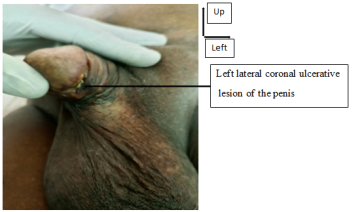
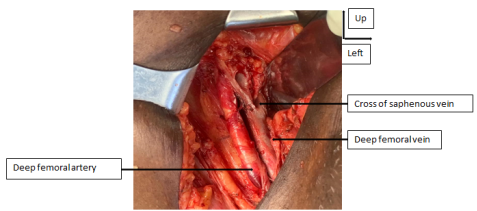
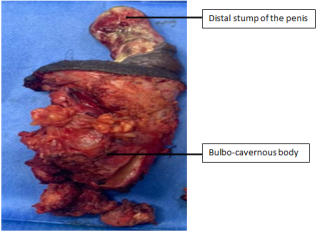
Aim: Penile cancer is one of the rarest urogenital cancers. Penile metastases after cystectomy are possible and seem to be associated with the existence of an extensive tumor on the surgical specimen. Case Presentation: We report here the case of old man 78 years old, with a history of Radical Cysto-Prostatectomy with Bricker type urinary diversion, indicated for a pT3N0M0R0 infiltrating urothelial carcinoma of the bladder. He had consulted 7 years post surgery for an indurated lesion of the penis with urethrorrhagia. On examination, he presented an ulcerative-necrotic lesion under the left lateral coronal area of the penis, a diffuse induration of corporal bodies from the glans to the bulb, bilateral inguinal macro lymphadenopathies. Magnetic Resonance Imaging of the penis suggested a tumor extending over the entire penis, infiltrating the corpora cavernosa and spongiosa, with invasion of the albuginea, adjacent fat and skin. In view of this picture, a total penectomy with emasculation was performed. The histology of the surgical specimen showed a poorly differentiated urothelial carcinoma with an immunohistochemical study in favor of a primary urothelial origin (GATA3+). The tumor infiltrated both corpora cavernosa and the urethra with positive margins of resection. The right inguinal lymph node dissection showed one metastatic node out of two. The left inguinal lymph node dissection showed one metastatic lymph node out of six with capsular rupture. Thoracic-abdominopelvic CT Scan showed a right inguinal adenopathy with no other lesions suggestive of secondary localization. The diagnosis of secondary urothelial carcinoma of the penis classified as pT4N2M0R1 was made and the patient underwent chemotherapy on tumor board meeting. Conclusion: Secondary cancers of the penis, although rare, can occur years after radical treatment of the primary tumor. Immuno-histochemestry was esential to differentiate from primary squamous cell carcinoma in our case.
| Published in | International Journal of Clinical Oncology and Cancer Research (Volume 9, Issue 2) |
| DOI | 10.11648/j.ijcocr.20240902.12 |
| Page(s) | 31-35 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2024. Published by Science Publishing Group |
Secondary Malignancy, Penile Caner, Bladder Cancer, Immuno-Histochemestry
| [1] | GLOBOCAN. Estimated number of new cases, worldwide. International Agency for Research on Cancer 2020. |
| [2] | LESOURD A. Anatomo-pathology of malignant penile tumours. Prog Urol 2005; 15 801-804. |
| [3] | MONDET F., MKAOUAR S., CHARTIER-KASTLER E, BITKER MO, DELCOURT A, RICHARD F. Cavernous metastases of bladder tumours after cystoprostatectomy. Prog Urol 2003; 13: 1330-1333. |
| [4] | SOW Y, THIAM A, FALL B, COULIBALI M, SARR A, DIAO B• ET AL. Penile cancer in Senegal: clinical and therapeutic aspects. Basic Clin. Androl. 2012; 22: 102–107. |
| [5] | SAVOIE PH, MOREL-JOURNEL N, MUREZ T, FERRETTI L, ROCHER L, FLECHON A. French ccAFU guidelines - update 2020-2022: penile cancer]. Prog Urol. 2020; 30(12S): S252-S279. |
| [6] | CARDOSO GUIMARÃES G, RODRIGUES DE SOUZA R, PAIVA GADELHA GUIMARÃES A, FILHO WD, VALESCHKA DE MATOS GRANJA N, KARAN KALIL R, ET AL. Penile metastasis of chondrosarcoma of the jaw. Urology. 2003; 61(4): 837. |
| [7] | PEREZ LM, SHUMWAY RA, CARSON CC, FISHER SR, HUDSON WR. Penile metastasis secondary to supraglottic squamous cell carcinoma: review of the literature. J Urol. 1992 Jan; 147(1): 157-60. |
| [8] | Ammani A, Alami E, Kasmaoui E. H, Bazine K, BEDDOUCH A ET LEZREK M. Penile metastases after cystoprostatectomy for urothelial carcinoma of the bladder. Afr J Urol 2009; 15(3): 214-219. |
| [9] | Touzani MA, Yddoussalah O. Cavernous metastasis from blader tumor]. Pan Afr Med J. 2017; 21(28): 60. |
| [10] | Bordeau KP, Lynch DF. Transitional cell carcinoma of the bladder metastatic to the penis. Urology. 2004; May; 63(5): 981-3. |
| [11] | GUEYE S. M, DIAGNE B. A, BA M. SYLLA C., MENSAH A. CANCER OF THE PENIS: EPIDEMIOLOGICAL ASPECTS AND THERAPEUTIC PROBLEMS IN SENEGAL. Médecine d'Afrique Noire: 1992, 39 (8/9). |
| [12] | DJE K, AVION KP, AKASSIMADOU N, COULIBALY N. Squamous cell carcinoma of the penis: a case report in an immunocompromised patient. Rev int sc méd -RISM-2017; 19(1): 85-87. |
| [13] | GUIRASSY S, BAH OR, BAH I, BARRY MII, DIALLO A, DIALLO AB. Squamous cell carcinoma of the penis: a case report of 4 patients at the Urology Department of Conakry University Hospital. Uro’Andro 2018; 1(10): 470-73. |
APA Style
Thiapato, F. S., Amadou, D. T., Talib, T. J. A., Désiré, N. R., Hamidou, K. K., et al. (2024). A Secondary Urothelial Carcinoma of the Penis Diagnosed. International Journal of Clinical Oncology and Cancer Research, 9(2), 31-35. https://doi.org/10.11648/j.ijcocr.20240902.12
ACS Style
Thiapato, F. S.; Amadou, D. T.; Talib, T. J. A.; Désiré, N. R.; Hamidou, K. K., et al. A Secondary Urothelial Carcinoma of the Penis Diagnosed. Int. J. Clin. Oncol. Cancer Res. 2024, 9(2), 31-35. doi: 10.11648/j.ijcocr.20240902.12
AMA Style
Thiapato FS, Amadou DT, Talib TJA, Désiré NR, Hamidou KK, et al. A Secondary Urothelial Carcinoma of the Penis Diagnosed. Int J Clin Oncol Cancer Res. 2024;9(2):31-35. doi: 10.11648/j.ijcocr.20240902.12
@article{10.11648/j.ijcocr.20240902.12,
author = {Faye Samba Thiapato and Diallo Thierno Amadou and Thiam Jafar Abou Talib and Niang Rokhaya Désiré and Kikalulu Kiambote Hamidou and Dembele Mamadou and Jalloh Mohamed and Kane Racine and Niang Lamine},
title = {A Secondary Urothelial Carcinoma of the Penis Diagnosed
},
journal = {International Journal of Clinical Oncology and Cancer Research},
volume = {9},
number = {2},
pages = {31-35},
doi = {10.11648/j.ijcocr.20240902.12},
url = {https://doi.org/10.11648/j.ijcocr.20240902.12},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ijcocr.20240902.12},
abstract = {Aim: Penile cancer is one of the rarest urogenital cancers. Penile metastases after cystectomy are possible and seem to be associated with the existence of an extensive tumor on the surgical specimen. Case Presentation: We report here the case of old man 78 years old, with a history of Radical Cysto-Prostatectomy with Bricker type urinary diversion, indicated for a pT3N0M0R0 infiltrating urothelial carcinoma of the bladder. He had consulted 7 years post surgery for an indurated lesion of the penis with urethrorrhagia. On examination, he presented an ulcerative-necrotic lesion under the left lateral coronal area of the penis, a diffuse induration of corporal bodies from the glans to the bulb, bilateral inguinal macro lymphadenopathies. Magnetic Resonance Imaging of the penis suggested a tumor extending over the entire penis, infiltrating the corpora cavernosa and spongiosa, with invasion of the albuginea, adjacent fat and skin. In view of this picture, a total penectomy with emasculation was performed. The histology of the surgical specimen showed a poorly differentiated urothelial carcinoma with an immunohistochemical study in favor of a primary urothelial origin (GATA3+). The tumor infiltrated both corpora cavernosa and the urethra with positive margins of resection. The right inguinal lymph node dissection showed one metastatic node out of two. The left inguinal lymph node dissection showed one metastatic lymph node out of six with capsular rupture. Thoracic-abdominopelvic CT Scan showed a right inguinal adenopathy with no other lesions suggestive of secondary localization. The diagnosis of secondary urothelial carcinoma of the penis classified as pT4N2M0R1 was made and the patient underwent chemotherapy on tumor board meeting. Conclusion: Secondary cancers of the penis, although rare, can occur years after radical treatment of the primary tumor. Immuno-histochemestry was esential to differentiate from primary squamous cell carcinoma in our case.
},
year = {2024}
}
TY - JOUR T1 - A Secondary Urothelial Carcinoma of the Penis Diagnosed AU - Faye Samba Thiapato AU - Diallo Thierno Amadou AU - Thiam Jafar Abou Talib AU - Niang Rokhaya Désiré AU - Kikalulu Kiambote Hamidou AU - Dembele Mamadou AU - Jalloh Mohamed AU - Kane Racine AU - Niang Lamine Y1 - 2024/04/28 PY - 2024 N1 - https://doi.org/10.11648/j.ijcocr.20240902.12 DO - 10.11648/j.ijcocr.20240902.12 T2 - International Journal of Clinical Oncology and Cancer Research JF - International Journal of Clinical Oncology and Cancer Research JO - International Journal of Clinical Oncology and Cancer Research SP - 31 EP - 35 PB - Science Publishing Group SN - 2578-9511 UR - https://doi.org/10.11648/j.ijcocr.20240902.12 AB - Aim: Penile cancer is one of the rarest urogenital cancers. Penile metastases after cystectomy are possible and seem to be associated with the existence of an extensive tumor on the surgical specimen. Case Presentation: We report here the case of old man 78 years old, with a history of Radical Cysto-Prostatectomy with Bricker type urinary diversion, indicated for a pT3N0M0R0 infiltrating urothelial carcinoma of the bladder. He had consulted 7 years post surgery for an indurated lesion of the penis with urethrorrhagia. On examination, he presented an ulcerative-necrotic lesion under the left lateral coronal area of the penis, a diffuse induration of corporal bodies from the glans to the bulb, bilateral inguinal macro lymphadenopathies. Magnetic Resonance Imaging of the penis suggested a tumor extending over the entire penis, infiltrating the corpora cavernosa and spongiosa, with invasion of the albuginea, adjacent fat and skin. In view of this picture, a total penectomy with emasculation was performed. The histology of the surgical specimen showed a poorly differentiated urothelial carcinoma with an immunohistochemical study in favor of a primary urothelial origin (GATA3+). The tumor infiltrated both corpora cavernosa and the urethra with positive margins of resection. The right inguinal lymph node dissection showed one metastatic node out of two. The left inguinal lymph node dissection showed one metastatic lymph node out of six with capsular rupture. Thoracic-abdominopelvic CT Scan showed a right inguinal adenopathy with no other lesions suggestive of secondary localization. The diagnosis of secondary urothelial carcinoma of the penis classified as pT4N2M0R1 was made and the patient underwent chemotherapy on tumor board meeting. Conclusion: Secondary cancers of the penis, although rare, can occur years after radical treatment of the primary tumor. Immuno-histochemestry was esential to differentiate from primary squamous cell carcinoma in our case. VL - 9 IS - 2 ER -
Urology Department, Principal Main Hospital of Dakar, Dakar, Senegal
Research Fields: oncology, lithiasis, prostate, bladder, kidney, Erevtile dysfonction
Urology Department, Idrissa POUYE General Hospital, Dakar, Senegal; Department of Surgery and Surgical Specialties, Faculty of Medicine, Pharmacy and Odontology of Cheikh Anta Diop University of Dakar, Dakar, Senegal
Research Fields: Recronstructive Urology, Endourology, Prostate Cancer, Bladder cancer, HBP, Lithiasis
Information