Abstract
Background: Peripartum cardiomyopathy causes dilated cardiomyopathy, which develops late in pregnancy or early after childbirth and primarily affects African women. Patients frequently experience more frequent partial or complete recovery than patients with other forms of dilated cardiomyopathy do, emphasizing the crucial role of early diagnosis and management. Despite its global prevalence, there is currently a lack of comprehensive data on the disease's impact and contributing factors in Ethiopia. This study aimed to assess the prevalence of peripartum cardiomyopathy and its associated factors among reproductive-aged women with dilated cardiomyopathy who were hospitalized or on cardiac follow-up at three tertiary hospitals in Addis Ababa, Ethiopia. Methods: An institution-based cross-sectional study was conducted via a universal sampling method at three hospitals. Medical records of reproductive-aged women with Dilated cardiomyopathies that were hospitalized or attended follow-up from October 2021 to September 2023 at the three hospitals were reviewed. Both descriptive and analytical statistical methods were employed via SPSS version 29 for analysis, with the significance level set at a p value <0.05. Frequency tables, descriptive summaries, graphs, and charts were used for illustration. Results: Three hundred four women of reproductive age with dilated cardiomyopathy participated. The prevalence of peripartum cardiomyopathy was 22.7%. Bivariate and multiple logistic regression analyses revealed that preeclampsia [AOR 13.740, 95% CI 1.120--168.509], multiparty [AOR 6.01, 95% CI 1.91--18.93], gestational diabetes [AOR 10.95, 95% CI 1.62--74.09], pregnancy-related anemia [AOR 4.55, 95% CI 1.47--14.09], low socioeconomic status [AOR 6.83, 95% CI 2.06--22.68], and alcohol consumption during pregnancy [AOR 18.98, 95% CI 5.15--70.03] were significantly associated with an increased risk of peripartum cardiomyopathy. Conclusion: Peripartum cardiomyopathy is a common form of dilated cardiomyopathy in women of reproductive age. Its association with multiple demographic and obstetric risk factors highlights the need for improved risk assessment and further research. Clinical trial number: not applicable
Keywords
Peripartum Cardiomyopathy, Dilated Cardiomyopathy, Pregnancy, Ethiopia
1. Background
Cardiomyopathy represents a heterogeneous group of diseases characterized by structural and functional abnormalities of the myocardium, often culminating in heart failure. Among these, dilated cardiomyopathy [DCM] is the most prevalent form and is characterized by left ventricular dilation and impaired systolic function. The etiology of DCM is multifactorial, encompassing genetic predispositions, viral infections, autoimmune diseases, and environmental factors such as alcohol abuse and certain medications
| [1] | Schaufelberger M. Cardiomyopathy and pregnancy. Heart. 2019; 105(20): 1543-51. |
| [2] | Lorini FL, Rizza A, Ferri F. The cardiomyopathies. Textbook of Echocardiography for Intensivists and Emergency Physicians. 2019: 153-61. |
| [3] | Loscalzo J, Fauci AS, Kasper DL, Hauser SL, Longo DL, Jameson JL. Harrison's principles of internal medicine. 2022. |
[1-3]
. In many cases, the exact cause remains unidentified, leading to the classification of idiopathic DCM
| [4] | Felker GM, Hu W, Hare JM, Hruban RH, Baughman KL, Kasper EK. The spectrum of dilated cardiomyopathy: the Johns Hopkins experience with 1,278 patients. Medicine. 1999; 78(4): 270-83. |
[4]
.
Peripartum cardiomyopathy (PPCM) is a distinct form of DCM that occurs during the last month of pregnancy or within five months postpartum in women without prior cardiovascular disease
| [5] | Sliwa K, Hilfiker-Kleiner D, Petrie MC, Mebazaa A, Pieske B, Buchmann E, et al. Current state of knowledge on etiology, diagnosis, management, and therapy of peripartum cardiomyopathy: a position statement from the Heart Failure Association of the European Society of Cardiology Working Group on peripartum cardiomyopathy. European journal of heart failure. 2010; 12(8): 767-78. |
[5]
. Globally, PPCM affects approximately 1 in 1,000 to 1 in 4,000 live births
| [6] | Arany Z, Elkayam U. Peripartum cardiomyopathy. Circulation. 2016; 133(14): 1397-409. |
[6]
. While population-based studies in the United States
| [7] | Goland S, Modi K, Bitar F, Janmohamed M, Mirocha JM, Czer LS, et al. Clinical profile and predictors of complications in peripartum cardiomyopathy. Journal of cardiac failure. 2009; 15(8): 645-50. |
[7]
have identified African descent as a significant risk factor, data on the prevalence of PPCM in Ethiopia are limited. However, the Sub-Saharan Africa Survey of Heart Failure (THESUS–HF), conducted in 12 hospitals across 9 sub-Saharan African countries, including Ethiopia, revealed that PPCM contributes to 15% of acute heart failure cases in women
| [8] | Damasceno A, Mayosi BM, Sani M, Ogah OS, Mondo C, Ojji D, et al. The causes, treatment, and outcome of acute heart failure in 1006 Africans from 9 countries: results of the sub-Saharan Africa survey of heart failure. Archives of internal medicine. 2012; 172(18): 1386-94. |
[8]
. Additionally, a 2018 echocardiographic assessment of 398 pregnant women receiving antenatal care at SPHMMC identified one case of PPCM, highlighting the presence of this condition in Ethiopia as one of the leading causes of dilated cardiomyopathy and heart failure in this population
| [9] | Dawit Bacha M, Hailu Abera M, Abdusamed Adem M, Filagot Tadesse M, Delayehu Bekele M. THE OCCURRENCE AND PATTERN OF CARDIOVASCULAR DISEASES AMONG PREGNANT MOTHERS ATTENDING SAINT PAUL’S HOSPITAL IN ADDIS ABABA. |
[9]
.
The pathophysiology of PPCM is not fully understood; however, several hypotheses have been proposed, including genetic susceptibility, oxidative stress, and the role of circulating factors such as prolactin
| [10] | Halkein J, Tabruyn SP, Ricke-Hoch M, Haghikia A, Scherr M, Castermans K, et al. MicroRNA-146a is a therapeutic target and biomarker for peripartum cardiomyopathy. The Journal of clinical investigation. 2013; 123(5): 2143-54. |
| [11] | Ware JS, Li J, Mazaika E, Yasso CM, DeSouza T, Cappola TP, et al. Shared genetic predisposition in peripartum and dilated cardiomyopathies. New England Journal of Medicine. 2016; 374(3): 233-41. |
[10, 11]
.
Clinically, PPCM presents with symptoms of heart failure, including dyspnea, fatigue, edema, and palpitations
| [3] | Loscalzo J, Fauci AS, Kasper DL, Hauser SL, Longo DL, Jameson JL. Harrison's principles of internal medicine. 2022. |
[3]
. Physical examination may reveal signs such as elevated jugular venous pressure, a displaced apical impulse, and the presence of a third heart sound
| [5] | Sliwa K, Hilfiker-Kleiner D, Petrie MC, Mebazaa A, Pieske B, Buchmann E, et al. Current state of knowledge on etiology, diagnosis, management, and therapy of peripartum cardiomyopathy: a position statement from the Heart Failure Association of the European Society of Cardiology Working Group on peripartum cardiomyopathy. European journal of heart failure. 2010; 12(8): 767-78. |
[5]
. The diagnosis is established on the basis of specific criteria: the onset of heart failure symptoms during the last month of pregnancy or within five months postpartum, the exclusion of other identifiable causes of heart failure, and echocardiographic evidence of left ventricular systolic dysfunction (ejection fraction < 45%)
| [5] | Sliwa K, Hilfiker-Kleiner D, Petrie MC, Mebazaa A, Pieske B, Buchmann E, et al. Current state of knowledge on etiology, diagnosis, management, and therapy of peripartum cardiomyopathy: a position statement from the Heart Failure Association of the European Society of Cardiology Working Group on peripartum cardiomyopathy. European journal of heart failure. 2010; 12(8): 767-78. |
| [12] | Grasso M, Bondavalli D, Vilardo V, Cavaliere C, Gatti I, Di Toro A, et al. The new 2023 ESC guidelines for the management of cardiomyopathies: a guiding path for cardiologist decisions. European Heart Journal Supplements. 2024; 26 [Supplement_1]: i1-i5. |
[5, 12]
.
The incidence of PPCM varies significantly across different geographical regions and is influenced by demographic, socioeconomic, and healthcare access factors
| [13] | Shahid M, Ibrahim R, Ulhaque T, Nhat H, Sainbayar E, Lee K, et al. Peripartum Cardiomyopathy and Social Vulnerability: An Epidemiological Analysis of Mortality Outcomes. Journal of the American Heart Association. 2024: e034825. |
[13]
. The identified risk factors include advanced maternal age
| [14] | Lee S, Cho GJ, Park GU, Kim LY, Lee TS, Kim DY, Choi SW, Youn JC, Han SW, Ryu KH, Na JO, Choi CU, Seo HS, Kim EJ. Incidence, Risk Factors, and Clinical Characteristics of Peripartum Cardiomyopathy in South Korea. Circ Heart Fail. 2018 Apr; 11(4): e004134. |
[14]
, multiparty
| [15] | Gentry MB, Dias JK, Luis A, Patel R, Thornton J, Reed GL. African-American women have a higher risk for developing peripartum cardiomyopathy. Journal of the American College of Cardiology. 2010; 55(7): 654-9. |
[15]
, multiple gestations
| [16] | Lee S, Cho GJ, Park GU, Kim LY, Lee T-S, Kim DY, et al. Incidence, risk factors, and clinical characteristics of peripartum cardiomyopathy in South Korea. Circulation: Heart Failure. 2018; 11(4): e004134. |
[16]
, hypertensive disorders of pregnancy
| [17] | Huang G, Zhang L, Long-Le M, Le-Xin W. Clinical characteristics and risk factors for peripartum cardiomyopathy. African health sciences. 2012; 12(1): 26-31. |
[17]
, gestational DM
| [16] | Lee S, Cho GJ, Park GU, Kim LY, Lee T-S, Kim DY, et al. Incidence, risk factors, and clinical characteristics of peripartum cardiomyopathy in South Korea. Circulation: Heart Failure. 2018; 11(4): e004134. |
[16]
, tocolytics use
| [18] | Lampert MB, Hibbard J, Weinert L, Briller J, Lindheimer M, Lang RM. Peripartum heart failure associated with prolonged tocolytic therapy. American journal of obstetrics and gynecology. 1993; 168(2): 493-5. |
[18]
, and socioeconomic disadvantages
| [16] | Lee S, Cho GJ, Park GU, Kim LY, Lee T-S, Kim DY, et al. Incidence, risk factors, and clinical characteristics of peripartum cardiomyopathy in South Korea. Circulation: Heart Failure. 2018; 11(4): e004134. |
| [17] | Huang G, Zhang L, Long-Le M, Le-Xin W. Clinical characteristics and risk factors for peripartum cardiomyopathy. African health sciences. 2012; 12(1): 26-31. |
| [19] | Karaye KM, Ishaq N, Sa'idu H, Balarabe S, Talle M, Isa M, et al. Incidence, clinical characteristics, and risk factors for peripartum cardiomyopathy in Nigeria: results from the PEACE Registry. ESC heart failure. 2020; 7(1): 236-44. |
[16, 17, 19]
. Understanding these risk factors is crucial for developing targeted interventions to improve maternal and neonatal health outcomes.
This study aimed to assess the prevalence of PPCM and its associated risk factors among reproductive-aged women diagnosed with DCM who were hospitalized or receiving follow-up care at St. Paul’s Hospital Millennium Medical College, St. Peter's Specialized Hospital, and Tikur Anbessa Specialized Hospital in Ethiopia. Insights gained from this research will inform clinical practices and public health strategies in the region.
2. Methods
2.1. Study Design, Period and Settings
This cross-sectional study was conducted in three major public hospitals in Addis Ababa, Ethiopia: St. Paul’s Hospital Millennium Medical College (SPHMMC)
| [20] | Mengistu MD, Benti H. Assessment of magnitude and spectrum of cardiovascular disease admissions and outcomes in Saint Paul Hospital Millennium Medical College, Addis Ababa: A retrospective study. Plos one. 2022; 17(12): e0267527. |
[20]
, St. Peter's Specialized Hospital (SPSH)
| [21] | Zeru AB, Muluneh MA. Admission and inpatient mortality of hypertension complications in Addis Ababa. Integrated Blood Pressure Control. 2020: 103-10. |
[21]
, and Tikur Anbessa Specialized Hospital (TASH)
| [22] | Abdissa SG, Oli K, Feleke Y, Goshu DY, Begna DM, Tafese A. Spectrum of cardiovascular diseases among Ethiopian patients at Tikur Anbessa specialized university teaching hospital, Addis Ababa. Ethiop medj. 2014; 52(1): 9-17. |
[22]
. These institutions collectively serve a population exceeding 4 million and were selected because they provide comprehensive cardiac care, including echocardiography and obstetric services, in the country. The study was conducted from October 2021 to September 2023.
2.2. Study Population
The study population comprised reproductive-aged women diagnosed with DCM who were either hospitalized or under cardiac follow-up at the selected hospitals during the study period.
2.3. Inclusion and Exclusion Criteria
The inclusion criteria were as follows: reproductive-aged women (15–49 years) diagnosed with DCM and receiving care at the selected hospitals during the study timeframe.
The exclusion criterion for women was incomplete medical records that could not be supplemented through telephone interviews, particularly if missing data for key variables exceeded 10%.
2.4. Sample Size and Sampling Technique
The sample size was determined via both single and double population proportion formulas. The single population proportion formula yielded a sample size of 384, assuming a prevalence of 50% for the maximum sample size calculation. The double population proportion formula was employed to assess specific risk factors, with the largest calculated sample size being 190 for preeclampsia.
The single population proportion formula was used to obtain a sample size of 384:
n= required sample size
Z= confidence level at 95% [standard value of 1.96]
d= margin of error = 5%
P= estimated prevalence of PPCM among reproductive-age women was not known in Ethiopia, and 50% was taken as the proportion of the population to provide the maximum sample size.
Therefore, when we substituted the values in the formula, a sample size of 384
n=384
The double population proportion formula was used to calculate the sample size required to determine factors associated with PPCM.
where n is the sample size, is the critical value of the normal distribution at α/2 [e.g., for a confidence level of 95%, α is 0.05, and the critical value is 1.96], is the critical value of the normal distribution at β [e.g., for a power of 80%, β is 0.2, and the critical value is 0.84], and and are the expected sample proportions of the two groups.
Factors that are consistently reported to have a significant association with PPCM in previous studies were used:
1) Preeclampsia (OR, 6.02, P1=97, P2=84)
| [16] | Lee S, Cho GJ, Park GU, Kim LY, Lee T-S, Kim DY, et al. Incidence, risk factors, and clinical characteristics of peripartum cardiomyopathy in South Korea. Circulation: Heart Failure. 2018; 11(4): e004134. |
[16]
, calculated sample size=190
2) No formal education (OR, 3.08, P1=85, P2=64)
| [19] | Karaye KM, Ishaq N, Sa'idu H, Balarabe S, Talle M, Isa M, et al. Incidence, clinical characteristics, and risk factors for peripartum cardiomyopathy in Nigeria: results from the PEACE Registry. ESC heart failure. 2020; 7(1): 236-44. |
[19]
, calculated sample size=160
3) Multiparity (OR: 2.9, P1=61, P2=35)
| [23] | Ntusi NB, Mayosi BM. Etiology and risk factors for peripartum cardiomyopathy: a systematic review. International journal of cardiology. 2009; 131(2): 168-79. |
[23]
, calculated sample size=160
4) Being unmarried (OR: 4.2, P1=51, P2=20)
| [15] | Gentry MB, Dias JK, Luis A, Patel R, Thornton J, Reed GL. African-American women have a higher risk for developing peripartum cardiomyopathy. Journal of the American College of Cardiology. 2010; 55(7): 654-9. |
[15]
, calculated sample size=84
Since the sample size calculated via the single population proportion formula was greater than the value calculated for each of the factors via the double population proportion formula, n was set to 384.
Upon HMIS and chart/EMR review, 378 reproductive-aged women with DCM were hospitalized or actively followed up at SPHMMC, SPSH, and TASH between October 2021 and September 2023, G.C.
Because the source population is <10,000, a population correction formula is needed.
= initial sample size=384
N= study population (Reproductive-aged women who were actively followed up or hospitalized at the three hospitals from October 2021 to September 2023) = 378
190.48
By adding a 10% contingency, a minimum sample size of 210 is found.
Upon reviewing the Health Management Information System (HMIS) and EMRs, 378 reproductive-aged women with DCM were eligible. Assuming a minimum required sample size of 210 to address both the descriptive and analytical questions of the study, and considering the financial and time feasibility of including all 378 eligible participants, a universal sampling method was employed to encompass all eligible individuals.
2.5. Study Variables
Dependent Variable: Peripartum cardiomyopathy (yes/no).
Independent Variables:
1) Sociodemographic factors: Age, education level, socioeconomic status, marital status, occupation, and alcohol use during pregnancy.
2) Obstetric factors: Parity, multiple pregnancies, hypertensive disorders, and tocolytic use.
3) Clinical factors: Chronic hypertension, pregestational diabetes, gestational diabetes, overt diabetes, and anemia during pregnancy.
2.6. Operational Definitions
1) DCM: Diagnosed via echocardiography, characterized by left ventricular dilation and/or systolic dysfunction not attributable to other cardiac conditions
| [24] | Arbelo E, Protonotarios A, Gimeno JR, Arbustini E, Barriales-Villa R, Basso C, et al. 2023 ESC Guidelines for the management of cardiomyopathies: Developed by the task force on the management of cardiomyopathies of the European Society of Cardiology [ESC]. European heart journal. 2023; 44(37): 3503-626. |
[24]
.
2) PPCM: A form of DCM occurring within the last month of pregnancy or up to five months postpartum, with echocardiographic evidence of left ventricular systolic dysfunction (EF < 45%)
| [25] | Bauersachs J, König T, van der Meer P, Petrie MC, Hilfiker-Kleiner D, Mbakwem A, et al. Pathophysiology, diagnosis and management of peripartum cardiomyopathy: a position statement from the Heart Failure Association of the European Society of Cardiology Study Group on peripartum cardiomyopathy. European journal of heart failure. 2019; 21(7): 827-43. |
[25]
.
3) Reproductive Age Group: Women aged 15--49 years
| [26] | ARSLAN CD. The Effects of Reproductive Right Policies on Women’s Experience of Egg and Embryo Freezing Process in Turkey: Middle East Technical University; 2022. |
[26]
.
4) Parous Women: Women who have given birth one or more times
| [27] | Bakketeig LS, Jacobsen G, Hoffman HJ, Lindmark G, Bergsjø P, Molne K, et al. Pre-pregnancy risk factors for small-for-gestational age births among parous women in Scandinavia. Acta obstetricia et gynecologica Scandinavica. 1993; 72(4): 273-9. |
[27]
.
2.7. Data Collection Tools, Methods and Procedures
Data were collected via a structured checklist adapted from a validated case‒control study conducted in Shandong Province, China
| [17] | Huang G, Zhang L, Long-Le M, Le-Xin W. Clinical characteristics and risk factors for peripartum cardiomyopathy. African health sciences. 2012; 12(1): 26-31. |
[17]
. The checklist was designed to capture comprehensive information regarding sociodemographic, obstetric, and clinical factors relevant to PPCM. Trained internal medicine residents and general practitioners gathered data from patient charts and EMRs over two months (November 1 to December 30, 2023). Missing data were supplemented through telephone interviews, which utilized contact information from patient records. Data were captured digitally via KoBoToolbox to ensure standardization and efficiency
| [28] | Lakshminarasimhappa M. Web-based and smart mobile app for data collection: Kobo Toolbox/Kobo collect. Journal of Indian Library Association Now Available at https://journalilaindianet/ 2022; 57(2): 72-9. |
[28]
.
2.8. Data Quality Control
A pretest of the data collection checklist was conducted with 5% of the total study population to assess its validity and completeness. Data collectors received training on the study objectives, data collection methods, and ethical considerations. The investigator monitored the data collection for accuracy and completeness, ensuring adherence to the study protocol.
2.9. Data Processing and Analysis
The collected data were checked for consistency and completeness, coded, and entered into the KoBoToolbox. Statistical analysis was performed via the Statistical Package for Social Sciences (SPSS) version 29. Descriptive statistics were employed to summarize demographic and clinical characteristics. Categorical data were analyzed as frequencies and percentages, whereas continuous data were expressed as the means with standard deviations.
For parous women with DCM, simple binary logistic regression and multivariable analysis were employed to calculate crude and adjusted odds ratios (ORs) with 95% confidence intervals (CIs) to identify risk factors for PPCM. A P value < 0.05 was considered statistically significant. The results are presented via tables, figures, and narrative descriptions to facilitate understanding.
3. Results
3.1. Sociodemographic Characteristics
A total of 304 reproductive-aged women diagnosed with dilated cardiomyopathy (DCM) were included in this study, with participants sourced from three tertiary hospitals: St. Paul’s Hospital Millennium Medical College (SPHMMC) (n = 107), St. Peter's Specialized Hospital (SPSH) (n = 74), and Tikur Anbessa Specialized Hospital (TASH) (n= 123). Among these participants, a significant majority (78.0%) resided in urban areas. The mean age of the participants was 32.8 years, with a standard deviation of 7.7 years.
Educational attainment was notably high, with 86.5% of participants having engaged in formal education. In terms of employment status, 55% of the participants were employed. Socioeconomic status (SES) analysis indicated that a substantial 63.5% of the patients belonged to the low SES classification. In terms of marital status, 79.3% of the patients were married, and 78.9% were parous (see
Table 1).
Table 1. Sociodemographic characteristics of reproductive-aged women with DCM in three tertiary hospitals, Addis Ababa, Ethiopia, 2024 (n= 304).
Sociodemographic characteristics | Subgroup | Frequency (n) | Percent (%) |
Place of residency | Rural | 67 | 22.0 |
Urban | 237 | 78.0 |
Age group | <25 | 57 | 18.8 |
25-35 | 118 | 38.8 |
>35 | 129 | 42.4 |
Occupation status | Employed | 167 | 54.9 |
Un employed | 137 | 45.1 |
SES | Low SES | 151 | 49.7 |
Higher SES | 153 | 50.3 |
Educational level | Formal education | 263 | 86.5 |
No formal education | 41 | 13.5 |
Marital status | Married | 241 | 79.3 |
Unmarried | 63 | 20.7 |
Parity | Parous | 240 | 78.9 |
Nulliparous | 64 | 21.1 |
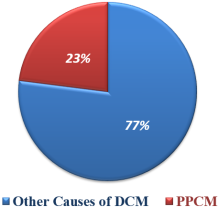
Figure 1. Prevalence of PPCM among reproductive-aged women with DCM in three tertiary hospitals, Addis Ababa, Ethiopia, 2024.
3.2. Prevalence of PPCM Among Reproductive-Aged Women with DCM
Among the 304 reproductive-aged women diagnosed with DCM, 69 participants were diagnosed with peripartum cardiomyopathy (PPCM), resulting in a prevalence of 22.7% (
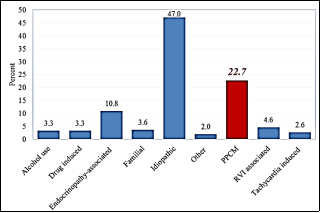
Figure 1). This finding indicates that PPCM is the most prevalent identifiable cause of DCM following idiopathic DCM, accounting for 47.0% of cases.
The analysis of other causes of DCM revealed that endocrinopathy-associated cardiomyopathy accounted for 10.8% of the cases, which was primarily associated with hyperthyroidism (n = 35) and hypothyroidism (n = 2). Right ventricular infarction (RVI)-associated cardiomyopathy accounted for 4.6% of the cases, whereas familial DCM accounted for 3.6%. Drug-induced DCM was noted in 8 patients due to Doxorubicin, 1 patient due to Idarubicin, and 1 patient due to Zidovudine, accounting for 3.3% of the patients. Alcoholic cardiomyopathy has been reported in an equal number of cases as drug-induced DCM. Tachycardia-induced DCM constituted 2.6% of the cases, whereas the remaining 2% were attributed to Takotsubo cardiomyopathy (n = 1), systemic lupus erythematosus (n = 3), rheumatoid arthritis (n = 1), or end-stage renal disease (n = 1) [
Figure 2].
Figure 2. Causes of DCM among reproductive-aged women with DCM in three tertiary hospitals, Addis Ababa, Ethiopia, 2024.
Overall, these findings underscore the importance of PPCM as the most prevalent identifiable cause of DCM among reproductive-aged women.
3.3. Factors Associated with PPCM Among Parous Women with DCM
Several factors were identified as significantly associated with PPCM among parous women with DCM. These included unemployment, low socioeconomic status (SES), multiparity, hypertensive disorders of pregnancy (HDP), preeclampsia, tocolytic use, gestational diabetes mellitus (DM), anemia during pregnancy, and alcohol use during pregnancy, all of which presented P values < 0.25 in the univariable analysis.
After adjusting for other variables via multivariable binary logistic regression, factors with a P value less than 0.25 were assessed to enhance the reliability of the findings regarding their association with the risk of PPCM. The analysis revealed that low SES was significantly associated with an increased risk of PPCM (adjusted odds ratio [AOR] 6.834, 95% confidence interval [CI] 2.059–22.682). Additionally, multiparity [AOR 6.013, 95% CI 1.910--18.935], preeclampsia [AOR 13.740, 95% CI 1.120--168.509], gestational DM [AOR 10.946, 95% CI 1.617--74.095], anemia during pregnancy [AOR 4.551, 95% CI 1.470--14.094], and alcohol consumption during pregnancy [AOR 18.985, 95% CI 5.147--70.035] were also significantly associated with an increased risk of PPCM. Conversely, unemployment was found to be significantly associated with a reduced risk of PPCM [AOR 0.299, 95% CI 0.094–0.952] (
Table 2). Notably, the associations between HDPs and tocolytic use were found to be statistically insignificant.
Table 2. Bivariable and multivariable logistic regression analysis of factors associated with PPCM in three tertiary hospitals, Addis Ababa, Ethiopia, 2024.
Variables | Bivariable | Multivariable |
COR (95% CI) | P- value | AOR (95% CI) | P- value |
Unemployment | 1.918 (1.089-3.378) | 0.024 | 0.299 (0.094-0.952) | 0.041 |
Low SES | 2.957 (1.645-5.314) | <0.001 | 6.834 (2.059-22.682) | 0.002 |
Multiparity | 3.454 (1.787-6.676) | <0.001 | 6.013 (1.910-18.935) | 0.002 |
HDP | 32.251 (11.781-88.290) | <0.001 | 7.013 (0.957-51.384) | 0.055 |
Preeclampsia | 68.934 (15.809-300.583) | <0.001 | 13.740 (1.120-168.509) | 0.040 |
Tocolytics use | 25.500 (3.164-205.515) | 0.002 | 9.442 (0.258-345.273) | 0.221 |
Gestational DM | 25.509 (5.680-114.555) | <0.001 | 10.946 (1.617-74.095) | 0.014 |
Anemia during pregnancy | 4.238 (2.050-8.764) | <0.001 | 4.551 (1.470-14.094) | 0.009 |
Alcohol during pregnancy | 6.353 (2.689-15.010) | 0.01 | 18.985 (5.147-70.035) | <0.001 |
Significant, P-value<0.05
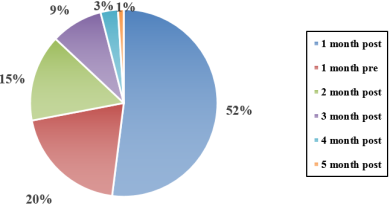
Furthermore, the results indicated that the period with the highest risk for PPCM diagnosis was the first postpartum period, accounting for 52% of the cases. In comparison, the last month of pregnancy accounted for 20% of the cases (
Figure 3). The frequency of diagnoses decreased as the timeframe moved beyond the initial postpartum period.
Figure 3. Timing of PPCM diagnosis relative to delivery in three tertiary hospitals, Addis Ababa, Ethiopia, 2024.
4. Discussion
This study aimed to assess the prevalence of peripartum cardiomyopathy (PPCM) and its associated factors among reproductive-aged women with dilated cardiomyopathy (DCM) who were hospitalized or receiving cardiac follow-up at selected tertiary hospitals in Addis Ababa, Ethiopia, in 2023. Among the 304 cases of DCM, 69 were attributed to PPCM, resulting in a prevalence rate of 22.7%. This prevalence is notably higher than the 11.3% reported at Johns Hopkins Hospital
| [29] | Kasper EK, Agema WR, Hutchins GM, Deckers JW, Hare JM, Baughman KL. The causes of dilated cardiomyopathy: a clinicopathologic review of 673 consecutive patients. Journal of the American College of Cardiology. 1994; 23(3): 586-90. |
| [30] | Felker GM, Thompson RE, Hare JM, Hruban RH, Clemetson DE, Howard DL, et al. Underlying causes and long-term survival in patients with initially unexplained cardiomyopathy. New England Journal of Medicine. 2000; 342(15): 1077-84. |
[29, 30]
. While variations in the definition of cardiomyopathy and differences in the mean age of participants may limit direct comparisons, the findings underscore the significant burden of PPCM in this population.
When the prevalence of PPCM reported in this study was compared with that reported in previous studies conducted in Africa, the rate of 22.7% aligns closely with the 19.2% prevalence reported in a 16-year review in Lagos, Nigeria
| [31] | Mbakwem AC, Amadi CE, Ajuluchukwu JN, Kushimo OA. Trends and outcomes of cardiovascular disease admissions in Lagos, Nigeria: a 16-year review. Cardiovascular Journal of Africa. 2023; 34(3): 140-8. |
[31]
. However, it is lower than the 38.7% prevalence reported in a retrospective analysis of echocardiographic patterns of heart diseases in Kano, Nigeria
| [32] | Karaye K, Sani M. The impact of income on the echocardiographic pattern of heart diseases in Kano, Nigeria. Nigerian Journal of Medicine. 2008; 17(3): 350-5. |
[32]
. Notably, PPCM emerged as the most identifiable cause of DCM among reproductive-aged women in this study, corroborating findings from similar studies in Nigeria
| [31] | Mbakwem AC, Amadi CE, Ajuluchukwu JN, Kushimo OA. Trends and outcomes of cardiovascular disease admissions in Lagos, Nigeria: a 16-year review. Cardiovascular Journal of Africa. 2023; 34(3): 140-8. |
| [32] | Karaye K, Sani M. The impact of income on the echocardiographic pattern of heart diseases in Kano, Nigeria. Nigerian Journal of Medicine. 2008; 17(3): 350-5. |
[31, 32]
. This highlights the ongoing significance of PPCM as a critical health concern for reproductive-aged women, particularly in the African context.
Several factors were identified as increasing the risk of PPCM in this study. Notably, compared with primiparous mothers, multiparous mothers presented a 6.013-fold greater likelihood of developing PPCM [AOR 6.013, 95% CI 1.910--18.935]. This finding is consistent with a large prospective study conducted in northern California, which reported an increased risk associated with multiparity [OR 2.1; 95% CI, 1.2–4.0]
| [33] | Gunderson EP, Croen LA, Chiang V, Yoshida CK, Walton D, Go AS. Epidemiology of peripartum cardiomyopathy: incidence, predictors, and outcomes. Obstetrics & Gynecology. 2011; 118(3): 583-91. |
[33]
, as well as a case‒control study in Georgia, indicating an association between having more than two previous pregnancies and PPCM [OR: 2.9, 95% CI: 1.1–7.4]
| [23] | Ntusi NB, Mayosi BM. Etiology and risk factors for peripartum cardiomyopathy: a systematic review. International journal of cardiology. 2009; 131(2): 168-79. |
[23]
.
Gestational diabetes mellitus (DM) was also found to significantly increase the risk of PPCM in this study [AOR 10.946, 95% CI 1.617–74.095], which aligns with findings from a population-based study in Korea [OR 1.70; 95% CI 1.26–2.29]
| [16] | Lee S, Cho GJ, Park GU, Kim LY, Lee T-S, Kim DY, et al. Incidence, risk factors, and clinical characteristics of peripartum cardiomyopathy in South Korea. Circulation: Heart Failure. 2018; 11(4): e004134. |
[16]
. While hypertensive heart disease, chronic hypertension, and superimposed hypertension did not show statistical significance in this study, preeclampsia exhibited a notable correlation with an increased risk of PPCM [AOR 13.740, 95% CI 1.120–168.509]. This finding is consistent with results from other studies, including a population-based Korean study [OR 6.02; 95% CI 4.94–7.34]
| [16] | Lee S, Cho GJ, Park GU, Kim LY, Lee T-S, Kim DY, et al. Incidence, risk factors, and clinical characteristics of peripartum cardiomyopathy in South Korea. Circulation: Heart Failure. 2018; 11(4): e004134. |
[16]
, a large prospective study in northern California [OR 4.1; 95% CI 1.9–8.5]
| [33] | Gunderson EP, Croen LA, Chiang V, Yoshida CK, Walton D, Go AS. Epidemiology of peripartum cardiomyopathy: incidence, predictors, and outcomes. Obstetrics & Gynecology. 2011; 118(3): 583-91. |
[33]
, and a longitudinal Nigerian study [OR 9.01, 95% CI: 2.18--37.75]
| [19] | Karaye KM, Ishaq N, Sa'idu H, Balarabe S, Talle M, Isa M, et al. Incidence, clinical characteristics, and risk factors for peripartum cardiomyopathy in Nigeria: results from the PEACE Registry. ESC heart failure. 2020; 7(1): 236-44. |
[19]
, all of which reported a significant correlation between preeclampsia and a greater risk of PPCM.
Additionally, anemia during pregnancy was linked to PPCM [AOR 4.551, 95% CI 1.470--14.094], corroborating findings from a large prospective study in northern California [OR 2.8, 95% CI: 1.6--4.7]
| [33] | Gunderson EP, Croen LA, Chiang V, Yoshida CK, Walton D, Go AS. Epidemiology of peripartum cardiomyopathy: incidence, predictors, and outcomes. Obstetrics & Gynecology. 2011; 118(3): 583-91. |
[33]
. The associations of low socioeconomic status [SES] [AOR 6.834, 95% CI 2.059--22.682] and alcohol consumption during pregnancy [AOR 18.985, 95% CI 5.147--70.035] with increased risk of PPCM are supported by a case‒control study in Georgia, which revealed elevated associations for both factors [low SES: OR 21.9, 95% CI 3.2--147.5; alcohol consumption: OR 29.1, 95% CI 3.8--221.3]
| [23] | Ntusi NB, Mayosi BM. Etiology and risk factors for peripartum cardiomyopathy: a systematic review. International journal of cardiology. 2009; 131(2): 168-79. |
[23]
. Furthermore, a retrospective study in Kano, Nigeria, revealed that all patients diagnosed with PPCM exhibited low SES, with incomes below $76.9, reinforcing the association of low SES with PPCM
| [32] | Karaye K, Sani M. The impact of income on the echocardiographic pattern of heart diseases in Kano, Nigeria. Nigerian Journal of Medicine. 2008; 17(3): 350-5. |
[32]
.
Interestingly, this study revealed a lower risk of PPCM associated with unemployment during pregnancy [AOR 0.299, 95% CI 0.094--0.952], whereas a longitudinal study in Nigeria suggested an increased risk of PPCM among unemployed women [OR 3.28, 95% CI 2.05--5.24]
| [19] | Karaye KM, Ishaq N, Sa'idu H, Balarabe S, Talle M, Isa M, et al. Incidence, clinical characteristics, and risk factors for peripartum cardiomyopathy in Nigeria: results from the PEACE Registry. ESC heart failure. 2020; 7(1): 236-44. |
[19]
. Additionally, while advanced maternal age has been identified as a risk factor for PPCM, the relationship remains ambiguous. This study revealed that a maternal age of 35 years or older was associated with a lower risk of PPCM [COR 0.310; 95% CI 0.110–0.879], which aligns with the findings of a longitudinal study in Nigeria that reported decreased odds of PPCM with increased maternal age [>30 years] [OR 0.745; 95% CI 0.475–1.167]
| [19] | Karaye KM, Ishaq N, Sa'idu H, Balarabe S, Talle M, Isa M, et al. Incidence, clinical characteristics, and risk factors for peripartum cardiomyopathy in Nigeria: results from the PEACE Registry. ESC heart failure. 2020; 7(1): 236-44. |
[19]
. In contrast, population-based studies in Korea and a large prospective study in northern California reported that a maternal age of 35 years or older was linked to an increased risk of PPCM [OR 1.56; 95% CI 1.32–1.83]
| [16] | Lee S, Cho GJ, Park GU, Kim LY, Lee T-S, Kim DY, et al. Incidence, risk factors, and clinical characteristics of peripartum cardiomyopathy in South Korea. Circulation: Heart Failure. 2018; 11(4): e004134. |
[16]
and [OR 3.0; 95% CI 1.3–7.0]
| [33] | Gunderson EP, Croen LA, Chiang V, Yoshida CK, Walton D, Go AS. Epidemiology of peripartum cardiomyopathy: incidence, predictors, and outcomes. Obstetrics & Gynecology. 2011; 118(3): 583-91. |
[33]
, respectively. These contradictory findings create uncertainty regarding the correlation between employment status and maternal age during pregnancy with PPCM.
Previous studies have identified a lack of formal education [OR 3.08, 95% CI 1.71--5.53]
| [19] | Karaye KM, Ishaq N, Sa'idu H, Balarabe S, Talle M, Isa M, et al. Incidence, clinical characteristics, and risk factors for peripartum cardiomyopathy in Nigeria: results from the PEACE Registry. ESC heart failure. 2020; 7(1): 236-44. |
[19]
and being unmarried during pregnancy [OR 4.2, 95% CI 1.4--12.3]
| [15] | Gentry MB, Dias JK, Luis A, Patel R, Thornton J, Reed GL. African-American women have a higher risk for developing peripartum cardiomyopathy. Journal of the American College of Cardiology. 2010; 55(7): 654-9. |
[15]
as factors correlated with PPCM. However, this study did not find a statistically significant association between formal education or marital status and PPCM, despite observing higher odds [1.5 times and 2.5 times, respectively].
5. Strengths and Limitations of the Study
This study presents several strengths, notably, its execution across three distinct tertiary hospitals over an extended period, which enhances the generalizability of the findings and allows for the identification of statistically significant associations related to various factors influencing peripartum cardiomyopathy [PPCM]. The data collection process was characterized by meticulous attention to detail, utilizing validated tools to gather information while ensuring the utmost confidentiality of the participants' data.
However, the study also faces inherent limitations. The definitive diagnosis of PPCM is challenging due to its classification as a diagnosis of exclusion, compounded by the lack of a specific diagnostic test. This complexity makes it difficult to confirm PPCM, even with comprehensive testing aimed at ruling out other potential causes of dilated cardiomyopathy [DCM], which may arise from pregnancy-related hemodynamic changes. Additionally, the retrospective design of the study and reliance on secondary data sources may restrict the quality of the data and limit control over the data collection process.
Despite these limitations, this study provides valuable insights that contribute to the existing body of knowledge on PPCM. This finding underscores the critical need for further research to address and mitigate the impact of PPCM, particularly in vulnerable populations. Future studies should aim to utilize prospective designs and standardized diagnostic criteria to increase the reliability of findings and inform effective interventions.
6. Conclusion
In conclusion, this study highlights the significant prevalence of PPCM among reproductive-aged women with DCM in Addis Ababa, Ethiopia, and identifies several associated risk factors. The findings underscore the need for increased awareness and targeted interventions to address PPCM in this vulnerable population, particularly in the context of low SES, multiparity, gestational diabetes, preeclampsia, and alcohol consumption during pregnancy. Further research is warranted to explore the underlying mechanisms and to develop effective prevention and management strategies for PPCM in Ethiopia and similar settings.
The authors recommend conducting larger prospective studies to further investigate the prevalence, incidence, and associated factors of PPCM. Such studies should aim to minimize the limitations encountered in this research, with the objective of determining the burden of PPCM per live birth and accurately identifying its risk factors.
Additionally, it is crucial to pay attention to PPCM by incorporating high-risk mothers into antenatal care [ANC] and obstetric risk assessment guidelines. This approach should facilitate risk modification and early diagnosis. We encourage healthcare providers to carefully identify mothers at risk for PPCM and to implement strategies to address modifiable risk factors, ensuring early detection and intervention.
Abbreviations
AOR | Adjusted Odds Ratio |
CI | Confidence Interval |
COR | Crude Odds Ratio |
DCM | Dilated Cardiomyopathy |
DM | Diabetes Mellitus |
EC | Ethiopian Calendar |
EF | Ejection Fraction |
EMR | Electrical Medical Record |
GBD | Global Burden of Diseases |
GC | Gregorian Calendar |
HDP | Hypertensive Disorders of Pregnancy |
HF | Heart Failure |
IHD | Ischemic Heart Disease |
LV | Left Ventricle |
LVIDd | Left Ventricle Internal Diameter at the End Diastole |
LVIDs | Left Ventricle Internal Diameter at the End Systole |
OR | Odds Ratio |
PPCM | Peripartum Cardiomyopathy |
RVI | Retroviral Infection |
SD | Standard Deviation |
SES | Socioeconomic Status |
SPHMMC | St. Paul’s Hospital Millennium Medical College |
SPSH | St. Peter’s Specialized Hospital |
SPSS | Statistical Package of Social Sciences |
TASH | Tikur Anbesa Specialized Hospital |
Acknowledgments
The authors express their gratitude to SPHMMC, SPSH, and TASH for providing access to the data source. The authors also thank the staff of the aforementioned institutions for their cooperation during the data collection period. Moreover, we thank those who provided invaluable suggestions, comments and advice throughout the research process.
Declarations
Ethics Approval and Consent to Participants
Ethical approval was obtained from the institutional review board of SPHMMC with Reference number of SPM23/946 prior to conducting the research and then letters for cooperation were also obtained for the remaining two hospitals. The informed consent requirements for chart review were waived by the institution ethics committee. To maintain patient confidentiality, names and other identifying information that could reveal patients' identities were kept confidential and anonymous. Informed verbal consent-taking, choosing convenient interview times for respondents, and providing respondents with privacy, respect, and empathetic inquiry were undertaken during telephone interviews. Furthermore, the scientific objectivity of the study was maintained with honesty, and the information collected from charts and interviews was respected and used only for the purpose of the study.
Consent for Publication
Not applicable.
Availability of Data and Materials
The datasets used and/or analyzed during this study are available from the corresponding author upon reasonable request.
Author Contributions
Ermiyas Berehanu Hayle: Conceptualization, Data curation, Formal Analysis, Investigation, Methodology, Project administration, Resources, Software, Validation, Visualization, Writing – original draft, Writing – review & editing
Adane Mamo Biabeyn: Conceptualization, Data curation, Formal Analysis, Investigation, Methodology, Project administration, Resources, Software, Validation, Visualization, Writing – original draft, Writing – review & editing
Wasihun Zerfu Zewde: Methodology, Resources, Software
Besufekad Tesfu Taye: Data curation, Formal Analysis, Software
Eyerusalem Girma Abebe: Data curation, Methodology, Validation, Visualization
Amsalu Alem Bahre: Methodology, Validation, Visualization
Tsion Habtamu Ababiya: Resources, Validation, Visualization
Abel Tesfaye Moges: Methodology, Resources, Software
Asfaw Hagos Shumye: I Investigation, Formal Analysis, Software
Asefa Adimasu Taddese: Supervision, Methodology, Validation
Funding
The author[s] did not receive financial support for this research, authorship or publication.
Conflicts of Interest
The authors declare no conflicts of interest.
References
| [1] |
Schaufelberger M. Cardiomyopathy and pregnancy. Heart. 2019; 105(20): 1543-51.
|
| [2] |
Lorini FL, Rizza A, Ferri F. The cardiomyopathies. Textbook of Echocardiography for Intensivists and Emergency Physicians. 2019: 153-61.
|
| [3] |
Loscalzo J, Fauci AS, Kasper DL, Hauser SL, Longo DL, Jameson JL. Harrison's principles of internal medicine. 2022.
|
| [4] |
Felker GM, Hu W, Hare JM, Hruban RH, Baughman KL, Kasper EK. The spectrum of dilated cardiomyopathy: the Johns Hopkins experience with 1,278 patients. Medicine. 1999; 78(4): 270-83.
|
| [5] |
Sliwa K, Hilfiker-Kleiner D, Petrie MC, Mebazaa A, Pieske B, Buchmann E, et al. Current state of knowledge on etiology, diagnosis, management, and therapy of peripartum cardiomyopathy: a position statement from the Heart Failure Association of the European Society of Cardiology Working Group on peripartum cardiomyopathy. European journal of heart failure. 2010; 12(8): 767-78.
|
| [6] |
Arany Z, Elkayam U. Peripartum cardiomyopathy. Circulation. 2016; 133(14): 1397-409.
|
| [7] |
Goland S, Modi K, Bitar F, Janmohamed M, Mirocha JM, Czer LS, et al. Clinical profile and predictors of complications in peripartum cardiomyopathy. Journal of cardiac failure. 2009; 15(8): 645-50.
|
| [8] |
Damasceno A, Mayosi BM, Sani M, Ogah OS, Mondo C, Ojji D, et al. The causes, treatment, and outcome of acute heart failure in 1006 Africans from 9 countries: results of the sub-Saharan Africa survey of heart failure. Archives of internal medicine. 2012; 172(18): 1386-94.
|
| [9] |
Dawit Bacha M, Hailu Abera M, Abdusamed Adem M, Filagot Tadesse M, Delayehu Bekele M. THE OCCURRENCE AND PATTERN OF CARDIOVASCULAR DISEASES AMONG PREGNANT MOTHERS ATTENDING SAINT PAUL’S HOSPITAL IN ADDIS ABABA.
|
| [10] |
Halkein J, Tabruyn SP, Ricke-Hoch M, Haghikia A, Scherr M, Castermans K, et al. MicroRNA-146a is a therapeutic target and biomarker for peripartum cardiomyopathy. The Journal of clinical investigation. 2013; 123(5): 2143-54.
|
| [11] |
Ware JS, Li J, Mazaika E, Yasso CM, DeSouza T, Cappola TP, et al. Shared genetic predisposition in peripartum and dilated cardiomyopathies. New England Journal of Medicine. 2016; 374(3): 233-41.
|
| [12] |
Grasso M, Bondavalli D, Vilardo V, Cavaliere C, Gatti I, Di Toro A, et al. The new 2023 ESC guidelines for the management of cardiomyopathies: a guiding path for cardiologist decisions. European Heart Journal Supplements. 2024; 26 [Supplement_1]: i1-i5.
|
| [13] |
Shahid M, Ibrahim R, Ulhaque T, Nhat H, Sainbayar E, Lee K, et al. Peripartum Cardiomyopathy and Social Vulnerability: An Epidemiological Analysis of Mortality Outcomes. Journal of the American Heart Association. 2024: e034825.
|
| [14] |
Lee S, Cho GJ, Park GU, Kim LY, Lee TS, Kim DY, Choi SW, Youn JC, Han SW, Ryu KH, Na JO, Choi CU, Seo HS, Kim EJ. Incidence, Risk Factors, and Clinical Characteristics of Peripartum Cardiomyopathy in South Korea. Circ Heart Fail. 2018 Apr; 11(4): e004134.
|
| [15] |
Gentry MB, Dias JK, Luis A, Patel R, Thornton J, Reed GL. African-American women have a higher risk for developing peripartum cardiomyopathy. Journal of the American College of Cardiology. 2010; 55(7): 654-9.
|
| [16] |
Lee S, Cho GJ, Park GU, Kim LY, Lee T-S, Kim DY, et al. Incidence, risk factors, and clinical characteristics of peripartum cardiomyopathy in South Korea. Circulation: Heart Failure. 2018; 11(4): e004134.
|
| [17] |
Huang G, Zhang L, Long-Le M, Le-Xin W. Clinical characteristics and risk factors for peripartum cardiomyopathy. African health sciences. 2012; 12(1): 26-31.
|
| [18] |
Lampert MB, Hibbard J, Weinert L, Briller J, Lindheimer M, Lang RM. Peripartum heart failure associated with prolonged tocolytic therapy. American journal of obstetrics and gynecology. 1993; 168(2): 493-5.
|
| [19] |
Karaye KM, Ishaq N, Sa'idu H, Balarabe S, Talle M, Isa M, et al. Incidence, clinical characteristics, and risk factors for peripartum cardiomyopathy in Nigeria: results from the PEACE Registry. ESC heart failure. 2020; 7(1): 236-44.
|
| [20] |
Mengistu MD, Benti H. Assessment of magnitude and spectrum of cardiovascular disease admissions and outcomes in Saint Paul Hospital Millennium Medical College, Addis Ababa: A retrospective study. Plos one. 2022; 17(12): e0267527.
|
| [21] |
Zeru AB, Muluneh MA. Admission and inpatient mortality of hypertension complications in Addis Ababa. Integrated Blood Pressure Control. 2020: 103-10.
|
| [22] |
Abdissa SG, Oli K, Feleke Y, Goshu DY, Begna DM, Tafese A. Spectrum of cardiovascular diseases among Ethiopian patients at Tikur Anbessa specialized university teaching hospital, Addis Ababa. Ethiop medj. 2014; 52(1): 9-17.
|
| [23] |
Ntusi NB, Mayosi BM. Etiology and risk factors for peripartum cardiomyopathy: a systematic review. International journal of cardiology. 2009; 131(2): 168-79.
|
| [24] |
Arbelo E, Protonotarios A, Gimeno JR, Arbustini E, Barriales-Villa R, Basso C, et al. 2023 ESC Guidelines for the management of cardiomyopathies: Developed by the task force on the management of cardiomyopathies of the European Society of Cardiology [ESC]. European heart journal. 2023; 44(37): 3503-626.
|
| [25] |
Bauersachs J, König T, van der Meer P, Petrie MC, Hilfiker-Kleiner D, Mbakwem A, et al. Pathophysiology, diagnosis and management of peripartum cardiomyopathy: a position statement from the Heart Failure Association of the European Society of Cardiology Study Group on peripartum cardiomyopathy. European journal of heart failure. 2019; 21(7): 827-43.
|
| [26] |
ARSLAN CD. The Effects of Reproductive Right Policies on Women’s Experience of Egg and Embryo Freezing Process in Turkey: Middle East Technical University; 2022.
|
| [27] |
Bakketeig LS, Jacobsen G, Hoffman HJ, Lindmark G, Bergsjø P, Molne K, et al. Pre-pregnancy risk factors for small-for-gestational age births among parous women in Scandinavia. Acta obstetricia et gynecologica Scandinavica. 1993; 72(4): 273-9.
|
| [28] |
Lakshminarasimhappa M. Web-based and smart mobile app for data collection: Kobo Toolbox/Kobo collect. Journal of Indian Library Association Now Available at
https://journalilaindianet/
2022; 57(2): 72-9.
|
| [29] |
Kasper EK, Agema WR, Hutchins GM, Deckers JW, Hare JM, Baughman KL. The causes of dilated cardiomyopathy: a clinicopathologic review of 673 consecutive patients. Journal of the American College of Cardiology. 1994; 23(3): 586-90.
|
| [30] |
Felker GM, Thompson RE, Hare JM, Hruban RH, Clemetson DE, Howard DL, et al. Underlying causes and long-term survival in patients with initially unexplained cardiomyopathy. New England Journal of Medicine. 2000; 342(15): 1077-84.
|
| [31] |
Mbakwem AC, Amadi CE, Ajuluchukwu JN, Kushimo OA. Trends and outcomes of cardiovascular disease admissions in Lagos, Nigeria: a 16-year review. Cardiovascular Journal of Africa. 2023; 34(3): 140-8.
|
| [32] |
Karaye K, Sani M. The impact of income on the echocardiographic pattern of heart diseases in Kano, Nigeria. Nigerian Journal of Medicine. 2008; 17(3): 350-5.
|
| [33] |
Gunderson EP, Croen LA, Chiang V, Yoshida CK, Walton D, Go AS. Epidemiology of peripartum cardiomyopathy: incidence, predictors, and outcomes. Obstetrics & Gynecology. 2011; 118(3): 583-91.
|
Cite This Article
-
APA Style
Hayle, E. B., Biabeyn, A. M., Zewde, W. Z., Taye, B. T., Abebe, E. G., et al. (2025). Prevalence and Risk Factors of Peripartum Cardiomyopathy Among Reproductive-Aged Women with Dilated Cardiomyopathy in Ethiopia: A Cross-Sectional Study. International Journal of Cardiovascular and Thoracic Surgery, 11(3), 31-40. https://doi.org/10.11648/j.ijcts.20251103.12
 Copy
|
Copy
|
 Download
Download
ACS Style
Hayle, E. B.; Biabeyn, A. M.; Zewde, W. Z.; Taye, B. T.; Abebe, E. G., et al. Prevalence and Risk Factors of Peripartum Cardiomyopathy Among Reproductive-Aged Women with Dilated Cardiomyopathy in Ethiopia: A Cross-Sectional Study. Int. J. Cardiovasc. Thorac. Surg. 2025, 11(3), 31-40. doi: 10.11648/j.ijcts.20251103.12
Copy
|
Download
AMA Style
Hayle EB, Biabeyn AM, Zewde WZ, Taye BT, Abebe EG, et al. Prevalence and Risk Factors of Peripartum Cardiomyopathy Among Reproductive-Aged Women with Dilated Cardiomyopathy in Ethiopia: A Cross-Sectional Study. Int J Cardiovasc Thorac Surg. 2025;11(3):31-40. doi: 10.11648/j.ijcts.20251103.12
Copy
|
Download
-
@article{10.11648/j.ijcts.20251103.12,
author = {Ermiyas Berehanu Hayle and Adane Mamo Biabeyn and Wasihun Zerfu Zewde and Besufekad Tesfu Taye and Eyerusalem Girma Abebe and Amsalu Alem Bahre and Tsion Habtamu Ababiya and Abel Tesfaye Moges and Asfaw Hagos Shumye and Asefa Adimasu Taddese},
title = {Prevalence and Risk Factors of Peripartum Cardiomyopathy Among Reproductive-Aged Women with Dilated Cardiomyopathy in Ethiopia: A Cross-Sectional Study
},
journal = {International Journal of Cardiovascular and Thoracic Surgery},
volume = {11},
number = {3},
pages = {31-40},
doi = {10.11648/j.ijcts.20251103.12},
url = {https://doi.org/10.11648/j.ijcts.20251103.12},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ijcts.20251103.12},
abstract = {Background: Peripartum cardiomyopathy causes dilated cardiomyopathy, which develops late in pregnancy or early after childbirth and primarily affects African women. Patients frequently experience more frequent partial or complete recovery than patients with other forms of dilated cardiomyopathy do, emphasizing the crucial role of early diagnosis and management. Despite its global prevalence, there is currently a lack of comprehensive data on the disease's impact and contributing factors in Ethiopia. This study aimed to assess the prevalence of peripartum cardiomyopathy and its associated factors among reproductive-aged women with dilated cardiomyopathy who were hospitalized or on cardiac follow-up at three tertiary hospitals in Addis Ababa, Ethiopia. Methods: An institution-based cross-sectional study was conducted via a universal sampling method at three hospitals. Medical records of reproductive-aged women with Dilated cardiomyopathies that were hospitalized or attended follow-up from October 2021 to September 2023 at the three hospitals were reviewed. Both descriptive and analytical statistical methods were employed via SPSS version 29 for analysis, with the significance level set at a p value Results: Three hundred four women of reproductive age with dilated cardiomyopathy participated. The prevalence of peripartum cardiomyopathy was 22.7%. Bivariate and multiple logistic regression analyses revealed that preeclampsia [AOR 13.740, 95% CI 1.120--168.509], multiparty [AOR 6.01, 95% CI 1.91--18.93], gestational diabetes [AOR 10.95, 95% CI 1.62--74.09], pregnancy-related anemia [AOR 4.55, 95% CI 1.47--14.09], low socioeconomic status [AOR 6.83, 95% CI 2.06--22.68], and alcohol consumption during pregnancy [AOR 18.98, 95% CI 5.15--70.03] were significantly associated with an increased risk of peripartum cardiomyopathy. Conclusion: Peripartum cardiomyopathy is a common form of dilated cardiomyopathy in women of reproductive age. Its association with multiple demographic and obstetric risk factors highlights the need for improved risk assessment and further research. Clinical trial number: not applicable},
year = {2025}
}
Copy
|
Download
-
TY - JOUR
T1 - Prevalence and Risk Factors of Peripartum Cardiomyopathy Among Reproductive-Aged Women with Dilated Cardiomyopathy in Ethiopia: A Cross-Sectional Study
AU - Ermiyas Berehanu Hayle
AU - Adane Mamo Biabeyn
AU - Wasihun Zerfu Zewde
AU - Besufekad Tesfu Taye
AU - Eyerusalem Girma Abebe
AU - Amsalu Alem Bahre
AU - Tsion Habtamu Ababiya
AU - Abel Tesfaye Moges
AU - Asfaw Hagos Shumye
AU - Asefa Adimasu Taddese
Y1 - 2025/07/04
PY - 2025
N1 - https://doi.org/10.11648/j.ijcts.20251103.12
DO - 10.11648/j.ijcts.20251103.12
T2 - International Journal of Cardiovascular and Thoracic Surgery
JF - International Journal of Cardiovascular and Thoracic Surgery
JO - International Journal of Cardiovascular and Thoracic Surgery
SP - 31
EP - 40
PB - Science Publishing Group
SN - 2575-4882
UR - https://doi.org/10.11648/j.ijcts.20251103.12
AB - Background: Peripartum cardiomyopathy causes dilated cardiomyopathy, which develops late in pregnancy or early after childbirth and primarily affects African women. Patients frequently experience more frequent partial or complete recovery than patients with other forms of dilated cardiomyopathy do, emphasizing the crucial role of early diagnosis and management. Despite its global prevalence, there is currently a lack of comprehensive data on the disease's impact and contributing factors in Ethiopia. This study aimed to assess the prevalence of peripartum cardiomyopathy and its associated factors among reproductive-aged women with dilated cardiomyopathy who were hospitalized or on cardiac follow-up at three tertiary hospitals in Addis Ababa, Ethiopia. Methods: An institution-based cross-sectional study was conducted via a universal sampling method at three hospitals. Medical records of reproductive-aged women with Dilated cardiomyopathies that were hospitalized or attended follow-up from October 2021 to September 2023 at the three hospitals were reviewed. Both descriptive and analytical statistical methods were employed via SPSS version 29 for analysis, with the significance level set at a p value Results: Three hundred four women of reproductive age with dilated cardiomyopathy participated. The prevalence of peripartum cardiomyopathy was 22.7%. Bivariate and multiple logistic regression analyses revealed that preeclampsia [AOR 13.740, 95% CI 1.120--168.509], multiparty [AOR 6.01, 95% CI 1.91--18.93], gestational diabetes [AOR 10.95, 95% CI 1.62--74.09], pregnancy-related anemia [AOR 4.55, 95% CI 1.47--14.09], low socioeconomic status [AOR 6.83, 95% CI 2.06--22.68], and alcohol consumption during pregnancy [AOR 18.98, 95% CI 5.15--70.03] were significantly associated with an increased risk of peripartum cardiomyopathy. Conclusion: Peripartum cardiomyopathy is a common form of dilated cardiomyopathy in women of reproductive age. Its association with multiple demographic and obstetric risk factors highlights the need for improved risk assessment and further research. Clinical trial number: not applicable
VL - 11
IS - 3
ER -
Copy
|
Download