Perioperative cyanotic spells in Tetralogy of Fallot (TOF) patients during the initiation of surgery can lead to profound desaturation & hemodynamic unstability. These spells are characterized by acute desaturation due to increased right-to-left shunting, often triggered by anesthesia induction, stress, or changes in vascular resistance. In severe cases, standard medical management—including fluid boluses, vasopressors, and beta-blockers—may fail, necessitating urgent intervention to restore pulmonary blood flow or put patient immediately on cardiopulmonary bypass (CPB). We encountered such a scenario in a 5-year-old child scheduled for total correction of TOF. Preoperative imaging had revealed good-sized branch pulmonary arteries but significant right ventricular outflow tract (RVOT) obstruction at valvular level. Two large major aortopulmonary collateral arteries (MAPCAs) had been coiled preoperatively. During anesthesia induction, the child developed a severe cyanotic spell perioperatively, with saturations progressively dropping below 20%. Despite aggressive conventional management, including oxygenation, deep sedation, and vasoactive support, the spell remained refractory, and the patient’s condition deteriorated rapidly. These measures failed to improve oxygenation, and decision was taken to immediately put patient on CPB.Recognizing the urgency, we immediately performed an emergency sternotomy to put patient on CPB, but as setting up CPB would take several minutes, meanwhile we also tried to stabilise the child by rapidly restore pulmonary circulation with our innovative novel Two IV Cannula technique: inserting a 14F IV cannula into the ascending aorta and another 14F IV cannula into the distal pulmonary artery, then connecting them with a standard IV tubing connector. This setup created a temporary aorto-pulmonary shunt within few seconds, functionally resembling a Blalock-Taussig-Thomas (BTT) shunt, allowing blood to bypass the obstructed outflow tract and directly perfuse the pulmonary circulation. This simple yet life-saving maneuver resulted in an immediate and dramatic improvement in oxygenation/saturation within few seconds, providing crucial time for controlled CPB initiation. Within seconds, the patient’s oxygen saturation improved dramatically from 20% to 70%, and hemodynamic stability was restored and allowing a controlled transition to CPB. This rapid stabilization technique using IV cannula in perioperative spelling child provided crucial time for CPB initiation under controlled conditions. The IV cannulas were then removed, and the total correction was successfully performed with a transannular patch. This simple, easily replicable & innovative Two IV cannulas technique offers a life-saving bridge to CPB in cases of refractory cyanotic spells. It is easy to implement, requires minimal equipment, achieved in few seconds and can be performed by an assistant while the primary surgeon continues with CPB cannulation. This approach may be especially useful in resource-limited settings & serves as an effective interim measure to stabilize the patient until bypass is established.
| Published in | International Journal of Cardiovascular and Thoracic Surgery (Volume 11, Issue 2) |
| DOI | 10.11648/j.ijcts.20251102.11 |
| Page(s) | 13-17 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2025. Published by Science Publishing Group |
Tetralogy of Fallot, Cyanotic Spell, Emergency Aorto-pulmonary Shunt, IV Cannula Technique, Pediatric Cardiac Surgery
Intervention | Time to Effect | Equipment Required | Feasibility in Emergency |
|---|---|---|---|
IV Cannula Aorto-Pulmonary Shunt (Two IV Cannulas Technique) | Few seconds | 2 IV cannulas & connector | Highly feasible. This can done by assistant also while main surgeon can continue in process of establishing CPB. |
Blalock-Taussig-Thomas (BTT) Shunt | 30–60 minutes | Graft, sutures | An emergency measure but take time. |
CPB Initiation | 5–10 minutes | CPB machine, cannulation | Time-consuming in beginners' hands. |
CPB | Cardio Pulmonary Bypass |
IV | Intravenous Cannula |
MAPCAs | Major Aorta Pulmonary Collaterals |
TOF | Tetrology of Fallot |
VSD | Ventricular Septal Defect |
RVOT | Right Ventricular Outflow Tract |
| [1] | Apitz C, Webb GD, Redington AN. Tetralogy of Fallot. Lancet. 2009; 374(9699): 1462-71. |
| [2] | Hoffman JI. Incidence of congenital heart disease: II. Pediatr Cardiol. 1995; 16(2): 103-13. |
| [3] | Andropoulos DB, et al. Anesthesia for congenital heart disease. J Cardiothorac Vasc Anesth. 2012; 26(5): 865-72. |
| [4] | St-Pierre SM, Béland MJ. Management of cyanotic spells in TOF. Cardiol Young. 2018; 28(8): 1132-9. |
| [5] | Rao PS. Management of TOF. Curr Cardiol Rep. 2019; 21(6): 58. |
| [6] | Jonas RA. Surgical Management of Congenital Heart Disease. CRC Press; 2014. |
| [7] | Bertranou EG, Blackstone EH, Hazelrig JB, Turner ME, Kirklin JW. Life expectancy without surgery in tetralogy of Fallot. Am J Cardiol. 1978; 42(3): 458-66. |
| [8] | Mahle WT, Pasquali SK, Wernovsky G, et al. Neonatal and early surgical management of tetralogy of Fallot. Semin Thorac Cardiovasc Surg Pediatr Card Surg Annu. 2011; 14(1): 39-45. |
| [9] | Turley K, Bonchek LI, Orsmond GS, et al. Emergency management of tetralogy of Fallot spells: a surgical perspective. Ann Thorac Surg. 1976; 22(4): 337-42. |
| [10] | Van Praagh R. The first mention of Tetralogy of Fallot (1888) and its first illustration (1798). Pediatr Cardiol. 1989; 10(3): 202-5. |
| [11] | Murphy JG, Gersh BJ, McGoon MD, et al. Long-term outcome in patients undergoing surgical repair of tetralogy of Fallot. N Engl J Med. 1993; 329(9): 593-9. |
| [12] | Hickey EJ, Caldarone CA, McCrindle BW. Left ventricular assessment and function in TOF repair: impact on outcomes. Circulation. 2009; 119(3): 445-51. |
| [13] | Shunt MA, Ehsan A, McElhinney DB, et al. Modified Blalock-Taussig shunt: risk factors and outcomes. Ann Thorac Surg. 2008; 86(3): 873-81. |
| [14] | Murtuza B, Sullivan ID, Brawn WJ, et al. Surgical management of Tetralogy of Fallot with major collaterals: outcomes and challenges. Ann Thorac Surg. 2011; 91(3): 823-30. |
| [15] | Kirklin JK, Blackstone EH, Jonas RA, et al. Intermediate outcomes after repair of Tetralogy of Fallot: risk stratification in the modern era. J Thorac Cardiovasc Surg. 2003; 126(3): 679-89. |
| [16] | Tweddell JS, Nersesian M, Mussatto KA, et al. Current approaches to management of tetralogy of Fallot: a single-institution review of 30 years and 1065 patients. Ann Thorac Surg. 2002; 74(1): 156-61. |
APA Style
Singh, A., Sharma, P., Malhotra, V., Sharma, V. (2025). Emergency Aorto-Pulmonary Shunt Using Two IV Cannulas Technique: A Rapid Stabilization Technique for Cyanotic Spells in Tetralogy of Fallot Before Cardiopulmonary Bypass. International Journal of Cardiovascular and Thoracic Surgery, 11(2), 13-17. https://doi.org/10.11648/j.ijcts.20251102.11
ACS Style
Singh, A.; Sharma, P.; Malhotra, V.; Sharma, V. Emergency Aorto-Pulmonary Shunt Using Two IV Cannulas Technique: A Rapid Stabilization Technique for Cyanotic Spells in Tetralogy of Fallot Before Cardiopulmonary Bypass. Int. J. Cardiovasc. Thorac. Surg. 2025, 11(2), 13-17. doi: 10.11648/j.ijcts.20251102.11
AMA Style
Singh A, Sharma P, Malhotra V, Sharma V. Emergency Aorto-Pulmonary Shunt Using Two IV Cannulas Technique: A Rapid Stabilization Technique for Cyanotic Spells in Tetralogy of Fallot Before Cardiopulmonary Bypass. Int J Cardiovasc Thorac Surg. 2025;11(2):13-17. doi: 10.11648/j.ijcts.20251102.11
@article{10.11648/j.ijcts.20251102.11,
author = {Ajit Singh and Puneet Sharma and Vinay Malhotra and Vishesh Sharma},
title = {Emergency Aorto-Pulmonary Shunt Using Two IV Cannulas Technique: A Rapid Stabilization Technique for Cyanotic Spells in Tetralogy of Fallot Before Cardiopulmonary Bypass},
journal = {International Journal of Cardiovascular and Thoracic Surgery},
volume = {11},
number = {2},
pages = {13-17},
doi = {10.11648/j.ijcts.20251102.11},
url = {https://doi.org/10.11648/j.ijcts.20251102.11},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ijcts.20251102.11},
abstract = {Perioperative cyanotic spells in Tetralogy of Fallot (TOF) patients during the initiation of surgery can lead to profound desaturation & hemodynamic unstability. These spells are characterized by acute desaturation due to increased right-to-left shunting, often triggered by anesthesia induction, stress, or changes in vascular resistance. In severe cases, standard medical management—including fluid boluses, vasopressors, and beta-blockers—may fail, necessitating urgent intervention to restore pulmonary blood flow or put patient immediately on cardiopulmonary bypass (CPB). We encountered such a scenario in a 5-year-old child scheduled for total correction of TOF. Preoperative imaging had revealed good-sized branch pulmonary arteries but significant right ventricular outflow tract (RVOT) obstruction at valvular level. Two large major aortopulmonary collateral arteries (MAPCAs) had been coiled preoperatively. During anesthesia induction, the child developed a severe cyanotic spell perioperatively, with saturations progressively dropping below 20%. Despite aggressive conventional management, including oxygenation, deep sedation, and vasoactive support, the spell remained refractory, and the patient’s condition deteriorated rapidly. These measures failed to improve oxygenation, and decision was taken to immediately put patient on CPB.Recognizing the urgency, we immediately performed an emergency sternotomy to put patient on CPB, but as setting up CPB would take several minutes, meanwhile we also tried to stabilise the child by rapidly restore pulmonary circulation with our innovative novel Two IV Cannula technique: inserting a 14F IV cannula into the ascending aorta and another 14F IV cannula into the distal pulmonary artery, then connecting them with a standard IV tubing connector. This setup created a temporary aorto-pulmonary shunt within few seconds, functionally resembling a Blalock-Taussig-Thomas (BTT) shunt, allowing blood to bypass the obstructed outflow tract and directly perfuse the pulmonary circulation. This simple yet life-saving maneuver resulted in an immediate and dramatic improvement in oxygenation/saturation within few seconds, providing crucial time for controlled CPB initiation. Within seconds, the patient’s oxygen saturation improved dramatically from 20% to 70%, and hemodynamic stability was restored and allowing a controlled transition to CPB. This rapid stabilization technique using IV cannula in perioperative spelling child provided crucial time for CPB initiation under controlled conditions. The IV cannulas were then removed, and the total correction was successfully performed with a transannular patch. This simple, easily replicable & innovative Two IV cannulas technique offers a life-saving bridge to CPB in cases of refractory cyanotic spells. It is easy to implement, requires minimal equipment, achieved in few seconds and can be performed by an assistant while the primary surgeon continues with CPB cannulation. This approach may be especially useful in resource-limited settings & serves as an effective interim measure to stabilize the patient until bypass is established.},
year = {2025}
}
TY - JOUR T1 - Emergency Aorto-Pulmonary Shunt Using Two IV Cannulas Technique: A Rapid Stabilization Technique for Cyanotic Spells in Tetralogy of Fallot Before Cardiopulmonary Bypass AU - Ajit Singh AU - Puneet Sharma AU - Vinay Malhotra AU - Vishesh Sharma Y1 - 2025/03/26 PY - 2025 N1 - https://doi.org/10.11648/j.ijcts.20251102.11 DO - 10.11648/j.ijcts.20251102.11 T2 - International Journal of Cardiovascular and Thoracic Surgery JF - International Journal of Cardiovascular and Thoracic Surgery JO - International Journal of Cardiovascular and Thoracic Surgery SP - 13 EP - 17 PB - Science Publishing Group SN - 2575-4882 UR - https://doi.org/10.11648/j.ijcts.20251102.11 AB - Perioperative cyanotic spells in Tetralogy of Fallot (TOF) patients during the initiation of surgery can lead to profound desaturation & hemodynamic unstability. These spells are characterized by acute desaturation due to increased right-to-left shunting, often triggered by anesthesia induction, stress, or changes in vascular resistance. In severe cases, standard medical management—including fluid boluses, vasopressors, and beta-blockers—may fail, necessitating urgent intervention to restore pulmonary blood flow or put patient immediately on cardiopulmonary bypass (CPB). We encountered such a scenario in a 5-year-old child scheduled for total correction of TOF. Preoperative imaging had revealed good-sized branch pulmonary arteries but significant right ventricular outflow tract (RVOT) obstruction at valvular level. Two large major aortopulmonary collateral arteries (MAPCAs) had been coiled preoperatively. During anesthesia induction, the child developed a severe cyanotic spell perioperatively, with saturations progressively dropping below 20%. Despite aggressive conventional management, including oxygenation, deep sedation, and vasoactive support, the spell remained refractory, and the patient’s condition deteriorated rapidly. These measures failed to improve oxygenation, and decision was taken to immediately put patient on CPB.Recognizing the urgency, we immediately performed an emergency sternotomy to put patient on CPB, but as setting up CPB would take several minutes, meanwhile we also tried to stabilise the child by rapidly restore pulmonary circulation with our innovative novel Two IV Cannula technique: inserting a 14F IV cannula into the ascending aorta and another 14F IV cannula into the distal pulmonary artery, then connecting them with a standard IV tubing connector. This setup created a temporary aorto-pulmonary shunt within few seconds, functionally resembling a Blalock-Taussig-Thomas (BTT) shunt, allowing blood to bypass the obstructed outflow tract and directly perfuse the pulmonary circulation. This simple yet life-saving maneuver resulted in an immediate and dramatic improvement in oxygenation/saturation within few seconds, providing crucial time for controlled CPB initiation. Within seconds, the patient’s oxygen saturation improved dramatically from 20% to 70%, and hemodynamic stability was restored and allowing a controlled transition to CPB. This rapid stabilization technique using IV cannula in perioperative spelling child provided crucial time for CPB initiation under controlled conditions. The IV cannulas were then removed, and the total correction was successfully performed with a transannular patch. This simple, easily replicable & innovative Two IV cannulas technique offers a life-saving bridge to CPB in cases of refractory cyanotic spells. It is easy to implement, requires minimal equipment, achieved in few seconds and can be performed by an assistant while the primary surgeon continues with CPB cannulation. This approach may be especially useful in resource-limited settings & serves as an effective interim measure to stabilize the patient until bypass is established. VL - 11 IS - 2 ER -
Department of Cardiothoracic and Vascular Surgery, Vardhman Mahavir Medical College and Safdarjung Hospital, New Delhi, India
Department of Cardiothoracic and Vascular Surgery, RPGMC, Tanda, Himachal Pradesh, India
Department of Cardiothoracic and Vascular Surgery, Vardhman Mahavir Medical College and Safdarjung Hospital, New Delhi, India
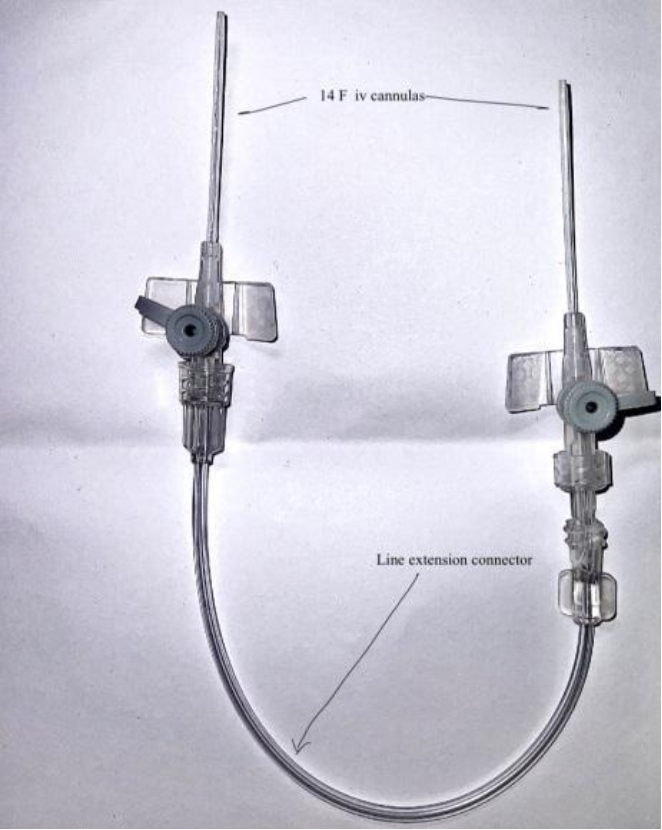
Figure 1. 14F IV cannulas with connector.
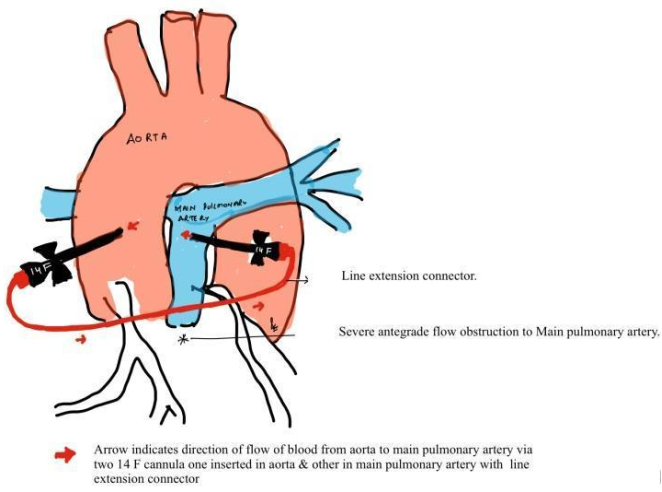
Figure 2. Schematic image representation of increasing pulmonary blood flow in case of intraoperative on table spelling child during induction of anasthesia before going on CPB using two cannulas with connector(Two IV Cannulas Technique). Note red arrow indicate direction of blood flow.
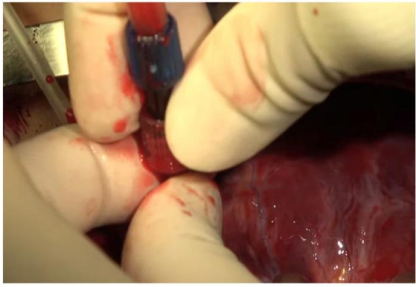
Figure 3. Intraopertive image showing surgeon (second assistant) quickly inserting two IV cannulas in intraoperative spelling child while main surgeon continues in establishing CPB.
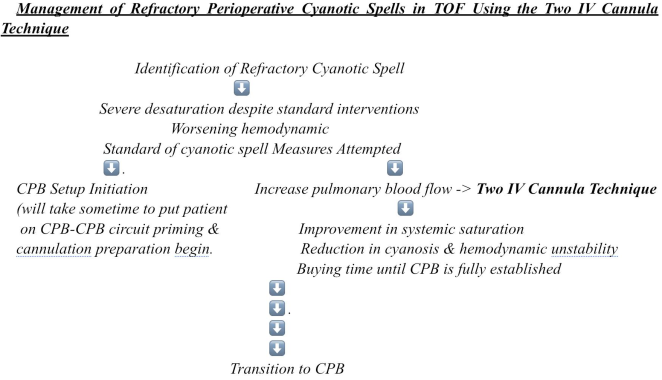
Figure 4. Flowchart of management of Refractory Perioperative Cyanotic Spells in TOF Using the Two IV Cannula Technique.
Information

