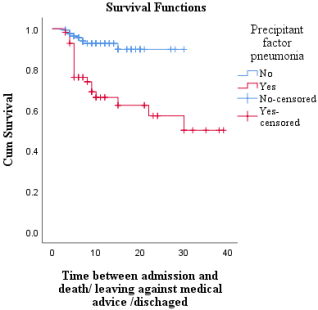
The Kaplan-Meier analysis, depicted in the
Figures 2-6, demonstrates a clear difference of survival distributions in health insurance, age, acute kidney injury (AKI), and pneumonia. The log-rank test further supports these findings, revealing a highly significant p-value of <0.001.
Proportional hazard assumption was checked using the log-minus-log curve and it does not violate the proportional assumption. The survival analysis has yielded insightful observations, emphasizing the impact of various factors on in-hospital outcomes. Pneumonia is identified as a substantial contributor, with a hazard ratio of 3.07 (95% CI: 1.40, 6.74, p = 0.005), indicating a significantly heightened risk. Similarly, acute kidney injury demonstrates a hazard ratio of 2.98 (95% CI: 1.31, 6.75, p = 0.009). Lack of health insurance also emerges as a noteworthy predictor, with a hazard ratio of 3.46 (95% CI: 1.51, 7.95, p = 0.003). Additionally, age greater than 65, is identified as a predictor factor, revealing a hazard ratio of 2.81 (95% CI: 1.18, 6.72, p = 0.020).
Figure 3. Kaplan-Meier of Acute kidney injury among acute heart failure patients admitted to Asella referral and teaching hospital, Asella 2024.
Figure 4. Kaplan-Meier of Age among acute heart failure patients admitted to Asella referral and teaching hospital, Asella 2024.
Figure 5. Kaplan-Meier of health insurance among acute heart failure patients admitted to Asella referral and teaching hospital, Asella 2024.
Table 10. Predictors of in hospital outcome among acute heart failure patients admitted to Asella referral and teaching hospital, Asella 2024.
Variables | Frequency (%) | Hazard ratio | 95% CI | P value |
Precipitant factor pneumonia | | | | |
Yes | 57 (24.7%) | 3.073 | 1.40, 6.74 | 0.005 |
No | 174 (75.3%) | | | |
Acute kidney injury | | | | |
Yes | 70 (30.3%) | 2.975 | 1.31, 6.75 | 0.009 |
No | 161 (69.7%) | | | |
Active health insurance | | | | |
No | 89 (38.5%) | 3.461 | 1.51, 7.95 | 0.003 |
Yes | 142 (61.5%) | | | |
Age | | | | |
≥ 65 | 83 (35.9%) | 2.814 | 1.18, 6.72 | 0.020 |
< 65 | 148 (64.1%) | | | |
Figure 6. Kaplan-Meier of precipitant factor pneumonia among acute heart failure patients admitted to Asella referral and teaching hospital, Asella 2024.
4. Discussion
Over half of the patients with acute heart failure (AHF) in this study were female, constituting 54.4% of the cohort. This female predominance is comparable to findings in other studies, such as the Acute Decompensated Heart Failure Registry (ADHERE) (52.0%) and the Organized Program to Initiate Lifesaving Treatment in Hospitalized Patients with Heart Failure (OPTIMIZE-HF) (52.0%). Notably, similar gender distribution patterns have been observed in study from Tikur Anbessa Specialized (54.4%) and Jimma (53.3%)
| [26] | Adams KF, Fonarow GC, Emerman CL, LeJemtel TH, Costanzo MR, Abraham WT, et al. Characteristics and outcomes of patients hospitalized for heart failure in the United States: Rationale, design, and preliminary observations from the first 100,000 cases in the Acute Decompensated Heart Failure National Registry (ADHERE). Am Heart J. 2005; 149(2): 209-16. |
| [41] | Dokainish H, Teo K, Zhu J, Roy A, Alhabib KF, Elsayed A, et al. Articles Global mortality variations in patients with heart failure : results from the International Congestive Heart Failure (INTER-CHF) prospective cohort study. 2017; 665-72. |
| [27] | O’Connor CM, Abraham WT, Albert NM, Clare R, Gattis Stough W, Gheorghiade M, et al. Predictors of mortality after discharge in patients hospitalized with heart failure: An analysis from the Organized Program to Initiate Lifesaving Treatment in Hospitalized Patients with Heart Failure (OPTIMIZE-HF). Am Heart J. 2008; 156(4): 662-73. |
| [50] | Mekonin G, Dukessa T, Dube L, Tadesse I. Acute heart failure outcome and predictors of outcome among patients admitted to Jimma University Medical Center, Southwest Ethiopia. 2022; |
[26, 41, 27, 50]
.
Regarding age, this study reveals that acute heart failure (AHF) predominantly affects relatively younger patients with a median age of 56. A similar trend to this study was observed in The Sub-Saharan Africa Survey of Heart Failure (THESUS-HF), which reported a median age of 55 years
| [6] | Damasceno A, Mayosi BM, Sani M, Ogah OS, Mondo C, Ojji D, et al. The causes, treatment, and outcome of acute heart failure in 1006 Africans from 9 countries: Results of the sub-Saharan Africa survey of heart failure. Arch Intern Med. 2012; 172(18): 1386-94. |
[6]
. This differs from developed countries where it is characterized as a disease of elderly, typically presenting with a mean age of 72 years (median age, 66-70)
| [26] | Adams KF, Fonarow GC, Emerman CL, LeJemtel TH, Costanzo MR, Abraham WT, et al. Characteristics and outcomes of patients hospitalized for heart failure in the United States: Rationale, design, and preliminary observations from the first 100,000 cases in the Acute Decompensated Heart Failure National Registry (ADHERE). Am Heart J. 2005; 149(2): 209-16. |
| [27] | O’Connor CM, Abraham WT, Albert NM, Clare R, Gattis Stough W, Gheorghiade M, et al. Predictors of mortality after discharge in patients hospitalized with heart failure: An analysis from the Organized Program to Initiate Lifesaving Treatment in Hospitalized Patients with Heart Failure (OPTIMIZE-HF). Am Heart J. 2008; 156(4): 662-73. |
| [28] | Chioncel O, Mebazaa A, Harjola VP, Coats AJ, Piepoli MF, Crespo-Leiro MG, et al. Clinical phenotypes and outcome of patients hospitalized for acute heart failure: the ESC Heart Failure Long-Term Registry. Eur J Heart Fail. 2017; 19(10): 1242-54. |
[26-28]
.
The majority of patients presented with worsening of preexisting chronic heart failure (61.9%), with a notable proportion having de novo heart failure (38.1%). NYHA class IV was predominant at admission (81.0%), highlighting the severity of cases. A comparative study from Tikur Anbessa Specialized Hospital reported NYHA IV, III, and II at rates of 69.2%, 24.3%, and 6.5%, respectively
| [16] | Tirfe M, Nedi T MD. Treatment outcome and associated factors in acute heart failure patients at Tikur Anbessa Specialized Hospital, Addis Ababa, Ethiopia. BMC Cardiovasc Disord. 2018; 20(1): 1-10. |
[16]
. This disparity may be attributed to the higher representation of patients from rural areas in this study (72.4%), potentially contributing to delays in presentation with severe symptoms.
The hemodynamic profiles indicated that a considerable number of patients presented with a warm and wet profile (64.5%), followed by warm dry (27.7%). A study from Tikur Anbessa Specialized Hospital reported a similar pattern, with warm wet being the most common, followed by warm dry
| [16] | Tirfe M, Nedi T MD. Treatment outcome and associated factors in acute heart failure patients at Tikur Anbessa Specialized Hospital, Addis Ababa, Ethiopia. BMC Cardiovasc Disord. 2018; 20(1): 1-10. |
[16]
. The BREATHE registry also indicated warm wet as the predominant hemodynamic profile
| [32] | Rockstroh K, Thienemann F, Sliwa K. Clinical update HIV and the heart : the impact of antiretroviral therapy : a global perspective. 2013; 3538-46. |
| [39] | de Albuquerque DC, Neto JD de S, Bacal F, Rohde LEP, Bernardez-Pereira S, Berwanger O, et al. I Brazilian registry of heart failure - Clinical aspects, care quality and hospitalization outcomes. Arq Bras Cardiol. 2015; 104(6): 433-42. |
[32, 39]
.
The study showed that the most prevalent symptoms of Framingham major criteria were Orthopnea, paroxysmal nocturnal dyspnea and rales. These findings are consistent with observations from the ALARM-HF registry, where orthopnea and rales emerged as the most common presenting symptoms
| [29] | Follath F, Yilmaz MB, Delgado JF, Parissis JT, Porcher R, Gayat E, et al. Clinical presentation, management and outcomes in the Acute Heart Failure Global Survey of Standard Treatment (ALARM-HF). Intensive Care Med. 2011; 37(4): 619-26. |
[29]
.
In the present study, the principal precipitating factors identified included pneumonia, atrial fibrillation, and drug discontinuation. Similar patterns were observed in the BREATHE registry, where infection and poor medication adherence were prominent factors. These findings are also in concordance with the observations reported in the OPTIMIZE-HF registry, which highlighted pneumonia, arrhythmia and acute coronary syndrome, as the predominant precipitating factors
| [27] | O’Connor CM, Abraham WT, Albert NM, Clare R, Gattis Stough W, Gheorghiade M, et al. Predictors of mortality after discharge in patients hospitalized with heart failure: An analysis from the Organized Program to Initiate Lifesaving Treatment in Hospitalized Patients with Heart Failure (OPTIMIZE-HF). Am Heart J. 2008; 156(4): 662-73. |
| [38] | Sato N, Kajimoto K, Keida T, Mizuno M, Minami Y, Yumino D, et al. Clinical Features and Outcome in Hospitalized Heart Failure in Japan (From the ATTEND Registry). 2013; 77(April): 944-51. |
| [33] | Keates AK, Mocumbi AO, Ntsekhe M, Sliwa K, Stewart S. Cardiovascular disease in Africa: Epidemiological profile and challenges. Nat Rev Cardiol. 2017; 14(5): 273-93. |
| [29] | Follath F, Yilmaz MB, Delgado JF, Parissis JT, Porcher R, Gayat E, et al. Clinical presentation, management and outcomes in the Acute Heart Failure Global Survey of Standard Treatment (ALARM-HF). Intensive Care Med. 2011; 37(4): 619-26. |
[27, 38, 33, 29]
. However, it is noteworthy that acute coronary syndrome (ACS) was less frequently identified as a precipitating factor in our study. This could be due to several factors, including restricted access to diagnostic resources such as electrocardiograms (ECGs) and cardiac biomarkers, as well as a lack of awareness regarding the clinical presentation of acute coronary syndrome (ACS) within the community. Evidence supporting this notion comes from a study conducted in both private and public hospitals of Addis Ababa, revealing that half of the patients lacked sufficient knowledge regarding acute coronary syndrome (ACS) even after receiving treatment for the condition
| [43] | Miró Ò, García Sarasola A, Fuenzalida C, Calderón S, Jacob J, Aguirre A, et al. Departments involved during the first episode of acute heart failure and subsequent emergency department revisits and rehospitalisations: an outlook through the NOVICA cohort. Eur J Heart Fail. 2019; 21(10): 1231-44. |
| [51] | Demisse L, Alemayehu B, Addissie A, Azazh A, Gary R. Knowledge, attitudes and beliefs about acute coronary syndrome among patients diagnosed with acute coronary syndrome, Addis Ababa, Ethiopia. BMC Cardiovasc Disord. 2022; 22(1): 1-9. Available from: https://doi.org/10.1186/s12872-022-02893-2 |
[43, 51]
.
The findings suggest that implementing pneumonia vaccination programs, focusing on educating and counseling patients about cardiac drug compliance, along with optimizing the management of atrial fibrillation, might contribute to a decrease in admissions for acute heart failure.
Heart failure with reduced ejection fraction (EF) is commonly recognized as the predominant type, consistent with findings from studies conducted at Tikur Anbessa Specialized Hospital and the BREATHE registry
| [35] | Baldi I, Azzolina D, Berchialla P, Gregori D, Corrao G. Comorbidity-adjusted relative survival in newly hospitalized heart failure patients: a population-based study. Int J Cardiol. 2017; Available from: http://dx.doi.org/10.1016/j.ijcard.2017.05.080 |
| [16] | Tirfe M, Nedi T MD. Treatment outcome and associated factors in acute heart failure patients at Tikur Anbessa Specialized Hospital, Addis Ababa, Ethiopia. BMC Cardiovasc Disord. 2018; 20(1): 1-10. |
| [19] | Talle MA, Bonny A, Scholtz W, Chin A, Nel G, Karaye KM, et al. Status of cardiac arrhythmia services in Africa in 2018: A PAsCAr sudden Cardiac death task Force report. Cardiovasc J Afr. 2018; 29(2): 115-21. |
[35, 16, 19]
.
In terms of underlying etiology, the study revealed that ischemic heart disease is the leading cause (36.36%), followed by chronic rheumatic heart disease and cor-pulmonale. These findings closely parallel data from the OPTIMIZE-HF registry, as well as observations from the BREATHE registry and studies conducted in Djibouti and Jimma.
| [21] | Fourcade L, Massoure PL, Roche NC, Lamblin G, Topin F, Dehan C. la perspective d ’ une transition épidémiologique Heart failure patterns in Djibouti : epidemiologic transition. 2013; 211-6. |
| [27] | O’Connor CM, Abraham WT, Albert NM, Clare R, Gattis Stough W, Gheorghiade M, et al. Predictors of mortality after discharge in patients hospitalized with heart failure: An analysis from the Organized Program to Initiate Lifesaving Treatment in Hospitalized Patients with Heart Failure (OPTIMIZE-HF). Am Heart J. 2008; 156(4): 662-73. |
| [39] | de Albuquerque DC, Neto JD de S, Bacal F, Rohde LEP, Bernardez-Pereira S, Berwanger O, et al. I Brazilian registry of heart failure - Clinical aspects, care quality and hospitalization outcomes. Arq Bras Cardiol. 2015; 104(6): 433-42. |
| [50] | Mekonin G, Dukessa T, Dube L, Tadesse I. Acute heart failure outcome and predictors of outcome among patients admitted to Jimma University Medical Center, Southwest Ethiopia. 2022; |
[21, 27, 39, 50]
. However, the THESUS-HF registry reported predominantly non-ischemic etiology, with hypertension and rheumatic heart disease being the most common causes
| [6] | Damasceno A, Mayosi BM, Sani M, Ogah OS, Mondo C, Ojji D, et al. The causes, treatment, and outcome of acute heart failure in 1006 Africans from 9 countries: Results of the sub-Saharan Africa survey of heart failure. Arch Intern Med. 2012; 172(18): 1386-94. |
[6]
. This difference can be attributed to the fact that the THESUS-HF registry was conducted a decade ago, and the predominance of ischemic heart disease in the recent study reflects epidemiological transition, as noted in a study on the Epidemiology of Cardiovascular Diseases in Morocco. In this study, an increasingly heavy burden of cardiovascular risk factors such as diabetes, hypertension, dyslipidemia, and smoking was observed
| [37] | Nieminen MS, Brutsaert D, Dickstein K, Drexler H, Follath F, Harjola VP, et al. EuroHeart Failure Survey II (EHFS II): A survey on hospitalized acute heart failure patients: Description of population. Eur Heart J. 2006; 27(22): 2725-36. |
| [11] | Elyamani R, Soulaymani A, Hami H. Epidemiology of Cardiovascular Diseases in Morocco: A Systematic Review. Rev Diabet Stud. 2021; 17(2): 57-67. |
[37, 11]
.
Hypertension, diabetes mellitus, and dyslipidemia emerged as the three most common comorbidities identified in this research. A study conducted in Jimma reported similar findings
| [50] | Mekonin G, Dukessa T, Dube L, Tadesse I. Acute heart failure outcome and predictors of outcome among patients admitted to Jimma University Medical Center, Southwest Ethiopia. 2022; |
[50]
. Likewise, in the KorAHF registry, major comorbidities included hypertension, diabetes, cerebrovascular illness, chronic renal failure, and chronic lung disease
| [44] | Butt JH, Fosbøl EL, Gerds TA, Andersson C, McMurray JJV, Petrie MC, et al. Readmission and death in patients admitted with new-onset versus worsening of chronic heart failure: insights from a nationwide cohort. Eur J Heart Fail. 2020; 22(10): 1777-85. |
| [40] | Lee SE, Lee HY, Cho HJ, Choe WS, Kim H, Choi JO, et al. Clinical characteristics & outcome of acute heart failure in Korea: Results from the Korean acute heart failure registry (KorAHF). Korean Circ J. 2017; 47(3): 341-53. |
[44, 40]
. The impact of comorbidities on underlying cardiac disease was evident in this study, as approximately 44% of patients with ischemic heart disease had one or more comorbidities, whereas only 21% of patients with right-sided heart failure exhibited comorbidities. This underscores the significant influence of comorbidities on underlying cardiac conditions.
The in-hospital mortality rate was 13.4%, with a higher mortality rate observed in patients experiencing worsening of preexisting heart failure (61%) compared to those with de novo heart failure (39%). The overall in-hospital mortality in this study was comparatively lower than that reported in the Jimma study (20.1%) and a prospective study conducted in Uganda (18.3%)
| [22] | Boombhi J, Moampea M, Kuate L, Menanga A, Hamadou B, Kingue S. Clinical Pattern and Outcome of Acute Heart Failure at the Yaounde Central Hospital. OALib. 2017; 04(03): 1-8. |
| [34] | Conrad N, Judge A, Tran J, Mohseni H, Hedgecott D, Crespillo AP, et al. Temporal trends and patterns in heart failure incidence: a population-based study of 4 million individuals. Lancet. 2018; 391(10120): 572-80. Available from: http://dx.doi.org/10.1016/S0140-6736(17)32520-5 |
| [50] | Mekonin G, Dukessa T, Dube L, Tadesse I. Acute heart failure outcome and predictors of outcome among patients admitted to Jimma University Medical Center, Southwest Ethiopia. 2022; |
[22, 34, 50]
. This discrepancy may be attributed to methodological differences, as the outcome for 19 patients in this study was unknown. Moreover, the lower mortality rate could also be linked to improvements in health insurance coverage, aligning with findings from INTER-CHF, which identified lower healthcare insurance rates as contributing factors to increase in-hospital mortality
| [8] | Dokainish H, Teo K, Zhu J, Roy A, Alhabib KF, Elsayed A, et al. Heart Failure in Africa, Asia, the Middle East and South America: The INTER-CHF study. Int J Cardiol. 2016; 204: 133-41. Available from: http://dx.doi.org/10.1016/j.ijcard.2015.11.183 |
[8]
. Additionally, lack of health insurance coverage was identified as a predictor for poor in-hospital outcomes in this study.
However, the in-hospital mortality rate among patients admitted to Asella Referral Hospital remains relatively high compared to other registries such as KorAHF, OPTIMIZE-HF, and the ESC Heart Failure Long-Term Registry, where rates ranged from 4-6.7%
| [27] | O’Connor CM, Abraham WT, Albert NM, Clare R, Gattis Stough W, Gheorghiade M, et al. Predictors of mortality after discharge in patients hospitalized with heart failure: An analysis from the Organized Program to Initiate Lifesaving Treatment in Hospitalized Patients with Heart Failure (OPTIMIZE-HF). Am Heart J. 2008; 156(4): 662-73. |
| [28] | Chioncel O, Mebazaa A, Harjola VP, Coats AJ, Piepoli MF, Crespo-Leiro MG, et al. Clinical phenotypes and outcome of patients hospitalized for acute heart failure: the ESC Heart Failure Long-Term Registry. Eur J Heart Fail. 2017; 19(10): 1242-54. |
| [40] | Lee SE, Lee HY, Cho HJ, Choe WS, Kim H, Choi JO, et al. Clinical characteristics & outcome of acute heart failure in Korea: Results from the Korean acute heart failure registry (KorAHF). Korean Circ J. 2017; 47(3): 341-53. |
[27, 28, 40]
. As noted in a Meta-Analysis on Heart Failure Care in Low- and Middle-Income Countries, this could be attributed to additional factors contributing to poor outcomes, including health-care infrastructure, quality of care, and variations in health-care access that may have contributed to higher mortality in our study
| [42] | Callender T, Woodward M, Roth G, Farzadfar F, Lemarie JC, Gicquel S, et al. Heart failure care in low- and middle-income countries: A systematic review and meta-analysis. PLoS Med. 2015; 11(8). |
[42]
.
The independent predictors of in-hospital mortality identified in this study included pneumonia, acute kidney injury, lack of active health insurance coverage, and age above 65.
In alignment with these findings, the ADHERE registry reported that measurements of blood urea nitrogen (BUN), followed by systolic blood pressure (SBP) and serum creatinine at admission, were highly predictive of in-hospital mortality in patients with acute decompensated heart failure (ADHF)
| [36] | Deursen VM Van, Urso R, Laroche C, Damman K, Dahlström U, Tavazzi L, et al. Co-morbidities in patients with heart failure : an analysis of the European Heart Failure Pilot Survey. |
| [26] | Adams KF, Fonarow GC, Emerman CL, LeJemtel TH, Costanzo MR, Abraham WT, et al. Characteristics and outcomes of patients hospitalized for heart failure in the United States: Rationale, design, and preliminary observations from the first 100,000 cases in the Acute Decompensated Heart Failure National Registry (ADHERE). Am Heart J. 2005; 149(2): 209-16. |
[36, 26]
. Similarly, the OPTIMIZE-HF registry highlighted advanced age as predictors of in-hospital outcomes
| [27] | O’Connor CM, Abraham WT, Albert NM, Clare R, Gattis Stough W, Gheorghiade M, et al. Predictors of mortality after discharge in patients hospitalized with heart failure: An analysis from the Organized Program to Initiate Lifesaving Treatment in Hospitalized Patients with Heart Failure (OPTIMIZE-HF). Am Heart J. 2008; 156(4): 662-73. |
[27]
. These consistent observations underscore the importance of these factors in assessing and predicting mortality risk in acute heart failure patients across different studies and registries.
5. Limitation of the Study
The present study has several limitations that should be noted. Measurements of biomarkers such as B-type natriuretic peptide (BNP) and N-terminal pro-B-type natriuretic peptide (NT-pro-BNP) were not available, and these biomarkers could have provided important insights into predicting the outcome of acute heart failure (AHF). Additionally, ECG and measurements of laboratory values, including cardiac troponin, renal function tests, and serum electrolytes, were not consistently available for all patients, and the absence of these data could affect the analysis and interpretation of outcomes.
Moreover, it is important to acknowledge that the study is retrospective in nature, which may introduce inherent limitations.
6. Conclusion and Recommendation
6.1. Conclusion
In summary, the study revealed a predominant representation of relatively young female patients experiencing acute decompensated heart failure (ADHF). Unfortunately, when compared to developed countries, the study's results indicate a high in-hospital mortality rate for acute heart failure. The identified independent predictors of in-hospital mortality are pneumonia, acute kidney injury, lack of active health insurance coverage and age above 65. The principal precipitating factors leading to hospitalization were pneumonia and ischemic heart disease was identified as the most common underlying cardiac disease.
6.2. Recommendation
To ARTH administration: Improve Consistency and availability of essential investigation such as electrocardiograms (ECG) and laboratory values like cardiac troponin, renal function tests, and serum electrolytes for all patients to improve quality of care. Tailored Interventions for Precipitating Factors: Design interventions addressing principal precipitating factors—pneumonia, atrial fibrillation, and drug discontinuation—through strategies for early detection, management and patient education.
Abbreviations
ACC/AHA | American College of Cardiology / American Heart Association |
ACE | Angiotensin Converting Enzyme |
ACS | Acute Coronary Syndrome |
ADHERE | Acute Decompensated Heart Failure National Registry |
ADHF | Acute Decompensated Heart Failure |
ADR/SE | Adverse Drug Event / Side Effect |
AF | Atrial Fibrillation |
AHF | Acute Heart Failure |
ALARM-HF | Acute Heart Failure Global Registry of Standard Treatment |
ATRH | Asella Teaching and Referral Hospital |
BNP | B-Type Natriuretic Peptide |
BUN | Blood Urea Nitrogen |
CAD | Coronary Artery Disease |
CHD | Congenital Heart Disease |
CKD | Chronic Kidney Disease |
COPD | Chronic Obstructive Pulmonary Disease |
CS | Cardiogenic Shock |
Author Contributions
Dawit Abdi: Conceptualization, Data curation, Formal Analysis, Methodology, Software, Validation, Visualization, Writing - original draft, Writing - review & editing
Rudwan Yasin Abrahim: Conceptualization, Formal Analysis, Investigation, Methodology, Software, Validation, Visualization, Writing - original draft, Writing - review & editing
Olifan Getachew: Conceptualization, Data curation, Formal Analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing - original draft, Writing - review & editing
Bethelhem Fekadeselassie Lemma: Data curation, Formal Analysis, Methodology, Software, Supervision, Validation, Visualization, Writing - original draft, Writing - review & editing
Kidist Mehari Azene: Conceptualization, Data curation, Formal Analysis, Methodology, Software, Supervision, Validation, Visualization, Writing - original draft, Writing - review & editing
Peniel Yigezu Sedi: Conceptualization, Data curation, Formal Analysis, Methodology, Software, Supervision, Validation, Visualization, Writing - original draft, Writing - review & editing
Conflicts of Interest
The authors declare no conflicts of interest.
References
| [1] |
McDonagh TA, Metra M, Adamo M, Gardner RS, Baumbach A, Böhm M, et al. 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur Heart J. 2021; 42(36): 3599-726.
|
| [2] |
Campos-Arjona R, García-Pinilla JM, de Teresa-Galván E. Acute heart failure. Med. 2019; 12(89): 5237-44.
|
| [3] |
Ural D, Çavuşoğlu Y, Eren M, Karaüzüm K, Temizhan A, Yılmaz MB, et al. Akut kalp yetersizliği tanı ve tedavisi. Anatol J Cardiol. 2015; 15(11): 860-89.
|
| [4] |
Heidenreich PA, Bozkurt B, Aguilar D, Allen LA, Byun JJ, Colvin MM, et al. 2022 AHA/ACC/HFSA Guideline for the Management of Heart Failure: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Vol. 145, Circulation. 2022. 895-1032 p.
|
| [5] |
Gallagher J, McDonald K, Ledwidge M, Watson CJ. Heart Failure in Sub-Saharan Africa. Card Fail Rev. 2018; 4(1): 1.
|
| [6] |
Damasceno A, Mayosi BM, Sani M, Ogah OS, Mondo C, Ojji D, et al. The causes, treatment, and outcome of acute heart failure in 1006 Africans from 9 countries: Results of the sub-Saharan Africa survey of heart failure. Arch Intern Med. 2012; 172(18): 1386-94.
|
| [7] |
Gtif I, Bouzid F, Charfeddine S, Abid L, Kharrat N. Heart failure disease: An African perspective. Arch Cardiovasc Dis. 2021; 114(10): 680-90.
|
| [8] |
Dokainish H, Teo K, Zhu J, Roy A, Alhabib KF, Elsayed A, et al. Heart Failure in Africa, Asia, the Middle East and South America: The INTER-CHF study. Int J Cardiol. 2016; 204: 133-41. Available from:
http://dx.doi.org/10.1016/j.ijcard.2015.11.183
|
| [9] |
S. Ogah O, Adebiyi A, Sliwa K. Heart Failure in Sub-Saharan Africa. Top Hear Fail Manag. 2019.
|
| [10] |
Olatayo Adeoti A, Adekunle Ajayi E, Oladimeji Ajayi A, Ayokunle Dada S, Olusesan Fadare J, Akolawole M, et al. Pattern and Outcome of Medical Admissions in Ekiti State University Teaching Hospital, Ado-Ekiti-A 5 Year Review. Am J Med Med Sci. 2015; 2015(2): 92-8. Available from:
http://journal.sapub.org/ajmms
|
| [11] |
Elyamani R, Soulaymani A, Hami H. Epidemiology of Cardiovascular Diseases in Morocco: A Systematic Review. Rev Diabet Stud. 2021; 17(2): 57-67.
|
| [12] |
Ogah OS, Stewart S, Falase AO, Akinyemi JO, Adegbite GD, Alabi AA, et al. Contemporary profile of acute heart failure in Southern Nigeria: Data from the abeokuta heart failure clinical registry. JACC Hear Fail. 2014; 2(3): 250-9.
|
| [13] |
Makubi A, Hage C, Lwakatare J, Kisenge P, Makani J, Rydén L, et al. Contemporary aetiology, clinical characteristics and prognosis of adults with heart failure observed in a tertiary hospital in Tanzania: The prospective Tanzania Heart Failure (TaHeF) study. Heart. 2014; 100(16): 1235-41.
|
| [14] |
Okello S, Rogers O, Byamugisha A, Rwebembera J, Buda AJ. Characteristics of acute heart failure hospitalizations in a general medical ward in Southwestern Uganda. Int J Cardiol. 2014; 176(3): 1233-4. Available from:
http://dx.doi.org/10.1016/j.ijcard.2014.07.212
|
| [15] |
Tirfe M, Nedi T, Mekonnen D, Berha AB. Treatment outcome and its predictors among patients of acute heart failure at a tertiary care hospital in Ethiopia: a prospective observational study. BMC Cardiovasc Disord. 2020; 20(1): 16. Available from:
https://doi.org/10.1186/s12872-019-01318-x
|
| [16] |
Tirfe M, Nedi T MD. Treatment outcome and associated factors in acute heart failure patients at Tikur Anbessa Specialized Hospital, Addis Ababa, Ethiopia. BMC Cardiovasc Disord. 2018; 20(1): 1-10.
|
| [17] |
Mwita JC, Dewhurst MJ, Magafu MGMD, Goepamang M, Omech B, Majuta KL, et al. Presentation and mortality of patients hospitalised with acute heart failure in Botswana. Cardiovasc J Afr. 2017; 28(2): 112-7.
|
| [18] |
Carlson S, Duber HC, Achan J, Ikilezi G, Mokdad AH, Stergachis A, et al. Capacity for diagnosis and treatment of heart failure in sub-Saharan Africa. Heart. 2017; 103(23): 1874-9.
|
| [19] |
Talle MA, Bonny A, Scholtz W, Chin A, Nel G, Karaye KM, et al. Status of cardiac arrhythmia services in Africa in 2018: A PAsCAr sudden Cardiac death task Force report. Cardiovasc J Afr. 2018; 29(2): 115-21.
|
| [20] |
Bukhman AK, Nsengimana VJP, Lipsitz MC, Henwood PC, Tefera E, Rouhani SA, et al. Diagnosis and Management of Acute Heart Failure in Sub-Saharan Africa. Curr Cardiol Rep. 2019; 21(10).
|
| [21] |
Fourcade L, Massoure PL, Roche NC, Lamblin G, Topin F, Dehan C. la perspective d ’ une transition épidémiologique Heart failure patterns in Djibouti : epidemiologic transition. 2013; 211-6.
|
| [22] |
Boombhi J, Moampea M, Kuate L, Menanga A, Hamadou B, Kingue S. Clinical Pattern and Outcome of Acute Heart Failure at the Yaounde Central Hospital. OALib. 2017; 04(03): 1-8.
|
| [23] |
Tigabe M, Fentahun A, Getawa S, Gelaye KA, Gebreyohannes EA. Clinical Characteristics and In-Hospital Outcome of Acute Heart Failure Patients Admitted to the Medical Ward of University of Gondar Comprehensive Specialized Hospital, Northwest Ethiopia. Vasc Health Risk Manag. 2021; 17: 581-90. Available from:
https://www.tandfonline.com/doi/abs/10.2147/VHRM.S322493
|
| [24] |
James SL, Abate D, Abate KH, Abay SM, Abbafati C, Abbasi N, et al. Global, regional, and national incidence, prevalence, and years lived with disability for 354 Diseases and Injuries for 195 countries and territories, 1990-2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet. 2018; 392(10159): 1789-858.
|
| [25] |
Groenewegen A, Rutten FH, Mosterd A, Hoes AW. Epidemiology of heart failure Measuring an epidemic. 2020; 7-9.
|
| [26] |
Adams KF, Fonarow GC, Emerman CL, LeJemtel TH, Costanzo MR, Abraham WT, et al. Characteristics and outcomes of patients hospitalized for heart failure in the United States: Rationale, design, and preliminary observations from the first 100,000 cases in the Acute Decompensated Heart Failure National Registry (ADHERE). Am Heart J. 2005; 149(2): 209-16.
|
| [27] |
O’Connor CM, Abraham WT, Albert NM, Clare R, Gattis Stough W, Gheorghiade M, et al. Predictors of mortality after discharge in patients hospitalized with heart failure: An analysis from the Organized Program to Initiate Lifesaving Treatment in Hospitalized Patients with Heart Failure (OPTIMIZE-HF). Am Heart J. 2008; 156(4): 662-73.
|
| [28] |
Chioncel O, Mebazaa A, Harjola VP, Coats AJ, Piepoli MF, Crespo-Leiro MG, et al. Clinical phenotypes and outcome of patients hospitalized for acute heart failure: the ESC Heart Failure Long-Term Registry. Eur J Heart Fail. 2017; 19(10): 1242-54.
|
| [29] |
Follath F, Yilmaz MB, Delgado JF, Parissis JT, Porcher R, Gayat E, et al. Clinical presentation, management and outcomes in the Acute Heart Failure Global Survey of Standard Treatment (ALARM-HF). Intensive Care Med. 2011; 37(4): 619-26.
|
| [30] |
Kurmani S, Squire I. Acute Heart Failure: Definition, Classification and Epidemiology. Curr Heart Fail Rep. 2017; 14(5): 385-92.
|
| [31] |
Bocchi EA. Heart Failure in South America. 2013; 147-56.
|
| [32] |
Rockstroh K, Thienemann F, Sliwa K. Clinical update HIV and the heart : the impact of antiretroviral therapy : a global perspective. 2013; 3538-46.
|
| [33] |
Keates AK, Mocumbi AO, Ntsekhe M, Sliwa K, Stewart S. Cardiovascular disease in Africa: Epidemiological profile and challenges. Nat Rev Cardiol. 2017; 14(5): 273-93.
|
| [34] |
Conrad N, Judge A, Tran J, Mohseni H, Hedgecott D, Crespillo AP, et al. Temporal trends and patterns in heart failure incidence: a population-based study of 4 million individuals. Lancet. 2018; 391(10120): 572-80. Available from:
http://dx.doi.org/10.1016/S0140-6736(17)32520-5
|
| [35] |
Baldi I, Azzolina D, Berchialla P, Gregori D, Corrao G. Comorbidity-adjusted relative survival in newly hospitalized heart failure patients: a population-based study. Int J Cardiol. 2017; Available from:
http://dx.doi.org/10.1016/j.ijcard.2017.05.080
|
| [36] |
Deursen VM Van, Urso R, Laroche C, Damman K, Dahlström U, Tavazzi L, et al. Co-morbidities in patients with heart failure : an analysis of the European Heart Failure Pilot Survey.
|
| [37] |
Nieminen MS, Brutsaert D, Dickstein K, Drexler H, Follath F, Harjola VP, et al. EuroHeart Failure Survey II (EHFS II): A survey on hospitalized acute heart failure patients: Description of population. Eur Heart J. 2006; 27(22): 2725-36.
|
| [38] |
Sato N, Kajimoto K, Keida T, Mizuno M, Minami Y, Yumino D, et al. Clinical Features and Outcome in Hospitalized Heart Failure in Japan (From the ATTEND Registry). 2013; 77(April): 944-51.
|
| [39] |
de Albuquerque DC, Neto JD de S, Bacal F, Rohde LEP, Bernardez-Pereira S, Berwanger O, et al. I Brazilian registry of heart failure - Clinical aspects, care quality and hospitalization outcomes. Arq Bras Cardiol. 2015; 104(6): 433-42.
|
| [40] |
Lee SE, Lee HY, Cho HJ, Choe WS, Kim H, Choi JO, et al. Clinical characteristics & outcome of acute heart failure in Korea: Results from the Korean acute heart failure registry (KorAHF). Korean Circ J. 2017; 47(3): 341-53.
|
| [41] |
Dokainish H, Teo K, Zhu J, Roy A, Alhabib KF, Elsayed A, et al. Articles Global mortality variations in patients with heart failure : results from the International Congestive Heart Failure (INTER-CHF) prospective cohort study. 2017; 665-72.
|
| [42] |
Callender T, Woodward M, Roth G, Farzadfar F, Lemarie JC, Gicquel S, et al. Heart failure care in low- and middle-income countries: A systematic review and meta-analysis. PLoS Med. 2015; 11(8).
|
| [43] |
Miró Ò, García Sarasola A, Fuenzalida C, Calderón S, Jacob J, Aguirre A, et al. Departments involved during the first episode of acute heart failure and subsequent emergency department revisits and rehospitalisations: an outlook through the NOVICA cohort. Eur J Heart Fail. 2019; 21(10): 1231-44.
|
| [44] |
Butt JH, Fosbøl EL, Gerds TA, Andersson C, McMurray JJV, Petrie MC, et al. Readmission and death in patients admitted with new-onset versus worsening of chronic heart failure: insights from a nationwide cohort. Eur J Heart Fail. 2020; 22(10): 1777-85.
|
| [45] |
CSA ECSA. Ethiopian 2022 Project Population Census. 2022; (July).
|
| [46] |
Chen X. Chinese clinical practice guideline for acute kidney injury. Natl Med J China. 2023; 103(42): 3332-66.
|
| [47] |
Is H, Use A. Preventing Cancer by Reducing Excessive Alcohol Use How Is Alcohol Use Defined ? What Is Considered One Drink ? What Are the Guidelines for Alcohol Use ?: 23-4.
|
| [48] |
Keller K. National Center for Health Statistics. Encycl Obes. 2014; 23-4.
|
| [49] |
Survey H. Ethiopia. 2016.
|
| [50] |
Mekonin G, Dukessa T, Dube L, Tadesse I. Acute heart failure outcome and predictors of outcome among patients admitted to Jimma University Medical Center, Southwest Ethiopia. 2022;
|
| [51] |
Demisse L, Alemayehu B, Addissie A, Azazh A, Gary R. Knowledge, attitudes and beliefs about acute coronary syndrome among patients diagnosed with acute coronary syndrome, Addis Ababa, Ethiopia. BMC Cardiovasc Disord. 2022; 22(1): 1-9. Available from:
https://doi.org/10.1186/s12872-022-02893-2
|
Cite This Article
-
APA Style
Abrahim, R. Y., Abdi, D., Azene, K. M., Lemma, B. F., Sedi, P. Y., et al. (2025). Clinical Characterstics and in Hospital Outcome of Acute Heart Failure Patients Admitted to Asella Teaching and Referral Hospital, South East Ethiopia, 2023. International Journal of Cardiovascular and Thoracic Surgery, 11(4), 45-62. https://doi.org/10.11648/j.ijcts.20251104.12
 Copy
|
Copy
|
 Download
Download
ACS Style
Abrahim, R. Y.; Abdi, D.; Azene, K. M.; Lemma, B. F.; Sedi, P. Y., et al. Clinical Characterstics and in Hospital Outcome of Acute Heart Failure Patients Admitted to Asella Teaching and Referral Hospital, South East Ethiopia, 2023. Int. J. Cardiovasc. Thorac. Surg. 2025, 11(4), 45-62. doi: 10.11648/j.ijcts.20251104.12
Copy
|
Download
AMA Style
Abrahim RY, Abdi D, Azene KM, Lemma BF, Sedi PY, et al. Clinical Characterstics and in Hospital Outcome of Acute Heart Failure Patients Admitted to Asella Teaching and Referral Hospital, South East Ethiopia, 2023. Int J Cardiovasc Thorac Surg. 2025;11(4):45-62. doi: 10.11648/j.ijcts.20251104.12
Copy
|
Download
-
@article{10.11648/j.ijcts.20251104.12,
author = {Rudwan Yasin Abrahim and Dawit Abdi and Kidist Mehari Azene and Bethelhem Fekadeselassie Lemma and Peniel Yigezu Sedi and Olifan Getachew},
title = {Clinical Characterstics and in Hospital Outcome of Acute Heart Failure Patients Admitted to Asella Teaching and Referral Hospital, South East Ethiopia, 2023
},
journal = {International Journal of Cardiovascular and Thoracic Surgery},
volume = {11},
number = {4},
pages = {45-62},
doi = {10.11648/j.ijcts.20251104.12},
url = {https://doi.org/10.11648/j.ijcts.20251104.12},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ijcts.20251104.12},
abstract = {Background: Acute heart failure represents a significant public health concern worldwide, posing a considerable burden on healthcare systems and often leading to adverse clinical outcomes, including high mortality rates. Thus, this study aimed to describe the in-hospital outcomes and associated factors for patients with acute heart failure. Which is vital for improving the quality of care and patient management. Objective: To determine clinical characteristics and in hospital outcome of acute heart failure patient admitted at Asella teaching and referral hospital. Methodology: The study employed an institution-based retrospective cohort design and assessed the clinical characteristics and in-hospital outcomes of acute heart failure (AHF) patients admitted to Asella Teaching and Referral Hospital. Data were collected from all patients admitted between September 2022 and September 2023. After manual checks for completeness, the data were coded and entered using Epi Info version 7.2 and analyzed with SPSS version 28. Descriptive statistics were used, presenting continuous variables as mean standard deviation or median (interquartile range) based on distribution either normal or not, respectively. In addition, categorical variables were presented as frequency and percentages. Kaplan-Meier method estimated and graphed survival probabilities over time and a Log-rank hypothesis test to compare survival functions of explanatory variables was utilized. Significant predictor variables were identified by fitting a semi parametric Cox’s proportional hazard model using a method of forward stepwise and statistical significance variables were declared based on a p-value less than 0.05. Result: Two hundred thirty one (231) patients were included in the study, with 121 (52.4%) being female. The median age of patients with acute heart failure was 56 years (IQR = 28 to 70). The commonest underlying disease and precipitating factor identified at admission was ischemic heart disease (36.4%) and pneumonia (24.68%) respectively. Out of the 231 patients, 13.4% died in the hospital. In the survival analysis the hazard ratios for precipitant factor pneumonia, acute kidney injury, lack of health insurance and age were identified 3.07 (95% CI: 1.40, 6.74, p = 0.005), 2.98 (95% CI: 1.31, 6.75, p = 0.009), 3.46 (95% CI: 1.51, 7.95, p = 0.003), and 2.81 (95% CI: 1.18, 6.72, p = 0.020), respectively as predictors of poor treatment outcome. Conclusion: Unfortunately, the in-hospital mortality rate for acute heart failure proved to be high in this study. The identified independent predictors of in-hospital mortality included pneumonia, acute kidney injury, lack of active health insurance coverage and age. The principal precipitating factors leading to hospitalization were pneumonia. Ischemic heart disease was identified as the most common underlying cardiac disease. Recommendation: Improve the consistency and availability of essential investigations. work on improving drug adherence and health insurance coverage.
},
year = {2025}
}
Copy
|
Download
-
TY - JOUR
T1 - Clinical Characterstics and in Hospital Outcome of Acute Heart Failure Patients Admitted to Asella Teaching and Referral Hospital, South East Ethiopia, 2023
AU - Rudwan Yasin Abrahim
AU - Dawit Abdi
AU - Kidist Mehari Azene
AU - Bethelhem Fekadeselassie Lemma
AU - Peniel Yigezu Sedi
AU - Olifan Getachew
Y1 - 2025/09/08
PY - 2025
N1 - https://doi.org/10.11648/j.ijcts.20251104.12
DO - 10.11648/j.ijcts.20251104.12
T2 - International Journal of Cardiovascular and Thoracic Surgery
JF - International Journal of Cardiovascular and Thoracic Surgery
JO - International Journal of Cardiovascular and Thoracic Surgery
SP - 45
EP - 62
PB - Science Publishing Group
SN - 2575-4882
UR - https://doi.org/10.11648/j.ijcts.20251104.12
AB - Background: Acute heart failure represents a significant public health concern worldwide, posing a considerable burden on healthcare systems and often leading to adverse clinical outcomes, including high mortality rates. Thus, this study aimed to describe the in-hospital outcomes and associated factors for patients with acute heart failure. Which is vital for improving the quality of care and patient management. Objective: To determine clinical characteristics and in hospital outcome of acute heart failure patient admitted at Asella teaching and referral hospital. Methodology: The study employed an institution-based retrospective cohort design and assessed the clinical characteristics and in-hospital outcomes of acute heart failure (AHF) patients admitted to Asella Teaching and Referral Hospital. Data were collected from all patients admitted between September 2022 and September 2023. After manual checks for completeness, the data were coded and entered using Epi Info version 7.2 and analyzed with SPSS version 28. Descriptive statistics were used, presenting continuous variables as mean standard deviation or median (interquartile range) based on distribution either normal or not, respectively. In addition, categorical variables were presented as frequency and percentages. Kaplan-Meier method estimated and graphed survival probabilities over time and a Log-rank hypothesis test to compare survival functions of explanatory variables was utilized. Significant predictor variables were identified by fitting a semi parametric Cox’s proportional hazard model using a method of forward stepwise and statistical significance variables were declared based on a p-value less than 0.05. Result: Two hundred thirty one (231) patients were included in the study, with 121 (52.4%) being female. The median age of patients with acute heart failure was 56 years (IQR = 28 to 70). The commonest underlying disease and precipitating factor identified at admission was ischemic heart disease (36.4%) and pneumonia (24.68%) respectively. Out of the 231 patients, 13.4% died in the hospital. In the survival analysis the hazard ratios for precipitant factor pneumonia, acute kidney injury, lack of health insurance and age were identified 3.07 (95% CI: 1.40, 6.74, p = 0.005), 2.98 (95% CI: 1.31, 6.75, p = 0.009), 3.46 (95% CI: 1.51, 7.95, p = 0.003), and 2.81 (95% CI: 1.18, 6.72, p = 0.020), respectively as predictors of poor treatment outcome. Conclusion: Unfortunately, the in-hospital mortality rate for acute heart failure proved to be high in this study. The identified independent predictors of in-hospital mortality included pneumonia, acute kidney injury, lack of active health insurance coverage and age. The principal precipitating factors leading to hospitalization were pneumonia. Ischemic heart disease was identified as the most common underlying cardiac disease. Recommendation: Improve the consistency and availability of essential investigations. work on improving drug adherence and health insurance coverage.
VL - 11
IS - 4
ER -
Copy
|
Download