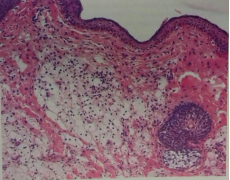
Eruptive xanthomas are most often the result of impaired lipid metabolism. They can be caused by a primary dysregulation in lipid metabolism (familial hyperlipoproteinemias) or by an increase in serum lipids from concomitant diseases (diabetes mellitus, obesity, chronic renal failure, nephrotic syndrome, pancreatitis, hypothyroidism, rarely hyperthyroidism, alcohol abuse, cholestasis or biliary cirrhosis, monoclonal gammopathy, multiple myeloma and leukemia) or from the use of certain medications (beta-blockers, estrogens, retinoids, protease inhibitors, cyclosporine, the antimycotic Miconazole and the antipsychotic Olanzapine (secondary hyperlipoproteinemias). Early diagnosis and adequate therapy of the skin changes and the comorbid underlying disease prevent serious life-threatening complications. A case of a 34-year-old man with papular yellowish lesions on the elbows is presented. The patient has accompanying diseases of diabetes mellitus, alcohol addiction, liver cirrhosis, chronic acute pancreatitis and chronic cholecystitis. The clinical diagnosis of eruptive xanthomas was confirmed by histopathological examination revealing foam cells in the dermis. Laboratory blood tests revealed an accelerated ESR and elevated blood glucose, transaminases, uric acid, total cholesterol, and triglycerides. Hepatoprotective and antidiabetic therapy combined with a dietary regimen improved the patient's condition and laboratory parameters. A partial reversal of skin lesions occurred. An overview of the epidemiology, etiopathogenesis, clinical picture, laboratory tests, differential diagnosis, dietary regimen, and treatment of eruptive xanthomas are presented.
| Published in | International Journal of Clinical Dermatology (Volume 7, Issue 1) |
| DOI | 10.11648/j.ijcd.20240701.15 |
| Page(s) | 24-29 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2024. Published by Science Publishing Group |
Eruptive Xanthomas, Chronic Alcohol Abuse, Dyslipidemia
AST | Aspartate Aminotransferase |
ALT | Alanine Aminotransferase |
GGT | GLUTAMYLTRANSFERASE |
HMG-CoA | β-Hydroxy β-methylglutaryl-CoA |
| [1] | Ahn CS, Yosipovitch G, Huang WW. Diabetes and the skin. In: Callen JP, Jorizzo JL, Zone JJ, Piette WW, Rosenbach MA, Vleugels RA, eds. Dermatological Signs of Systemic Disease. 5th ed. Philadelphia, PA: Elsevier; 2017: chap 24. |
| [2] | Braunstein I. Cutaneous manifestations of lipid disorders. In: Callen JP, Jorizzo JL, Zone JJ, Piette WW, Rosenbach MA, Vleugels RA, eds. Dermatological Signs of Systemic Disease. 5th ed. Philadelphia, PA: Elsevier; 2017: chap 26. |
| [3] | Fitzpatrick JE, High WA, Kyle WL. Yellow lesions. In: Fitzpatrick JE, High WA, Kyle WL, eds. Urgent Care Dermatology: Symptom-Based Diagnosis. Philadelphia, PA: Elsevier; 2018: chap 33. |
| [4] | McFarland J, McConnell G. Histologic studies of Xanthoma. J Med Res. 1904 Jul; 12(1): 69-74. |
| [5] | Brunzell JD. Clinical practice. Hypertriglyceridemia. N Engl J Med 2007; 357.10: 1009-1017. |
| [6] | Zaremba J, Zaczkiewicz A, Placek W. Eruptive xanthomas. Postepy Dermatol Alergol 2013; 30: 399–402. |
| [7] | Hegele RA, Ginsberg HN, Chapman MJ, et al. The polygenic nature of hypertriglyceridaemia: implications for definition, diagnosis, and management. Lancet Diabetes Endocrinol. 2014; 2: 655–666. |
| [8] | Roga G, Jithendriya M. Eruptive xanthoma: Warning sign of systemic disease. Cleve Clin J Med. 2016; 83(10): 715-716. |
| [9] | Marogi EP, Ohiomoba RO, Stone NJ. Eruptive Xanthomas: Importance of recognition to Reduce Delay of Effective Triglyceride Reduction. Am J Med. 2022; 135(4): 444-447. |
| [10] | Rigolon de Lara J, Momente Miquelin G, Lapins J, et al. Eruptive Xanthoma as a Sign of Underlaying Severe Metabolic Disorder. Dermatol Pract Concept. 2023; 13(1): e2023025. |
| [11] | Bell A, Shreenath AP. Xanthoma. StatPearls [Internet]. Last Update: August 28, 2023. |
| [12] | Parker F. Xanthomas and hyperlipidemias. J Am Acad Dermatol. 1985; 13(1): 1-30. |
| [13] | Caputo R, Monti M, Berti E, et al. Normolipemic eruptive cutaneous xanthomatosis. Arch Dermatol. 1986; 122(11): 1294-1297. |
| [14] | Wanat K., Noe Megan H. Cutaneous Xanthomas. UpToDate; 10 Nov. 2017. |
| [15] | Pouwels ED, Blom DJ, Firth JC, et al. Severe hypertriglyceridaemia as a result of familial chylomicronaemia: the Cape Town experience. S Afr Med J. 2008; 98(2): 105-108. |
| [16] | Ison HE, Clarke SL, Knowles JW. Familial Hypercholesterolemia. In: Adam MP, Feldman J, Mirzaa GM, Pagon RA, Wallace SE, Bean LJH, Gripp KW, Amemiya A, editors. GeneReviews® [Internet]. University of Washington, Seattle; Seattle (WA): Jan 2, 2014. |
| [17] | Mabuchi H. Half a Century Tales of Familial Hypercholesterolemia (FH) in Japan. J Atheroscler Thromb. 2017; 24(3): 189-207. |
| [18] | Roller E, Schulte KW, Hengge U, et al. Eruptive xanthomas. Hautarzt. 2004; 55(10): 978-980. |
| [19] | Quispe R, Hendrani AD, Baradaran-Noveiry B, et al. Characterization of lipoprotein profiles in patients with hypertriglyceridemic Fredrickson-Levy and Lees dyslipidemia phenotypes: the Very Large Database of Lipids Studies 6 and 7. Arch Med Sci. 2019; 15(5): 1195-1202. |
| [20] | Brunzell JD, Bierman EL. Chylomicronemia syndrome. Interaction of genetic and acquired hypertriglyceridemia. Med Clin North Am. 1982; 66(2): 455–468. |
| [21] | Leaf DA. Chylomicronemia and the chylomicronemia syndrome: a practical approach to management. Am J Med. 2008; 69(2): 105-108. |
| [22] | Goldberg RB, Chait A. A Comprehensive Update on the Chylomicronemia Syndrome. Front Endocrinol (Lausanne). 2020; 11: 593931. |
| [23] | Archer CB, MacDonald DM. Eruptive xanthomata in type V hyperlipoproteinemia associated with diabetes mellitus. Clin Exp Dermatol. 1984; 9(3): 312–316. |
| [24] | Zadak Z. Internist´s view on skin manifestations of hyperlipidemia in diabetic patients Vnitr Lek. 2006; 52(5): 465-469. |
| [25] | Zabeen B, Khaled Z, Nahar J, et al. Hypertriglyceridemia associated with eruptive xanthomas and lipemia retinalis in newly diagnosed diabetes mellitus. Mymensingh Med J. 2013; 22(3): 591-595. |
| [26] | Inoue-Nishimoto T, Hanafusa T, Hirohata A et al. Eruptive Xanthoma with Acute Pancreatitis in a Patient with Hypertriglyceridemia and Diabetes. Ann Dermatol. 2016; 28(1): 136-137. |
| [27] | Suzuki L, Hirayama S, Fukui M, et al. Lipoprotein-X in cholestatic patients causes xanthomas and promotes foam cell formation in human macrophages. J Clin Lipidol. 2017; 11(1): 110–118. |
| [28] | Lee SY, Sheth CA. Eruptive xanthoma associated with severe hypertriglyceridemia and poorly controlled type 1 diabetes mellitus. J Community Hosp Intern Med Perspect. 2019; 9(4): 344-346. |
| [29] | Harris J, Cao S, Hile G, et al. Diffuse xanthomas in a patient with primary biliary cholangitis and lipoprotein X. JAAD Case Rep. 2020; 7: 30–32. |
| [30] | Ladizinski B, Lee KC. Eruptive xanthomas in a patient with severe hypertriglyceridemia and type 2 diabetes. CMAJ. 2013; 185: 1600. |
| [31] | Jaber PW, Wilson B, Johns D, et al. Eruptive xanthomas during pregnancy. J Am Acad Dermatol. 1992; 27(2Pt2): 300-302. |
| [32] | Dicken CH, Connolly SM. Eruptive xanthomas associated with isotretinoin (13-cis-retinoic acid). Arch Dermatol. 1980; 116(8): 951-952. |
| [33] | Barr RJ, Fujita WH, Graham JH. Eruptive xanthomas associ ated with intravenous miconazole therapy. Arch Dermatol. 1978; 114(10): 1544-1545. |
| [34] | Chang HY, Ridky TW, Kimball AB, et al. Eruptive xan- thomas associated with olanzapine use. Arch Dermatol. 2003; 139(8): 1045-1048. |
| [35] | Roederer G, Xhignesse M, Davignon J. Eruptive and tubero- eruptive xanthomas of the skin arising on sites of prior injury. Two case reports. JAMA. 1988; 260(9): 1282-1283. |
| [36] | Eeckhout I, Vogelaers D, Geerts ML, et al. Xanthomas due to generalized oedema. Br J Dermatol. 1997; 136(4): 601-603. |
| [37] | Mai V, Akhondi H. Xanthomas: Differentiating atherogenic from nonatherogenic. Cleveland Clinic J Med. 2022; 89(8): 429-431. |
| [38] | Parker F. Normocholesterolemic xanthomatosis. Arch Derm tol. 1986; 122(11): 1253-1257. |
| [39] | Kashif M, Kumar H, Khaja M. An unusual presentation of eruptive xanthoma: A case report and literature review. Medicine (Baltimore). 2016; 95(37): e4866. |
| [40] |
Song X, Zhang D, Zhao Z, et al. Multiple Red-brown Papules and Plaques on the Trunk and Extremities: A Quiz. Acta Derm Venereol. 2023; 103: adv12419.
https://doi.org/10.2340/actadv.v103.12419 PMID: 37721357 |
| [41] | Brazzelli V, Rivetti N, Carugno A, et al. Eruptive xanthomas after extensive tattooing: a case report and literature review. G Ital Dermatol Venereol. 2015; 150(6): 770–1. |
| [42] | Gao H, Chen J. Eruptive xanthomas presenting in tattoos. CMAJ. 2015; 187(5): 356. |
| [43] | Cruz PD, East C, Bergstresser PR. Dermal, subcutaneous, and tendon xanthomas: diagnostic markers for specific lipoprotein disorders. J Am Acad Dermatol. 1988; 19(1 Pt 1): 95-111. |
| [44] | Patterson JW. Cutaneous infiltrates - nonlymphoid. In: Patterson JW, ed. Weedon's Skin Pathology. 5th ed. Philadelphia, PA: Elsevier; 2021: chap 41. |
| [45] | Rupec RA, Schaller M. Xanthoma disseminatum. Int J Derma tol 2002; 41: 911–913. |
| [46] | Cooper PH. Eruptive xanthoma: a microscopic simulant of granuloma annulare. J Cutan Pathol 1986; 13: 207–215. |
| [47] | Fagundes PP, Pinto AS, Pinto PA, et al. Eruptive xanthoma with unexpected granuloma annulare-like microscopic appearance: case report. An Bras Dermatol. 2009; 84(3): 289-292. |
| [48] | Hernandez-Martin A, Baselga E, Drolet BA, Esterly NB. Juvenile xanthogranuloma. J Am Acad Dermatol. 1997; 36((3 Pt 1)): 355–359. |
| [49] | Dehner LP. Juvenile xanthogranulomas in the first two decades of life: a clinicopathologic study of 174 cases with cutaneous and extracutaneous manifestations. Am J Surg Pathol. 2003; 27(5): 579–593. |
| [50] | Wang J, Wu X, Xi ZJ. Langerhans cell histiocytosis of bone in children: a clinicopathologic study of 108 cases. World J Pediatr. 2010; 6: 255–259. |
| [51] | Bito T, Kawakami C, Shimajiri S, et al. Generalized eruptive xanthoma with prominent deposition of naked chylomicrons: evidence for chylomicrons as the origin of urate-like crystals. J Cutan Pathol. 2010; 37(11): 1161-1163. |
| [52] | Jahr C, Vera V, Bustos R, et al. Diagnosis of pseudoxanthoma elasticum in a patient with discrete skin lesions. An Bras Dermatol. 2023; 98(4): 542–544. |
| [53] | Hamada T. Lipoid proteinosis. Clin Exp Dermatol. 2002 Nov; 27(8): 624-9. |
| [54] | Kim SM, Lee H, Kim YC. Eruptive Xanthoma With Dermal Mucin Deposition. Am J Dermatopathol. 2021; 43(8): 583-584. |
| [55] | Leung AKC, Barankin B, Hon KLE. Molluscum Contagiosum: An Update. Recent Pat Inflamm Allergy Drug Discov. 2017; 11(1): 22-31. |
| [56] | Yuan G, Al-Shali KZ, Hegele RA. Hypertriglyceridemia: its etiology, effects and treatment. CMAJ. 2007; 176(8): 1113–1120. |
| [57] | Ranjan N. Management of hyperlipidemias: an update. Indian J Dermatol Venereol Leprol. 2009; 75(5): 452–462. |
| [58] | White LE, Horenstein MG, Shea CR. Xanthomas. In: Lebwohl MG, Heymann WR, Coulson IH, Murrell DF, eds. Treatment of Skin Disease. 6th ed. Philadelphia, PA: Elsevier; 2022: chap 256.. |
| [59] | Nessel TA, Kerndt CC, Bills JA, et al. Eruptive xanthomas: a warning sign of future hyperlipidemia complications. Int J Res Dermatol. 2020; 6: 579–583. |
| [60] | Lind S, Olsson AG, Eriksson M, et al. Autosomal recessive hyper cholesterolaemia: normalization of plasma LDL cholesterol by ezetimibe in combination with statin treatment. Intern Med. 2004; 256(5): 406-412. |
| [61] | Thompson PD, Panza G, Zaleski A, et al. Statin-Associated Side Effects. J Am Coll Cardiol. 2016; 67(20): 2395-2410. |
APA Style
Darawish, B. E., Broshtilova, V., Yungareva, I., Smilov, N., Trenovski, A., et al. (2024). Eruptive Xanthomas – A Case Report with a Review of the Literature. International Journal of Clinical Dermatology, 7(1), 24-29. https://doi.org/10.11648/j.ijcd.20240701.15
ACS Style
Darawish, B. E.; Broshtilova, V.; Yungareva, I.; Smilov, N.; Trenovski, A., et al. Eruptive Xanthomas – A Case Report with a Review of the Literature. Int. J. Clin. Dermatol. 2024, 7(1), 24-29. doi: 10.11648/j.ijcd.20240701.15
AMA Style
Darawish BE, Broshtilova V, Yungareva I, Smilov N, Trenovski A, et al. Eruptive Xanthomas – A Case Report with a Review of the Literature. Int J Clin Dermatol. 2024;7(1):24-29. doi: 10.11648/j.ijcd.20240701.15
@article{10.11648/j.ijcd.20240701.15,
author = {Balkis El Darawish and Valentina Broshtilova and Irina Yungareva and Nencho Smilov and Aleksandar Trenovski and Yoanna Velevska and Sonya Marina},
title = {Eruptive Xanthomas – A Case Report with a Review of the Literature
},
journal = {International Journal of Clinical Dermatology},
volume = {7},
number = {1},
pages = {24-29},
doi = {10.11648/j.ijcd.20240701.15},
url = {https://doi.org/10.11648/j.ijcd.20240701.15},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ijcd.20240701.15},
abstract = {Eruptive xanthomas are most often the result of impaired lipid metabolism. They can be caused by a primary dysregulation in lipid metabolism (familial hyperlipoproteinemias) or by an increase in serum lipids from concomitant diseases (diabetes mellitus, obesity, chronic renal failure, nephrotic syndrome, pancreatitis, hypothyroidism, rarely hyperthyroidism, alcohol abuse, cholestasis or biliary cirrhosis, monoclonal gammopathy, multiple myeloma and leukemia) or from the use of certain medications (beta-blockers, estrogens, retinoids, protease inhibitors, cyclosporine, the antimycotic Miconazole and the antipsychotic Olanzapine (secondary hyperlipoproteinemias). Early diagnosis and adequate therapy of the skin changes and the comorbid underlying disease prevent serious life-threatening complications. A case of a 34-year-old man with papular yellowish lesions on the elbows is presented. The patient has accompanying diseases of diabetes mellitus, alcohol addiction, liver cirrhosis, chronic acute pancreatitis and chronic cholecystitis. The clinical diagnosis of eruptive xanthomas was confirmed by histopathological examination revealing foam cells in the dermis. Laboratory blood tests revealed an accelerated ESR and elevated blood glucose, transaminases, uric acid, total cholesterol, and triglycerides. Hepatoprotective and antidiabetic therapy combined with a dietary regimen improved the patient's condition and laboratory parameters. A partial reversal of skin lesions occurred. An overview of the epidemiology, etiopathogenesis, clinical picture, laboratory tests, differential diagnosis, dietary regimen, and treatment of eruptive xanthomas are presented.
},
year = {2024}
}
TY - JOUR T1 - Eruptive Xanthomas – A Case Report with a Review of the Literature AU - Balkis El Darawish AU - Valentina Broshtilova AU - Irina Yungareva AU - Nencho Smilov AU - Aleksandar Trenovski AU - Yoanna Velevska AU - Sonya Marina Y1 - 2024/05/30 PY - 2024 N1 - https://doi.org/10.11648/j.ijcd.20240701.15 DO - 10.11648/j.ijcd.20240701.15 T2 - International Journal of Clinical Dermatology JF - International Journal of Clinical Dermatology JO - International Journal of Clinical Dermatology SP - 24 EP - 29 PB - Science Publishing Group SN - 2995-1305 UR - https://doi.org/10.11648/j.ijcd.20240701.15 AB - Eruptive xanthomas are most often the result of impaired lipid metabolism. They can be caused by a primary dysregulation in lipid metabolism (familial hyperlipoproteinemias) or by an increase in serum lipids from concomitant diseases (diabetes mellitus, obesity, chronic renal failure, nephrotic syndrome, pancreatitis, hypothyroidism, rarely hyperthyroidism, alcohol abuse, cholestasis or biliary cirrhosis, monoclonal gammopathy, multiple myeloma and leukemia) or from the use of certain medications (beta-blockers, estrogens, retinoids, protease inhibitors, cyclosporine, the antimycotic Miconazole and the antipsychotic Olanzapine (secondary hyperlipoproteinemias). Early diagnosis and adequate therapy of the skin changes and the comorbid underlying disease prevent serious life-threatening complications. A case of a 34-year-old man with papular yellowish lesions on the elbows is presented. The patient has accompanying diseases of diabetes mellitus, alcohol addiction, liver cirrhosis, chronic acute pancreatitis and chronic cholecystitis. The clinical diagnosis of eruptive xanthomas was confirmed by histopathological examination revealing foam cells in the dermis. Laboratory blood tests revealed an accelerated ESR and elevated blood glucose, transaminases, uric acid, total cholesterol, and triglycerides. Hepatoprotective and antidiabetic therapy combined with a dietary regimen improved the patient's condition and laboratory parameters. A partial reversal of skin lesions occurred. An overview of the epidemiology, etiopathogenesis, clinical picture, laboratory tests, differential diagnosis, dietary regimen, and treatment of eruptive xanthomas are presented. VL - 7 IS - 1 ER -
Spectro - Institute of Medical Aesthetics, Sofia, Bulgaria
Department of Internal Medicine, Pharmacology and Clinical Pharmacology, Pediatrics, Epidemiology, Infectious Diseases and Dermatology, Faculty of Medicine, Sofia University, Sofia, Bulgaria
Department of Skin and Venereal Diseases, Medical Institute of the Ministry of Internal Affairs, Sofia, Bulgaria
Clinic of Urology, Medical Institute of the Ministry of Internal Affairs, Sofia, Bulgaria
Department of Anesthesiology and Intensive Care, Medical Institute of the Ministry of Internal Affairs, Sofia, Bulgaria
Department of Infectious Diseases, Parasitology and Dermatovenereology, Medical University, Varna, Bulgaria
Department of Skin and Venereal Diseases, Medical Institute of the Ministry of Internal Affairs, Sofia, Bulgaria
Information