Abstract
Background: Over the past three decades, infections following cesarean sections have increased markedly, with surgical site infections (SSIs) emerging as a leading cause of maternal morbidity and mortality. This issue is especially critical in low- and middle-income countries, including Ethiopia, where reliable data on the magnitude and determinants of post-cesarean infections remain limited. These infections contribute to prolonged hospital stays, higher healthcare costs, and elevated risks for both mothers and newborns. Objective: This study aimed to assess the prevalence of post-cesarean section infections and identify associated risk factors in selected hospitals in Addis Ababa, Ethiopia, in 2024. Methods: An institution-based retrospective cross-sectional study was conducted in selected hospitals between June 10 and August 30, 2024. A total of 472 medical records of women who underwent cesarean sections from January 1, 2019, through December 31, 2023, were reviewed using a systematic random sampling method. Hospitals were selected using simple random sampling. Data were entered and cleaned using Epi Info version 7.2.1.0 and analyzed with SPSS version 26. Binary logistic regression was employed to identify factors associated with post-cesarean infections. Adjusted odds ratios (AORs) with 95% confidence intervals (CIs) were calculated, and statistical significance was determined at a p-value < 0.05. Results: The prevalence of post-cesarean section infection was 17%. Key factors significantly associated with increased risk included: presence of clinical signs of infection (AOR = 4.37, 95% CI: 3.25-6.22), underlying co-morbid conditions (AOR = 4.72, 95% CI: 3.34-6.23), and operation duration longer than 30 minutes (AOR = 3.43, 95% CI: 2.32-4.43). Conclusion and Recommendation: The prevalence of post-cesarean infections in Addis Ababa was alarmingly high. Major risk factors included signs of infection, co-morbid illnesses, prolonged labor (>24 hours), previous cesarean deliveries, and extended operative time. To reduce infection rates, hospitals should enforce strict infection prevention protocols and maintain high standards of surgical practice.
Keywords
Surgical Site Infection, Cesarean Section, Risk Factors, Maternal Health, Addis Ababa, Ethiopia
1. Introduction
Cesarean section (CS) is one of the most frequently performed surgical procedures in obstetrics, involving the delivery of a fetus, placenta, and membranes through incisions in the abdominal and uterine walls, typically after 20 weeks of gestation
| [1] | Solomkin J, Kluytmans J, Alnaif B, et al. WHO global guidelines for the prevention of surgical site infection. Lancet Infect Dis. 2017; 17(3): 262-4. |
[1]
. While cesarean delivery can be lifesaving for both mother and child-particularly in cases of obstructed labor, fetal distress, or abnormal fetal presentations-it also carries significant risks when performed in settings lacking the necessary infrastructure for safe surgery and postoperative care
| [4] | World Health Organization. WHO Statement on Caesarean Section Rates. Geneva: WHO; 2015. |
| [5] | Mangram AJ, Horan TC, Pearson ML, Silver LC, Jarvis WR. Guideline for prevention of surgical site infection. Infect Control Hosp Epidemiol. 1999; 20: 250-78. |
[4, 5]
. Surgical site infections (SSIs), defined as infections occurring at or near a surgical incision within 30 days of the procedure (or up to one year if an implant is placed), are among the most common postoperative complications associated with CS
| [2] | Azeze GG, Bizuneh AD. Surgical site infection following cesarean section in Ethiopia. BMC Res Notes. 2019; 12: 288. |
| [3] | Smith AK. Cesarean Section Surgical Site Infection Prevention. 2017. |
[2, 3]
.
SSIs after cesarean delivery can be classified into superficial, deep, and organ/space infections, depending on the extent of tissue involvement
| [2] | Azeze GG, Bizuneh AD. Surgical site infection following cesarean section in Ethiopia. BMC Res Notes. 2019; 12: 288. |
[2]
. Despite notable advancements in perioperative care, including improved hygiene, sterile surgical techniques, and the routine use of prophylactic antibiotics, SSIs remain a major cause of maternal morbidity and mortality
| [14] | Gibbs RS. Clinical risk factors for puerperal infection. Obstet Gynecol. 1980; 55(5 Suppl): 178S-84S. |
| [15] | Krieger Y, Walfisch A, Sheiner E. Surgical site infection following cesarean deliveries: trends and risk factors. J Matern Fetal Neonatal Med. 2017; 30(1): 8-12. |
| [16] | Salim R, Braverman M, Teitler N, Berkovic I, Suliman A, Shalev E. Risk factors for infection following cesarean delivery: an interventional study. J Matern Fetal Neonatal Med. 2012; 25(12): 2708-12. |
[14-16]
. Globally, SSI incidence following cesarean section ranges from 3% to 15%, with variation influenced by population characteristics, healthcare quality, and surgical practices
| [12] | Olsen MA, Butler AM, Willers DM, Devkota P, Gross GA, Fraser VJ. Risk factors for surgical site infection after low transverse cesarean section. Infect Control Hosp Epidemiol. 2008; 29(6): 477-84. |
| [13] | Opøien HK, Valbø A, Grinde-Andersen A, Walberg M. Post-cesarean surgical site infections: rates and risk factors. Acta Obstet Gynecol Scand. 2007; 86(9): 1097-102. |
| [17] | Awad SS. Adherence to surgical care improvement project measures and post-operative surgical site infections. Surg Infect (Larchmt). 2012; 13(4): 234-7. |
[12, 13, 17]
.
The increasing rate of cesarean deliveries worldwide-estimated at 22.9 million in 2012 alone-is alarming, particularly in light of WHO recommendations suggesting that only 10-15% of all births require CS
| [6] | Horan TC, Gaynes RP, Martone WJ, Jarvis WR, Emori TG. CDC definitions of nosocomial surgical site infections. Infect Control Hosp Epidemiol. 1992; 13(10): 606-8. |
| [11] | Molina G, Weiser TG, Lipsitz SR, et al. Cesarean delivery rate and maternal and neonatal mortality. JAMA. 2015; 314(21): 2263-70. |
[6, 11]
. Yet many countries now report CS rates far exceeding this threshold. For instance, in Australia and New Zealand, CS accounts for approximately 30% of hospital deliveries
| [7] | Ehrenkranz NJ, Richter EI, Phillips PM, Shultz JM. Surgical site infections: false-positive diagnoses. Infect Control Hosp Epidemiol. 1995; 16(12): 712-6. |
| [8] | Taylor G, McKenzie M, Kirkland T, Wiens R, Rose M. Surgeon's diagnosis on surgical wound infection rates. Am J Infect Control. 1990; 18(5): 295-9. |
| [9] | Centers for Disease Control and Prevention. Consensus paper on surveillance of surgical wound infections. Infect Control Hosp Epidemiol. 1992; 13(10): 599-605. |
[7-9]
. This surge is attributed not only to clinical indications but also to elective and repeat procedures, socioeconomic factors, and rising maternal comorbidities such as obesity and diabetes, both of which are strongly associated with postoperative complications including SSIs
| [12] | Olsen MA, Butler AM, Willers DM, Devkota P, Gross GA, Fraser VJ. Risk factors for surgical site infection after low transverse cesarean section. Infect Control Hosp Epidemiol. 2008; 29(6): 477-84. |
| [13] | Opøien HK, Valbø A, Grinde-Andersen A, Walberg M. Post-cesarean surgical site infections: rates and risk factors. Acta Obstet Gynecol Scand. 2007; 86(9): 1097-102. |
| [18] | Novelia S. Surgical Site Infection Post-Cesarean: Integrative Review. 2020. |
| [21] | Novelia S, Kurniati N, Yona S. Surgical site infection post-cesarean: an integrative review. Nurse Media J Nurs. 2017; 7(1): 46-55. |
[12, 13, 18, 21]
.
Studies from both developed and developing nations reveal a wide variation in CS-SSI prevalence: 12.5% in Nigeria, 29.4% in Oman, 9.6% in Thailand, and up to 51% among obese women in England
| [18] | Novelia S. Surgical Site Infection Post-Cesarean: Integrative Review. 2020. |
| [19] | Johnson A, Young D, Reilly J. Caesarean section surgical site infection surveillance. J Hosp Infect. 2006; 64(1): 30-5. |
[18, 19]
. In the United States, SSI rates among obese women reach 13.5%, while Australia reports a 10% rate among the general population
| [19] | Johnson A, Young D, Reilly J. Caesarean section surgical site infection surveillance. J Hosp Infect. 2006; 64(1): 30-5. |
[19]
. These infections not only prolong hospitalization and increase healthcare costs but also exert emotional, physical, and socioeconomic burdens on mothers, particularly during the postpartum period when they are expected to care for their newborns
| [16] | Salim R, Braverman M, Teitler N, Berkovic I, Suliman A, Shalev E. Risk factors for infection following cesarean delivery: an interventional study. J Matern Fetal Neonatal Med. 2012; 25(12): 2708-12. |
| [17] | Awad SS. Adherence to surgical care improvement project measures and post-operative surgical site infections. Surg Infect (Larchmt). 2012; 13(4): 234-7. |
| [20] | Watts DH, Krohn MA, Hillier SL, Eschenbach DA. The association of occult amniotic fluid infection with preterm labor. Obstet Gynecol. 1992; 79(3): 351-7. |
| [22] | Stapleton EJ, Hohmann S, Francis HL, Etzioni DA. Disposable jackets and surgical site infections. JAMA Surg. 2020; 155(1): 15-20. |
[16, 17, 20, 22]
.
Risk factors for CS-SSI are broadly categorized into intrinsic and extrinsic types. Intrinsic factors include obesity, diabetes, limited mobility, poor nutritional status, preeclampsia, and premature rupture of membranes, while extrinsic factors involve surgical practices such as prolonged operative time, inadequate skin preparation, lack of antibiotic prophylaxis, use of drains, and emergency or unscheduled procedures
| [21] | Novelia S, Kurniati N, Yona S. Surgical site infection post-cesarean: an integrative review. Nurse Media J Nurs. 2017; 7(1): 46-55. |
[21]
. These factors contribute significantly to postoperative complications and maternal outcomes.
Despite global improvements in infection control and perioperative care, the burden of post-cesarean SSIs remains high and is projected to rise alongside the increasing CS rates. Therefore, understanding the epidemiology and risk factors of CS-SSI is critical for designing effective prevention strategies. Evidence-based interventions-such as optimization of maternal health, timely antibiotic prophylaxis, and adherence to surgical best practices-are essential to mitigate the impact of SSIs and improve maternal outcomes
| [10] | Miller ES, Hahn K, Grobman WA. Consequences of primary elective cesarean delivery. Obstet Gynecol. 2013; 121(4): 789-97. |
| [21] | Novelia S, Kurniati N, Yona S. Surgical site infection post-cesarean: an integrative review. Nurse Media J Nurs. 2017; 7(1): 46-55. |
| [23] | Gelaw KA, Dejene TA, Mamo YT. Surgical site infection following cesarean section in Ethiopia: a prospective cohort study. Patient Saf Surg. 2017; 11: 18. |
| [24] | Larsen JW, Gavard JA. Guidelines for prevention of post-operative infection in obstetrics and gynecology. Infect Dis Obstet Gynecol. 2003; 11: 65-70. |
| [25] | Jido TA, Garba ID. Surgical site infection following cesarean section in Kano, Nigeria. Ann Med Health Sci Res. 2012; 2(1): 33-6. |
[10, 21, 23-25]
.
2. Methods
2.1. Study Setting and Study Period
This study was conducted in Addis Ababa, the capital city of Ethiopia, centrally located within the country. The city spans an area of approximately 210 square kilometers and, according to the 2007 national census, has a population of 3,384,569
| [29] | Dacho A, Angelo A. Surgical site infection following cesarean section in Mizan Tepi University Teaching Hospital, Southwest Ethiopia. J Nurs Care. 2018; 7: 454. |
[29]
. Administratively, Addis Ababa is divided into 11 sub-cities, situated at an average altitude of 2,300 meters (7,546 feet) above sea level. Each sub-city comprises 10 to 12 woredas, and the city includes a total of 328 kebeles
| [26] | Shiferaw WS, Aynalem YA, Akalu TY, Petrucka PM, Anbesu EW. Surgical site infections in Ethiopia: a systematic review and meta-analysis. BMC Surg. 2020; 20: 107. |
[26]
.
The research was carried out in selected public hospitals within Addis Ababa, which serve as either tertiary or general hospitals for their respective catchment populations. In total, the city has 11 public hospitals and approximately 98 public health centers that offer a broad range of healthcare services, including maternal and child health care.
Data collection took place between June 10 and August 30, 2024. This study relied on retrospective data extracted from delivery registers, specifically focusing on cases of post-cesarean section surgical site infections documented from January 1, 2019, through December 31, 2023.
2.2. Study Design
An institution-based cross-sectional study design was employed to assess the magnitude and associated factors of post-cesarean section surgical site infections in selected hospitals of Addis Ababa.
2.3. Source Population
The source population consisted of all medical records related to delivery services at the selected hospitals in Addis Ababa, Ethiopia.
2.4. Study Population
The study population included the selected medical documents of mothers who delivered via cesarean section at the chosen hospitals during the study period.
2.5. Sample Size Determination and Sampling Procedure
The sample size was calculated using the single population proportion formula based on a previous study reporting a 12.9% prevalence of post-cesarean section surgical site infections
| [27] | Mohammed AS, Kassaw AA. Magnitude of surgical site infection following cesarean section in Mizan Tepi University Teaching Hospital, Southwest Ethiopia. J Nurs Care. 2018; 7: 454. |
[27]
. The following parameters were used for the calculation:
Level of significance (α) = 0.05
Margin of error (d) = 5%
Confidence level = 95% (Zα/2 = 1.96)
Prevalence (P) = 0.129
The initial sample size (n) was calculated as
So calculated is n= 172
Additionally, Epi Info Version 7.2.1.0 was used to calculate sample sizes for factors associated with post-cesarean section infections, applying the double population proportion formula with assumptions of 80% power, 95% confidence level, and a 1:1 ratio of exposed to unexposed groups.
Table 1. Summarizes the sample size calculations for key factors influencing post-cesarean section infection in the selected hospitals of Addis Ababa, 2024.
S. no | Proportion/factor | AOR | Calculated sample size | References |
1 | Had Prophylaxis given | % of exposed 12.1% | 0.385 | 85 | | [28] | Abseno M. Prevalence and determinants of tuberculosis among Addis Ababa city bus drivers. 2004. |
[28] |
% of unexposed 87.9% |
2 | Post-operative hospital stay | % exposed=7.1 | 0.109 | 109 | | [28] | Abseno M. Prevalence and determinants of tuberculosis among Addis Ababa city bus drivers. 2004. |
[28] |
% unexposed=92.9 |
Since the calculated sample sizes for individual factors were relatively small, the largest sample size was selected and adjusted by applying a design effect of 2.5 and accounting for a 10% non-response rate. Consequently, the final sample size for the study was set at 473 participants.
2.6. Sampling Technique
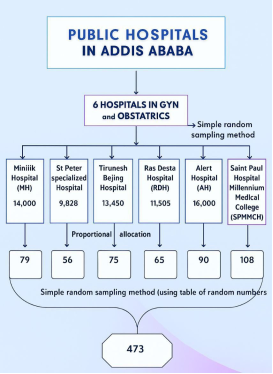
Initially, hospitals within Addis Ababa were selected through a random sampling process. Subsequently, six hospitals-St. Paul’s Specialized Hospital (SPSH), Alert Hospital (AH), St. Paul’s Millennium Medical College (SPMMC), Menelik Hospital (MH), Trunesh Beijing Hospital (TBH), and Ras Desta Hospital (RDH)-were chosen using the lottery method to ensure unbiased representation.
St. Peter Hospital (SPH) and Alert Hospital (AH) each serve a catchment area encompassing 36 health centers, collectively covering 72 health centers in total. The remaining 26 health centers fall under the catchment areas of St. Paul’s Millennium Medical College Hospital (SPMMCH), Menelik Hospital, Trunesh Beijing Hospital, and Ras Desta Hospital. This structured sampling approach ensures a broad and representative inclusion of healthcare facilities across Addis Ababa’s diverse health system
Figure 1. Schematic presentation of sampling procedure to post cesarean section infection and Associated Factor in selected Hospitals, Addis Ababa, 2024.
2.7. Eligibility Criteria
2.7.1. Inclusion Criteria
All medical records of mothers diagnosed with post-cesarean section surgical site infections (SSI) at the selected hospitals in Addis Ababa, spanning from January 1, 2019, to December 31, 2024, were included in this study.
2.7.2. Exclusion Criteria
Medical records that were incomplete, illegible, damaged, or otherwise unreadable were excluded from the study.
2.8. Data Collection Procedure
Data were collected using a structured, questionnaire developed by the researcher in English. The tool was pre-tested to ensure clarity and consistency. Data collection was performed by trained midwives holding a Bachelor of Science degree. These data collectors received orientation and training on the study objectives, interviewing techniques, ethical considerations, and data quality assurance.
The entire process was closely monitored by the principal investigator and designated supervisors. Data collectors conducted a thorough chart review, with ongoing support provided by the principal investigator in case of challenges during data collection.
2.8.1. Data quality Assurance
A pre-test was conducted using 5% of the total sample (30 post-cesarean records) before the actual data collection began. The pre-test helped evaluate the effectiveness and accuracy of the questionnaire in capturing the required data. Based on the results, necessary modifications were made to improve the tool’s reliability and clarity.
To ensure high-quality data, a one-day training session was provided to data collectors and supervisors by the principal investigator. The training covered the study objectives, data collection methods, confidentiality, and standard operating procedures. Each completed questionnaire was reviewed daily by supervisors for accuracy and completeness, and the principal investigator performed a double-check to ensure consistency.
2.9. Data Analysis and Interpretation
Data were entered into Epi-Data version 3.1, cleaned, and then exported to SPSS version 26 for statistical analysis. Variables were recoded as necessary prior to analysis. Descriptive statistics, including frequencies, means, medians, standard deviations, and percentages, were used to summarize socio-demographic characteristics and post-cesarean section infection data. Results were presented using tables and figures for clarity.
To assess associations, chi-square tests were used for categorical variables. Bivariate analysis was first conducted using binary logistic regression to examine the relationship between each independent variable and the outcome. Variables with a p-value < 0.25 were included in the multivariate logistic regression model, as per Hosmer and Lemeshow’s guideline, to control for potential confounders.
Multivariate logistic regression was then performed to identify factors independently associated with post-cesarean section infections. Variables with a p-value < 0.05 and 95% confidence intervals were considered statistically significant. Both crude and adjusted odds ratios (COR and AOR) with 95% CI were reported to determine the strength and direction of the associations
2.10. Study Variables
2.10.1. Dependent Variable
Maternal surgical site infection (SSI) following cesarean section
2.10.2. Independent Variables
Socio-demographic Characteristics
1) Age (in years)
2) Marital status
3) Educational level of the mother
4) Occupational status
Monthly income
Housing condition
Anthropometric Measurements
Weight
Height
Body Mass Index (BMI)
Obstetric and Clinical Factors
Gravidity
Duration of labor
Time of rupture of membrane
Operational definition
surgical site infection (SSI). Surgical site infections are classified based on the United States Centers for Disease Control and Prevention (CDC) definitions into superficial and deep incisional SSIs:
Superficial Incisional SSI: An infection occurring within 30 days after surgery that involves only the skin or subcutaneous tissue of the incision, with at least one of the following criteria:
Purulent drainage from the superficial incision, with or without laboratory confirmation.
Organisms isolated from an aseptically obtained culture of fluid or tissue from the superficial incision.
Signs or symptoms such as pain or tenderness, localized swelling, redness, or heat, and the incision is deliberately opened by a surgeon unless the culture is negative.
Diagnosis of superficial SSI by the surgeon or attending physician.
Deep Incisional SSI; An infection occurring within 30 days post-operation involving the deep soft tissues (e.g., fascial or muscle layers), with at least one of the following:
Purulent drainage from the deep incision (excluding organ/space infections).
Spontaneous dehiscence or deliberate opening of the deep incision by a surgeon when the patient presents with fever (>38°C), localized pain, or tenderness, unless the site is culture-negative.
Presence of abscess or other signs of infection found during direct examination, reoperation, histopathological, or radiologic evaluation.
Diagnosis of deep SSI by a surgeon or attending physician. From US Centers for Disease Control and Prevention Superficial incisional SSI Infection occurs within 30 days after the operation and infection involves only skin or subcutaneous tissue of the incision and at least one of the following:
Other Relevant Definitions
Cellulitis: Characterized by a painful and tender wound, with erythema and edema extending beyond the edge of the incision.
Wound Abscess: Defined as an unusually tender wound accompanied by serous or bloody discharge.
Wound Dehiscence: Refers to the partial or complete separation of the surgical wound, where fascia and/or skin layers burst open.
Pelvic Abscess: Identified by persistent spiking fever or chills, lower abdominal pain and distension, adnexal tenderness, and poor response to antibiotics; swelling may be found in the adnexa or pouch of Douglas.
Peritonitis: Clinical signs include low-grade fever or chills, lower abdominal pain, absent bowel sounds, rebound tenderness, abdominal distension, nausea or vomiting, anorexia, and in severe cases, signs of shock.
Urinary Tract Infection (UTI): Diagnosed when the patient presents with flank pain, dysuria (burning sensation during urination), and fever.
Lost to Follow-Up: Mothers who were discharged but did not return for post-discharge follow-up and could not be reached for outcome assessment.
3. Results
3.1. Socio-Demographic and Medical Characteristics
A total of 473 mothers who underwent cesarean section for delivery during the study period in selected hospitals of Addis Ababa, Ethiopia, in 2024 were initially included. However, 1 case were excluded due to maternal death within the first two days post-operation. As a result, data from 472 mothers were analyzed.
The age of participants ranged from 15 to 45 years, with a mean age of 28 years (±5 SD). The largest proportion, 46.7% (n = 221), were between 20 and 29 years of age. Additionally, 30% (n = 141) were between 30 and 39 years, 17% (n = 61) were aged 15 to 19, and the remaining 10.3% (n = 49) were between 40 and 45 years.
Regarding religion, 35% (n = 165) of the mothers identified as Orthodox Christian, 34% (n = 160) as Muslim, and 17% (n = 61) as Protestant or Catholic. The remaining 7% (n = 33) adhered to other religious beliefs.
In terms of occupation, 48.9% (n = 231) of the participants were employed, while 31% (n = 146) were housewives. Educationally, 28% (n = 132) had no formal education. About 30% (n = 142) reported low monthly family income, indicating socioeconomic vulnerability. A significant majority of the mothers (78%) resided in urban areas. (Refer to
Table 2 for detailed distribution.)
Table 2. Socio-demographic characteristics of women who are under the procedure of C/S in in selected hospitals of Addis Ababa, Ethiopia 2024. (n=472).
Variables | Variables categories | Frequency | Percentage (%) |
Age of mother | 15-19 | 61 | 13 |
20-29 | 221 | 46.7 |
30-39 | 141 | 30 |
40-45 | 49 | 10.3 |
Educational status of mothers | Uneducated | 132 | 28 |
Read and write | 108 | 23 |
Primary school | 198 | 42 |
Secondary school and above | 33 | 7 |
Marital status | Single | 67 | 14 |
Married | 325 | 69 |
Divorced | 52 | 11 |
Widowed | 28 | 6 |
religion | Muslim | 160 | 34 |
Orthodox | 165 | 35 |
catholic | 52 | 11 |
Protestant | 61 | 13 |
Other | 33 | 7% |
income | Lower | 142 | 30 |
Middle | 283 | 60 |
higher | 47 | 10 |
occupation | House wife | 146 | 31 |
Government employee | 66 | 14 |
Private employee | 80 | 17 |
Merchant | 43 | 9 |
Daily laborer | 57 | 12 |
Student | 80 | 17 |
Residency | Urban | 368 | 78% |
Rural | 104 | 22% |
3.2. Obstetric, Medical, and Operative Characteristics of Women Undergoing Cesarean Section
Based on the analyzed data, the majority of women who underwent cesarean section were primiparous, accounting for 45% (n = 212), followed by multiparous women at 34% (n = 160). Grand multiparas constituted 17% (n = 61), while nulliparous women represented 8% (n = 38). Regarding gestational age, 79% (n = 373) of the deliveries occurred between 37 and 42 weeks of gestation. Preterm births (less than 37 weeks) accounted for 14% (n = 66), and post-term pregnancies (over 42 weeks) comprised 7% (n = 33). A substantial proportion-80% (n = 378)-of women experienced labor prior to surgery, with 85% (n = 401) reporting a labor duration of less than 24 hours.
In terms of membrane status, 93% (n = 439) had intact membranes at the time of operation. Concerning amniotic fluid, 85% (n = 401) had clear fluid, whereas 12% (n = 71) had meconium-stained fluid, and 3% (n = 14) had blood-stained fluid. Finally, the majority of cesarean sections-86% (n = 406)-were performed under emergency conditions, reflecting the critical clinical circumstances surrounding most of the procedures (
Table 3).
Table 3. Presents the obstetric, medical, and operative characteristics of women who underwent cesarean section in selected hospitals across Addis Ababa, Ethiopia, in 2024 (n = 472).
Variables | Variables categories | Frequency (N=472) | Percentage (%) |
Parity | Nulliparous | 38 | 8 |
primipara | 212 | 45 |
multipara | 160 | 34 |
grand multipara | 61 | 13 |
Gestational Age | <37weeks | 66 | 14 |
37-42 weeks | 373 | 79 |
>42 weeks | 33 | 7 |
Co morbid disease | Yes | 334 | 70.8 |
No | 118 | 29.2 |
Mothers have been in labor before operation | Yes | 378 | 80 |
No | 94 | 20 |
Duration of Labor | >24 | 71 | 15 |
<24 | 401 | 85 |
Membrane state | intact | 439 | 93 |
Ruptured | 33 | 7 |
Duration of membrane Ruptured | <24 | 377 | 80% |
>24 | 94 | 20% |
Colour of liquor | clear | 401 | 85% |
Meconium | 71 | 12% |
blood stained | 14 | 3 |
Type of Cs | Emergency | 406 | 86 |
Elective | 66 | 14 |
Indication of Cs | Obstructed labor | 80 | 17 |
Fetal Distress/NRF HB | 236 | 50 |
Previous CS | 42 | 9 |
Mal-presentation | 51 | 11 |
Uterine rupture | 61 | 13 |
3.3. Intraoperative and Postoperative Pregnancy and Labor-Related Characteristics
According to the data, the majority of cesarean operations-55% (n = 259)-were completed within 15 to 30 minutes. An additional 30% (n = 142) took less than 15 minutes, while 9% (n = 42) lasted between 30 and 45 minutes, and 6% (n = 28) exceeded 45 minutes, lasting up to 60 minutes. Regional anesthesia was the predominant method used, administered in 96% (n = 453) of the cases. Prophylactic antibiotics were given to 92% (n = 434) of the mothers as part of infection prevention protocols. Regarding estimated blood loss, 55% (n = 260) of the participants lost less than 500 ml, 27% (n = 127) lost between 500 and 1000 ml, 18% (n = 85) experienced blood loss between 1001 and 1500 ml, and 12% (n = 57) lost more than 1500 ml during surgery. Prior to the operation, 75% (n = 354) had a hematocrit level above 10%, yet 35% (n = 165) of the women required blood transfusions. Postoperatively, 83% (n = 392) showed no signs of infection, indicating successful management and prevention of surgical site infections (SSIs). In addition, 76% (n = 359) had received antenatal care (ANC) during pregnancy.
A longitudinal abdominal incision was the most commonly performed technique, used in 92% of cases. At the time of wound assessment, 65% (n = 307) were documented as having clean wounds, free of any surgical site infection. (
Table 4).
Table 4. Intraoperative and Postoperative Pregnancy and Labor-Related Characteristics of Women Undergoing Cesarean Section in Selected Hospitals of Addis Ababa, Ethiopia, 2024 (n = 472).
Variables | Variables categories | Frequency (N=472) | Percentage (%) |
Duration of the operation | <15 min | 142 | 30 |
15-30 min | 259 | 55 |
30-45min | 42 | 9 |
45-60 min | 29 | 6 |
Type of Anesthesia | Regional | 453 | 96 |
general | 19 | 4 |
Had prophylaxis given | Yes | 434 | 92 |
No | 38 | 8 |
Pre-op hematocrit count | >10% | 354 | 75 |
<10% | 118 | 25 |
Was the client transfused | Yes | 165 | 35 |
No | 307 | 65 |
Sign of infection | Yes | 80 | 17 |
no | 392 | 83 |
ANC follow up | Yes | 359 | 76 |
No | 113 | 24 |
Previous History of CS | Yes | 61 | 13 |
No | 411 | 87 |
Types of Abdominal incision | Longitudinal | 434 | 92 |
vertical | 38 | 8 |
Post op Hematocrit | <10 | 354 | 75% |
>10 | 118 | 25% |
Surgical site infection | Clean | 307 | 65 |
clean contaminated | 113 | 24 |
contaminated | 52 | 11 |
3.4. Post Cesarean Section Infection
The pie chart below illustrates the prevalence of post-caesarean section infections among women who underwent cesarean delivery in selected hospitals in Addis Ababa during 2024. The data reveal that 17% of patients developed infections following surgery, represented by the vibrant red/orange segment. In contrast, the majority-83%-experienced no infection
Figure 2. Shows prevalence of post cesarean section infection in selected hospitals in Addis Ababa Ethiopia 2024.
3.5. Bivariable Analysis of Factors Affecting CS
In the multivariable logistic regression analysis, several factors showed a statistically significant association with post-caesarean section infections (p < 0.005). The presence of clinical signs of infection was a strong predictor: women exhibiting these signs were 4.37 times more likely to develop post-operative infections compared to those without such signs [Adjusted Odds Ratio (AOR) = 4.37; 95% CI: 3.25-6.22]. Similarly, women with co-morbid medical conditions were found to be 4.72 times more likely to experience post-cesarean section infections than those without underlying health issues [AOR = 4.72; 95% CI: 3.34-6.23]. A prior history of cesarean section also significantly increased the risk, with affected women being 3.41 times more likely to develop infections compared to those undergoing their first CS [AOR = 3.41; 95% CI: 2.24-4.32]. Furthermore, the duration of labor was a significant factor: women who labored for more than 24 hours were 2.43 times more likely to develop post-operative infections [AOR = 2.43; 95% CI: 1.83-3.62]. Lastly, operation duration played a role-procedures lasting between 30 and 45 minutes were associated with a 3.43-fold increase in infection risk compared to shorter surgeries [AOR = 3.43; 95% CI: 1.32-4.43 (
Table 5).
Table 5. Shows a bivariate- analysis of factors affecting post cesarean section infection relation of women who are under the procedure of C/S in selected hospitals of Addis Ababa, Ethiopia 2024. (n=472)
Variables | Ceserian section | COR (95%) | AOR(5% CI) | P-value |
Post Cs infection | No infection |
Sign of infection | | | | | 0.000 |
Yes | 80 | 17 | 6.46(5.22-8.35) ⃰⃰⃰⃰ | 4.37(3.25-6.22) ⃰⃰⃰⃰ ⃰⃰⃰⃰ |
No | 199 | 176 | 1 | 1 |
Co- morbid disease | | | | | 0.000 |
YES | 80 | 38 | 5.53(3.52-7.23) | 4.72(3.34-6.23) ⃰⃰⃰⃰ ⃰⃰⃰⃰ |
No | 66 | 268 | 1 | 1 |
History of CS | | | | | 0.000 |
Yes | 48 | 13 | 4.53(2.64-5.63) ⃰⃰⃰⃰ | 3.41(2.24-4.32) ⃰⃰ ⃰⃰ |
No | 73 | 338 | 1 | 1 |
Duration of Labor: | | | | | 0.000 |
> 24 | 56 | 15 | 3.42(2.32-4.53) ⃰ | 2.43(1.83-3.62) ⃰⃰ ⃰⃰ |
<24 | 165 | 236 | 1 | 1 |
Duration of the operation: | | | | | |
<15 min | 62 | 80 | 1.34(0.86-2.32) | 1.21(0.54-2.23) | 0.000 |
15-30 min | 70 | 189 | 2.22(0.24-3.11) | 1.23(0.13-2.34) | 0.000 |
30-45min | 36 | 6 | 4.23(1.45-5.23) ⃰ | 3.43(1.32-4.43)⃰ ⃰⃰ | 0.000 |
45-60 min | 19 | 9 | 1 | 1 | |
4. Discussion
Pregnant women remain particularly vulnerable to infections during labor and delivery, with surgical site infections (SSIs) being the most common hospital-acquired infections in obstetric care-accounting for approximately 38% of nosocomial infections in this patient group
| [20] | Watts DH, Krohn MA, Hillier SL, Eschenbach DA. The association of occult amniotic fluid infection with preterm labor. Obstet Gynecol. 1992; 79(3): 351-7. |
[20]
. The findings of this study are consistent with global and regional evidence, highlighting key risk factors that significantly contribute to the development of post-caesarean section infections.
Notably, women who experienced prolonged labor exceeding 24 hours were found to be 2.43 times more likely to develop post-operative infections compared to those with shorter labor durations [AOR = 2.43; 95% CI: 1.83-3.62]. This may be attributed to the increased risk of ascending infections, prolonged rupture of membranes, and heightened maternal exhaustion-factors that compromise immune function and tissue integrity.
In addition, longer operative times were strongly associated with increased infection risk. Specifically, surgical procedures lasting between 30 to 45 minutes were linked to a 3.43-fold higher likelihood of post-cesarean infection [AOR = 3.43; 95% CI: 1.32-4.43]. This supports findings from a recent Ethiopian systematic review and meta-analysis, which reported that cesarean surgeries exceeding one hour were significantly associated with higher infection rates, with an AOR of 1.78 (95% CI: 1.08-2.94)
| [27] | Mohammed AS, Kassaw AA. Magnitude of surgical site infection following cesarean section in Mizan Tepi University Teaching Hospital, Southwest Ethiopia. J Nurs Care. 2018; 7: 454. |
[27]
. Prolonged surgeries may expose tissues to pathogens for longer periods, increase blood loss, and reflect complex or emergency procedures-all of which contribute to a higher infection burden.
Furthermore, global literature and WHO data continue to emphasize the need for evidence-based protocols to reduce SSI risk, including timely antibiotic prophylaxis, improved labor monitoring, and strict surgical asepsis-especially in high-volume settings like those in Addis Ababa. The growing rate of cesarean sections in urban Ethiopia underscores the importance of identifying modifiable risk factors to improve maternal outcomes and reduce healthcare costs associated with postoperative infections.
5. Conclusion and Recommendation
This study revealed that the prevalence of post-cesarean section surgical site infections (SSIs) in selected hospitals in Addis Ababa was 17%, which is considerably higher than internationally accepted benchmarks. These findings underscore an urgent need to strengthen maternal healthcare systems, particularly regarding surgical safety, infection prevention, and quality obstetric services.
Several key factors were significantly associated with post-cesarean infections. These included the presence of co-morbidities, a history of previous cesarean sections, clinical signs of infection, prolonged labor exceeding 24 hours, and extended surgical duration ranging from 30 to 45 minutes. Each of these risk factors reflects opportunities for targeted intervention to reduce maternal morbidity and improve clinical outcomes.
Recommendations
Based on the findings of this study, the following recommendations are proposed:
Strengthen Infection Prevention and Surgical Standards:
Hospital staff should adhere strictly to standard infection prevention protocols and evidence-based surgical techniques. Special emphasis should be placed on proper aseptic procedures, timely antibiotic prophylaxis, and minimizing operative time through skilled surgical practice.
Enhance Antenatal Care Services
Antenatal care (ANC) should be leveraged as a platform for infection prevention by promoting the use of iron-folate supplementation, screening and managing maternal co-morbidities, and educating women on danger signs and hygiene practices during pregnancy and labor.
Ensure Skilled Attendance and Emergency Preparedness: The presence of qualified, senior-level obstetricians during cesarean procedures is essential, especially in high-risk cases. Facilities should be equipped with maternal waiting rooms in appropriate settings to improve access to timely referrals and reduce delays in care.
Promote Awareness and Health Education: Community-level education and awareness campaigns should focus on the early identification of labor complications, infection symptoms, and the importance of institutional delivery. Mothers should be counseled on when to seek care and the benefits of adhering to ANC follow-up.
Optimize Labor Monitoring and Timely Decision-Making: Continuous monitoring of labor using partographs and strict adherence to labor management protocols should be prioritized to prevent prolonged labor, which is a known risk factor for infection. Timely decision-making regarding cesarean section is crucial.
Policy and Resource Allocation: Government and health authorities should prioritize investments in expanding basic and comprehensive emergency obstetric care (BEmONC and CEmONC) services at the community and district levels, ensuring all women have access to safe, high-quality surgical care when needed.
This integrated approach is vital for reducing the burden of post-cesarean infections and achieving better maternal health outcomes in Addis Ababa and similar urban settings
Abbreviations
BEmONC | Basic and Comprehensive Emergency Obstetric Care |
CEmONC | Comprehensive Emergency Obstetric Care |
CDC | Center for Disease Control and Prevention |
CI | Confidence Interval |
SSIs | Surgical Site Infections |
UTI | Urinary Tract Infection |
RRR | Relative Risk Ratio |
C/S | Caesarean Section |
OR | Operation room |
PO | per Oath |
SSI | Surgical Site Infections |
WHO | World Health Organization |
CDC | Center for Disease Control and Prevention |
Acknowledgments
The authors would like to thank Addis Ababa health bureau for providing ethical clearance and the study participants for their participation., all Addis ababa Hospitals administrators, for accepting to conduct the study, as well as special thanks to the participants for accepting and obtaining consent to conduct this study.
Author Contributions
Abdurehman Seid Mohammed and Abate Assefa served as the principal investigators and were actively involved in all stages of the research process, including proposal development, study design, conceptualization, questionnaire development, supervision, data collection, data entry, statistical analysis, and interpretation of findings. Rejeb Nesru Kemal and Abdurehman Seid Mohammed jointly supervised the data collection, oversaw the data analysis, and contributed to the final writing and refinement of the study outputs. The manuscript was prepared and finalized for journal submission by Abdurehman Seid Mohammed.
Declarations
Ethics Approval and Consent
Ethical approval for this study was obtained from the Institutional Review Board (IRB) of the Addis Ababa Health Bureau. Formal ethical clearance was granted by the respective ethical review committee. The study adhered strictly to the ethical principles outlined in the Declaration of Helsinki. Prior to data collection, written informed consent was obtained from the legal guardians of all research participants. Throughout the research process, the confidentiality, privacy, and autonomy of participants were fully respected, and all procedures were conducted with the highest ethical standards.
Consent for Publication
Not relevant.
Availability of Data and Materials
The corresponding author can provide the datasets used and analyzed in this study upon reasonable request.
Funding
No financial support for the research authorship and/or publication of this article
Conflicts of Interest
The author(s) declared no potential conflicts of interest concerning the research, authorship, and/or publication of this article.
References
| [1] |
Solomkin J, Kluytmans J, Alnaif B, et al. WHO global guidelines for the prevention of surgical site infection. Lancet Infect Dis. 2017; 17(3): 262-4.
|
| [2] |
Azeze GG, Bizuneh AD. Surgical site infection following cesarean section in Ethiopia. BMC Res Notes. 2019; 12: 288.
|
| [3] |
Smith AK. Cesarean Section Surgical Site Infection Prevention. 2017.
|
| [4] |
World Health Organization. WHO Statement on Caesarean Section Rates. Geneva: WHO; 2015.
|
| [5] |
Mangram AJ, Horan TC, Pearson ML, Silver LC, Jarvis WR. Guideline for prevention of surgical site infection. Infect Control Hosp Epidemiol. 1999; 20: 250-78.
|
| [6] |
Horan TC, Gaynes RP, Martone WJ, Jarvis WR, Emori TG. CDC definitions of nosocomial surgical site infections. Infect Control Hosp Epidemiol. 1992; 13(10): 606-8.
|
| [7] |
Ehrenkranz NJ, Richter EI, Phillips PM, Shultz JM. Surgical site infections: false-positive diagnoses. Infect Control Hosp Epidemiol. 1995; 16(12): 712-6.
|
| [8] |
Taylor G, McKenzie M, Kirkland T, Wiens R, Rose M. Surgeon's diagnosis on surgical wound infection rates. Am J Infect Control. 1990; 18(5): 295-9.
|
| [9] |
Centers for Disease Control and Prevention. Consensus paper on surveillance of surgical wound infections. Infect Control Hosp Epidemiol. 1992; 13(10): 599-605.
|
| [10] |
Miller ES, Hahn K, Grobman WA. Consequences of primary elective cesarean delivery. Obstet Gynecol. 2013; 121(4): 789-97.
|
| [11] |
Molina G, Weiser TG, Lipsitz SR, et al. Cesarean delivery rate and maternal and neonatal mortality. JAMA. 2015; 314(21): 2263-70.
|
| [12] |
Olsen MA, Butler AM, Willers DM, Devkota P, Gross GA, Fraser VJ. Risk factors for surgical site infection after low transverse cesarean section. Infect Control Hosp Epidemiol. 2008; 29(6): 477-84.
|
| [13] |
Opøien HK, Valbø A, Grinde-Andersen A, Walberg M. Post-cesarean surgical site infections: rates and risk factors. Acta Obstet Gynecol Scand. 2007; 86(9): 1097-102.
|
| [14] |
Gibbs RS. Clinical risk factors for puerperal infection. Obstet Gynecol. 1980; 55(5 Suppl): 178S-84S.
|
| [15] |
Krieger Y, Walfisch A, Sheiner E. Surgical site infection following cesarean deliveries: trends and risk factors. J Matern Fetal Neonatal Med. 2017; 30(1): 8-12.
|
| [16] |
Salim R, Braverman M, Teitler N, Berkovic I, Suliman A, Shalev E. Risk factors for infection following cesarean delivery: an interventional study. J Matern Fetal Neonatal Med. 2012; 25(12): 2708-12.
|
| [17] |
Awad SS. Adherence to surgical care improvement project measures and post-operative surgical site infections. Surg Infect (Larchmt). 2012; 13(4): 234-7.
|
| [18] |
Novelia S. Surgical Site Infection Post-Cesarean: Integrative Review. 2020.
|
| [19] |
Johnson A, Young D, Reilly J. Caesarean section surgical site infection surveillance. J Hosp Infect. 2006; 64(1): 30-5.
|
| [20] |
Watts DH, Krohn MA, Hillier SL, Eschenbach DA. The association of occult amniotic fluid infection with preterm labor. Obstet Gynecol. 1992; 79(3): 351-7.
|
| [21] |
Novelia S, Kurniati N, Yona S. Surgical site infection post-cesarean: an integrative review. Nurse Media J Nurs. 2017; 7(1): 46-55.
|
| [22] |
Stapleton EJ, Hohmann S, Francis HL, Etzioni DA. Disposable jackets and surgical site infections. JAMA Surg. 2020; 155(1): 15-20.
|
| [23] |
Gelaw KA, Dejene TA, Mamo YT. Surgical site infection following cesarean section in Ethiopia: a prospective cohort study. Patient Saf Surg. 2017; 11: 18.
|
| [24] |
Larsen JW, Gavard JA. Guidelines for prevention of post-operative infection in obstetrics and gynecology. Infect Dis Obstet Gynecol. 2003; 11: 65-70.
|
| [25] |
Jido TA, Garba ID. Surgical site infection following cesarean section in Kano, Nigeria. Ann Med Health Sci Res. 2012; 2(1): 33-6.
|
| [26] |
Shiferaw WS, Aynalem YA, Akalu TY, Petrucka PM, Anbesu EW. Surgical site infections in Ethiopia: a systematic review and meta-analysis. BMC Surg. 2020; 20: 107.
|
| [27] |
Mohammed AS, Kassaw AA. Magnitude of surgical site infection following cesarean section in Mizan Tepi University Teaching Hospital, Southwest Ethiopia. J Nurs Care. 2018; 7: 454.
|
| [28] |
Abseno M. Prevalence and determinants of tuberculosis among Addis Ababa city bus drivers. 2004.
|
| [29] |
Dacho A, Angelo A. Surgical site infection following cesarean section in Mizan Tepi University Teaching Hospital, Southwest Ethiopia. J Nurs Care. 2018; 7: 454.
|
Cite This Article
-
APA Style
Mohammed, A. S., Kassaw, A. A., Kemal, R. N. (2025). Magnitude and Determinants of Surgical Site Infections Following Cesarean Section: A Retrospective Multi-Hospital Study in Addis Ababa, Ethiopia, 2024. International Journal of Biomedical Engineering and Clinical Science, 11(2), 28-39. https://doi.org/10.11648/j.ijbecs.20251102.12
 Copy
|
Copy
|
 Download
Download
ACS Style
Mohammed, A. S.; Kassaw, A. A.; Kemal, R. N. Magnitude and Determinants of Surgical Site Infections Following Cesarean Section: A Retrospective Multi-Hospital Study in Addis Ababa, Ethiopia, 2024. Int. J. Biomed. Eng. Clin. Sci. 2025, 11(2), 28-39. doi: 10.11648/j.ijbecs.20251102.12
Copy
|
Download
AMA Style
Mohammed AS, Kassaw AA, Kemal RN. Magnitude and Determinants of Surgical Site Infections Following Cesarean Section: A Retrospective Multi-Hospital Study in Addis Ababa, Ethiopia, 2024. Int J Biomed Eng Clin Sci. 2025;11(2):28-39. doi: 10.11648/j.ijbecs.20251102.12
Copy
|
Download
-
@article{10.11648/j.ijbecs.20251102.12,
author = {Abdurehman Seid Mohammed and Abate Assefa Kassaw and Rejeb Nesru Kemal},
title = {Magnitude and Determinants of Surgical Site Infections Following Cesarean Section: A Retrospective Multi-Hospital Study in Addis Ababa, Ethiopia, 2024
},
journal = {International Journal of Biomedical Engineering and Clinical Science},
volume = {11},
number = {2},
pages = {28-39},
doi = {10.11648/j.ijbecs.20251102.12},
url = {https://doi.org/10.11648/j.ijbecs.20251102.12},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ijbecs.20251102.12},
abstract = {Background: Over the past three decades, infections following cesarean sections have increased markedly, with surgical site infections (SSIs) emerging as a leading cause of maternal morbidity and mortality. This issue is especially critical in low- and middle-income countries, including Ethiopia, where reliable data on the magnitude and determinants of post-cesarean infections remain limited. These infections contribute to prolonged hospital stays, higher healthcare costs, and elevated risks for both mothers and newborns. Objective: This study aimed to assess the prevalence of post-cesarean section infections and identify associated risk factors in selected hospitals in Addis Ababa, Ethiopia, in 2024. Methods: An institution-based retrospective cross-sectional study was conducted in selected hospitals between June 10 and August 30, 2024. A total of 472 medical records of women who underwent cesarean sections from January 1, 2019, through December 31, 2023, were reviewed using a systematic random sampling method. Hospitals were selected using simple random sampling. Data were entered and cleaned using Epi Info version 7.2.1.0 and analyzed with SPSS version 26. Binary logistic regression was employed to identify factors associated with post-cesarean infections. Adjusted odds ratios (AORs) with 95% confidence intervals (CIs) were calculated, and statistical significance was determined at a p-value 24 hours), previous cesarean deliveries, and extended operative time. To reduce infection rates, hospitals should enforce strict infection prevention protocols and maintain high standards of surgical practice.},
year = {2025}
}
Copy
|
Download
-
TY - JOUR
T1 - Magnitude and Determinants of Surgical Site Infections Following Cesarean Section: A Retrospective Multi-Hospital Study in Addis Ababa, Ethiopia, 2024
AU - Abdurehman Seid Mohammed
AU - Abate Assefa Kassaw
AU - Rejeb Nesru Kemal
Y1 - 2025/08/18
PY - 2025
N1 - https://doi.org/10.11648/j.ijbecs.20251102.12
DO - 10.11648/j.ijbecs.20251102.12
T2 - International Journal of Biomedical Engineering and Clinical Science
JF - International Journal of Biomedical Engineering and Clinical Science
JO - International Journal of Biomedical Engineering and Clinical Science
SP - 28
EP - 39
PB - Science Publishing Group
SN - 2472-1301
UR - https://doi.org/10.11648/j.ijbecs.20251102.12
AB - Background: Over the past three decades, infections following cesarean sections have increased markedly, with surgical site infections (SSIs) emerging as a leading cause of maternal morbidity and mortality. This issue is especially critical in low- and middle-income countries, including Ethiopia, where reliable data on the magnitude and determinants of post-cesarean infections remain limited. These infections contribute to prolonged hospital stays, higher healthcare costs, and elevated risks for both mothers and newborns. Objective: This study aimed to assess the prevalence of post-cesarean section infections and identify associated risk factors in selected hospitals in Addis Ababa, Ethiopia, in 2024. Methods: An institution-based retrospective cross-sectional study was conducted in selected hospitals between June 10 and August 30, 2024. A total of 472 medical records of women who underwent cesarean sections from January 1, 2019, through December 31, 2023, were reviewed using a systematic random sampling method. Hospitals were selected using simple random sampling. Data were entered and cleaned using Epi Info version 7.2.1.0 and analyzed with SPSS version 26. Binary logistic regression was employed to identify factors associated with post-cesarean infections. Adjusted odds ratios (AORs) with 95% confidence intervals (CIs) were calculated, and statistical significance was determined at a p-value 24 hours), previous cesarean deliveries, and extended operative time. To reduce infection rates, hospitals should enforce strict infection prevention protocols and maintain high standards of surgical practice.
VL - 11
IS - 2
ER -
Copy
|
Download