Objective: Although international guidelines outline best practices for assessing and delivering nutrition to critically ill patients, their implementation varies considerably across Intensive Care Units (ICUs). This study aimed to evaluate current nutritional practices among intensivists, identify challenges in meeting nutritional goals in the ICU, and describe strategies used for post-ICU nutritional care. Methods: An online survey was disseminated to certified intensivists, who were invited to complete a structured questionnaire electronically. Institutional ethics approval (INT/ECI2023/P2/1344) and clinical trial registration (CTRI/2024/01/061457) were obtained. Results: Of 201 respondents, 53% had more than 10 years of clinical experience, and 33% performed in-hospital ICU duties. Most institutions provided patient nutrition 79% reported awareness of established nutritional protocols, yet 69% cited the unavailability of qualified ICU dietitians. Only 6% used indirect calorimetry for caloric assessment. Enteral nutrition was initiated in 95% of patients, predominantly via intermittent bolus feeding (70%), and 80% commenced feeding soon after ICU admission when feasible. Feed intolerance was assessed in 87% of cases using gastric residual volumes, with a threshold of greater than 50% of the previous feed being the common criterion. Nearly 60% initiated parenteral nutrition within 48–72 hours of developing enteral feed intolerance. Protein or albumin levels were used by 69% to assess nutritional status. Only 7% reported structured post-ICU nutritional follow-up. Conclusions: Substantial variability exists in ICU nutritional practices, with limited adherence to international recommendations and significant resource-related barriers.
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited.
Critical Illness, Intensive Care Units, Nutritional Support, Enteral Nutrition, Parenteral Nutrition, Surveys and Questionnaires
1. Introduction
Nutritional support in the intensive care unit (ICU) is a foundational component of the physiological response to critical illness, influencing both short-term and long-term outcomes. Adequate delivery of calories, protein, and micronutrients is essential for preserving organ function, maintaining immune competence, and supporting recovery from metabolic stress.
[1]
Lambell KJ, Tatucu-Babet OA, Chapple LA, Gantner D, Ridley EJ. Nutrition therapy in critical illness: a review of the literature for clinicians. Crit Care. 2020; 24(1): 35.
Despite its importance, nutrition therapy often receives lower priority compared to hemodynamic stabilization, antimicrobial management, and ventilatory care. This imbalance contributes to considerable variation in nutritional strategies across ICUs and may adversely influence patient trajectories.
In many settings, constraints such as limited availability of trained clinical dietitians, insufficient awareness of evidence-based nutritional guidelines, and inconsistent application of existing protocols further complicate efforts to ensure optimal nutritional support.
[2]
Moisey LL, Merriweather JL, Drover JW. The role of nutrition rehabilitation in the recovery of survivors of critical illness: underrecognized and underappreciated. Crit Care. 2022; 26: 270.
Elmezoughi E, de Vasconcellos K. An evaluation of feeding practices and determination of barriers to providing nutritional support in a multidisciplinary South African intensive care unit. South Afr J Crit Care. 2020; 36(1).
Even where local policies exist, their implementation may be hindered by workforce shortages, inadequate training, or competing clinical demands. As critically ill patients are particularly vulnerable to catabolism and malnutrition, lapses in nutritional delivery may prolong ICU stay, impair functional recovery, and burden healthcare systems.
Although the literature is extensive on the consequences of inadequate nutrition in critical illness, fewer studies have examined how intensivists actually apply nutritional principles in daily practice. Understanding clinicians’ real-world approaches is essential for identifying gaps, designing targeted interventions, and strengthening institutional nutritional policies.
This study aimed to evaluate the nutritional practices of intensivists across diverse hospital settings, with an emphasis on the methods used to assess nutritional needs, feeding modalities, identify feeding intolerance, and strategies employed after ICU discharge. The findings provide a clearer understanding of current practice patterns and highlight opportunities for improving the nutritional management of critically ill patients.
2. Methodology and Analysis
A cross-sectional survey was conducted using a structured online questionnaire distributed via email and social media platforms. Intensivists were invited to complete and submit the survey voluntarily and anonymously. The questionnaire consisted of multiple-choice items with optional comment fields, allowing for elaboration where needed. Institutional ethics approval (INT/ECI2023/P2/1344) of Postgraduate Institute of Medical Education and Research, Chandigarh, India, and clinical trial registration (CTRI/2024/01/061457; dated 15 January 2024) were obtained prior to survey dissemination.
Eligible participants were intensivists who had completed formal training in critical care or had more than five years of continuous experience in the ICU and were currently managing critically ill patients.
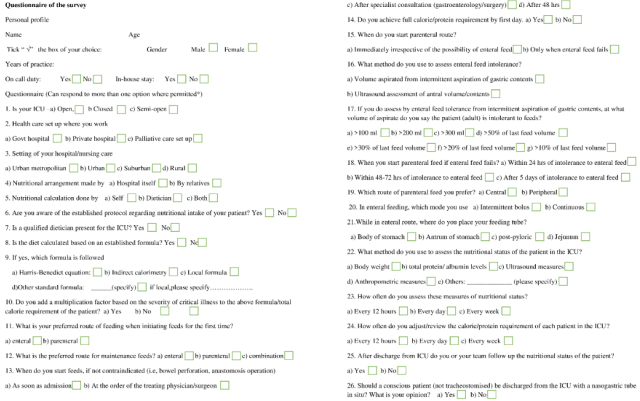
The questionnaire collected information on: (1) Demographic characteristics and workplace settings; (2) Responsibility for calculating nutritional requirements; (3) Timing and route of initiation of nutrition therapy; (4) Assessment methods for feeding intolerance; (5) Indications and timing for parenteral nutrition; (6) Preferred enteral feeding modalities; (7) Approaches to nutritional assessment and post-ICU follow-up. (Figure 1).
Data were summarised descriptively to identify prevailing practice patterns and areas of variability. Numbers have been summarized as counts and percentages for each response. All analyses were performed using R version 4.4.0. In-house intensivists were defined as those who were physically present in the ICUs throughout their shifts.
3. Results
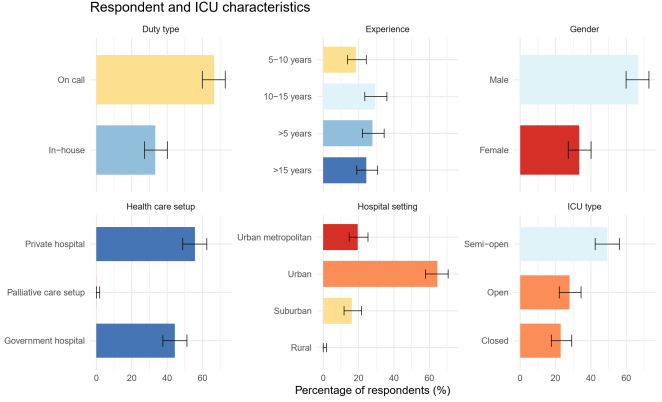
A total of 201 intensivists responded to 367 distributed questionnaires (response rate of 55%). Of these, 134 (66.7%; 95% CI 59.9-72.8%) were male, and more than half reported over 10 years of ICU experience (10–15 years: 59/201 [29.4%; 95% CI 23.5-36.0%]; >15 years: 49/201 [24.4%; 95% CI 19.0-30.8%]). Sixty-seven respondents (33.3%; 95% CI 27.2-40.1%) provided in-house ICU coverage, while the remaining 134 (66.7%; 95% CI 59.9-72.8%) served on call. Semi-open ICUs were the most frequently reported model (99/201 [49.3%; 95% CI 42.4-56.1%]), followed by open (56/201 [27.9%; 95% CI 22.1-34.4%]) and closed ICUs (46/201 [22.9%; 95% CI 17.6-29.2%]). The majority of respondents worked in private hospitals (112/201 [55.7%; 95% CI 48.8-62.4%]) and urban or metropolitan areas (177/211 [83.9%; 95% CI 78.3-88.5%]), with no representation from rural ICUs. (Figure 2).
Distribution of respondent demographics and ICU organizational features. Panels show proportions of intensivists by gender, years of ICU experience, duty pattern (in-house vs on-call), ICU model (open, closed, semi-open), healthcare sector (government vs private), and hospital setting (urban metropolitan, urban, suburban, rural). Values represent the percentage of total respondents (N = 201), error bars represent 95% CI.
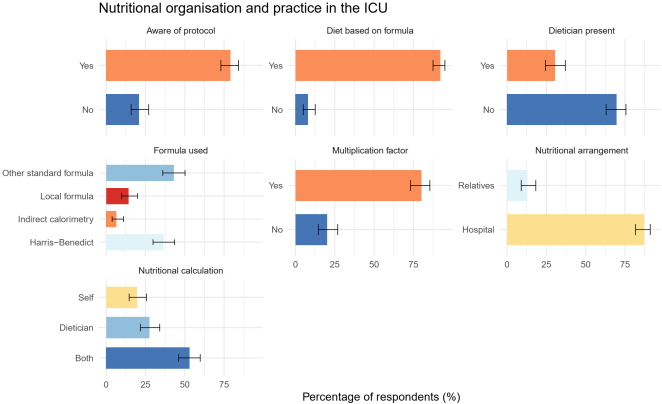
Although nearly all respondents indicated that nutrition was prepared within the hospital (175/201 [87.1%; 95% CI 81.7-91.0%]), 26 (12.9%; 95% CI 9.0-18.3%) reported occasional reliance on patient relatives to arrange feeds. Nutritional calculations were most commonly performed collaboratively by both intensivists and dietitians (106/200 [53.0%; 95% CI 46.1-59.8%]), while 39 (19.5%; 95% CI 14.6-25.5%) relied solely on intensivists and 55 (27.5%; 95% CI 21.8-34.1%) on dietitians. One hundred and fifty-nine respondents (79.1%; 95% CI 73.0-84.2%) reported familiarity with established nutritional guidelines. (Figure 3).
Figure 3. Nutritional organisation and practice in the ICU.
Overview of institutional nutrition-related practices. Panels illustrate who arranges patient nutrition (hospital vs relatives), who performs nutritional calculations (intensivist, dietician, or both), awareness of established nutritional protocols, availability of a dedicated ICU dietician, use of standardised formulae, types of formula applied, and use of severity-based multiplication factors. All values represent percentages of respondents (N = 201), error bars represent 95% CI.
Access to dedicated ICU dietitians was limited, with only 61 respondents (30.3%; 95% CI 24.4-37.0%) reporting their availability. Standard nutritional formulas were widely used (185/201 [92.0%; 95% CI 87.5-95.0%]); among those using a formula, 79/184 (42.9%; 95% CI 36.0-50.2%) used other standard formulas, 67 (36.4%; 95% CI 29.8-43.6%) used Harris-Benedict, and only 12 (6.5%; 95% CI 3.8-11.1%) reported access to indirect calorimetry. Enteral feeding was the preferred initial route for 192 respondents (95.5%; 95% CI 91.7-97.6%). One hundred and sixty-one (80.1%; 95% CI 74.0-85.0%) initiated enteral nutrition early after ICU admission without contraindications, whereas 39 (19.4%; 95% CI 14.5-25.4%) deferred initiation to the treating physician’s or surgeon’s order.
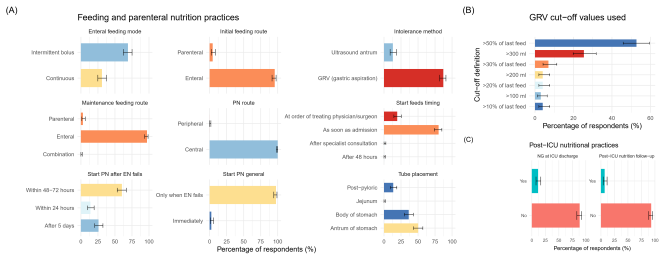
On day one, 57 respondents (28.4%; 95% CI 22.6-35.0%) achieved full caloric targets. When enteral feeding failed, 196 (97.5%; 95% CI 94.3-98.9%) transitioned to parenteral nutrition. Gastric residual volume (GRV) assessment was used by 175 (87.1%; 95% CI 81.7-91.0%) to evaluate feed intolerance, with thresholds varying: 106 (52.7%; 95% CI 45.8-59.5%) used >50% of the previous feed as the cutoff, 51 (25.4%; 95% CI 19.9-31.8%) used >300 ml, and the remainder used lower absolute volumes. Parenteral nutrition was most commonly initiated within 48–72 hours after persistent intolerance (121/201 [60.2%; 95% CI 53.3-66.7%]) and exclusively via central venous access (201/201 [100%; 95% CI 98.1-100%]). (Figure 4).
Regarding tube placement, 101 respondents (50.2%; 95% CI 43.4-57.1%) used antral positioning, 73 (36.3%; 95% CI 30.0-43.2%) used the body of the stomach, and 27 (13.4%; 95% CI 9.4-18.8%) used post-pyloric placement. Intermittent bolus feeding was preferred by 139 (69.2%; 95% CI 62.5-75.1%) over continuous infusion (62/201 [30.8%; 95% CI 24.9-37.5%]). Nutritional assessment relied predominantly on serum protein or albumin levels (139/201 [69.2%; 95% CI 62.5-75.1%]), and 161 (80.1%; 95% CI 74.0-85.0%) underwent daily evaluations. Only 14 respondents (7.0%; 95% CI 4.2-11.4%) reported following up nutrition after ICU discharge, and 23 (11.4%; 95% CI 7.7-16.6%) discharged patients with nasogastric tubes still in place. (Figure 4).
Composite figure summarising key aspects of nutritional management. (A) Enteral and parenteral feeding practices, including preferred initial and maintenance feeding routes, timing of feed initiation, methods used to assess feed intolerance, parenteral nutrition (PN) initiation criteria, PN route, enteral feeding mode, and feeding-tube placement. (B) Gastric residual volume (GRV) thresholds used by respondents to define enteral feed intolerance. (C) Post-ICU nutrition-related practices, including follow-up of nutritional status and opinions regarding discharge with a nasogastric tube. Data represent the percentage of respondents (N = 201), error bars represent 95% CI, EN – Enteral Nutrition.
4. Discussion
This cross-sectional survey of 201 intensivists reveals that while foundational nutritional principles are broadly endorsed early enteral nutrition was initiated by 80.1% (95% CI 74.0-85.0%) and standardised formulas were used by 92.0% (95% CI 87.5-95.0%), substantial practice heterogeneity persists in several critical domains. Access to dedicated ICU dietitians remained low (30.3%; 95% CI 24.4-37.0%), and indirect calorimetry was available to only 6.5% (95% CI 3.8-11.1%) of respondents. Feeding intolerance assessment relied predominantly on gastric residual volume measurement (87.1%; 95% CI 81.7-91.0%), yet the thresholds applied varied widely, with roughly half using a proportional cutoff (>50% of the previous feed) and a quarter using an absolute volume of >300 ml. Full caloric targets on day one were achieved by only 28.4% (95% CI 22.6-35.0%), and parenteral nutrition, when required, was most commonly delayed to 48-72 hours after enteral failure (60.2%; 95% CI 53.3-66.7%). Perhaps most notably, structured post-ICU nutritional follow-up was reported by only 7.0% (95% CI 4.2-11.4%) of intensivists, and just 11.4% (95% CI 7.7-16.6%) discharged patients with nasogastric tubes in situ, suggesting that the transition from ICU to ward represents a major gap in the continuity of nutritional care.
The present survey offers valuable insights into real-world nutritional practices among intensivists and highlights several persistent gaps between recommended guidelines and their practical application. Respondents were generally experienced clinicians, yet considerable variability in nutritional strategies was observed across multiple care domains. These findings mirror international concerns regarding inconsistent delivery of evidence-based nutritional therapy in critical illness, despite its recognised impact on outcomes such as infection risk, ventilator dependence, muscle preservation, and mortality
[1]
Lambell KJ, Tatucu-Babet OA, Chapple LA, Gantner D, Ridley EJ. Nutrition therapy in critical illness: a review of the literature for clinicians. Crit Care. 2020; 24(1): 35.
Moisey LL, Merriweather JL, Drover JW. The role of nutrition rehabilitation in the recovery of survivors of critical illness: underrecognized and underappreciated. Crit Care. 2022; 26: 270.
A prominent observation was the low prevalence of closed ICU models, reported by only 22% of participants. Closed ICUs, with intensivist-led decision-making, have consistently demonstrated improved outcomes partly attributable to more standardised and coordinated care, including nutrition delivery.
[4]
Ghorra S, Reinert SE, Cioffi W, Buczko G, Simms HH. Analysis of the effect of conversion from open to closed surgical intensive care unit. Ann Surg. 1999; 229: 163–171.
Belkin O, Fernandez-Nava L, Sheikh M, Pang A, Schmitz B, Vogt C, et al. The benefits of a closed ICU: a systematic review. The Southwest Respiratory and Critical Care Chronicles. 2024; 12(50): 30–37.
The predominance of semi-open or open formats may therefore contribute to inconsistent adherence to nutritional protocols. Compounding this challenge, only one-third of intensivists were continuously present in the ICU, despite continuous in-house coverage being associated with improved quality of care and increased patient and family satisfaction.
[6]
Gajic O, Afessa B, Hanson AC, Krpata T, Yilmaz M, Mohamed SF, et al. Effect of 24-hour mandatory versus on-demand critical care specialist presence on quality of care and family and provider satisfaction in the intensive care unit of a teaching hospital. Crit Care Med. 2008; 36(1): 36–44.
Such staffing and organisational limitations likely hinder the timely initiation and monitoring of nutritional therapy.
Resource distribution also shaped practice patterns. Most respondents practiced in private ICUs and urban or metropolitan settings, reflecting the concentration of advanced critical care infrastructure in these regions.
[7]
Ramakrishnan A, Ramakrishnan N. Critical Care Delivery in India: Stats, State(s) and Strategies. Indian J Crit Care Med. 2023; 27(4): 231–232.
Nonetheless, 13% reported reliance on externally sourced enteral feeds, despite recommendations that all formulas be prepared within the institution to minimize the risk of contamination.
[8]
Mokhalalati JK, Druyan ME, Shott SB, Comer GM. Microbial, nutritional and physical quality of commercial and hospital prepared tube feedings in Saudi Arabia. Saudi Med J. 2004; 25(3): 331–341.
[8]
This highlights infrastructural gaps that may directly affect the safety of nutritional delivery.
Although a majority of respondents collaborated with dietitians, only 40% had access to a dedicated ICU dietitian. A multidisciplinary approach, including dietitians, nurses, physiotherapists, and physicians, is essential for accurate nutritional assessment and optimal delivery.
[9]
Cahill NE, Murch L, Cook D, Heyland DK; Canadian Critical Care Trials Group. Barriers to feeding critically ill patients: a multicenter survey of critical care nurses. J Crit Care. 2012; 27(6): 727-734.
Dietitian shortages represent a recognised global barrier to high-quality nutritional care.
[10]
Fadeur M, Preiser JC, Verbrugge AM, Misset B, Rousseau AF. Oral Nutrition during and after Critical Illness: SPICES for Quality of Care! Nutrients. 2020; 12(11): 3509.
Encouragingly, 80% of respondents reported familiarity with established guidelines, and 92% used standardised formulas, reflecting a strong foundational knowledge base. However, indirect calorimetry, the gold standard for determining caloric needs, was used by only 12%.
[11]
Allingstrup MJ, Kondrup J, Wiis J, Claudius C, Pedersen UG, Hein-Rasmussen R, et al. Early goal-directed nutrition versus standard of care in adult intensive care patients: the single-centre, randomised, outcome assessor-blinded EAT-ICU trial. Intensive Care Med. 2017; 43(11): 1637-1647.
This limited availability is common worldwide and necessitates reliance on predictive equations, which may increase the risk of under- or overfeeding in metabolically unstable patients.
[12]
Reignier J, Rice TW, Arabi YM, Casaer M. Nutritional Support in the ICU. BMJ. 2025; 388: e077979.
Respondents widely endorsed early enteral nutrition, aligning with guideline recommendations advocating initiation within 24–48 hours of ICU admission in hemodynamically stable patients.
[13]
Singer P, Blaser AR, Berger MM, Alhazzani W, Calder PC, Casaer MP, et al. ESPEN guideline on clinical nutrition in the intensive care unit. Clin Nutr. 2019; 38(1): 48–79.
Early feeding has been shown to have benefits, including reduced infectious complications, shorter ICU stays, and a lower incidence of multiple organ dysfunction. However, only 28% achieved full caloric targets on day one, consistent with cautionary guidance to avoid rapid escalation in high-risk patients due to the risk of metabolic intolerance and refeeding complications.
[14]
DOIg GS, Simpson F, Heighes PT, Bellomo R, Chesher D, Caterson ID, et al. Restricted versus continued standard caloric intake during the management of refeeding syndrome in critically ill adults: a randomised, parallel-group, multicentre, single-blind controlled trial. Lancet Respir Med. 2015; 3(12): 943-952.
In stable patients, immediate caloric achievement may be reasonable, but careful monitoring remains essential.
[15]
Desachy A, Clavel M, Vuagnat A, Normand S, Gissot V, François B. Initial efficacy and tolerability of early enteral nutrition with immediate or gradual introduction in intubated patients. Intensive Care Med. 2008; 34(6): 1054-1059.
Nearly all participants transitioned to parenteral nutrition (PN) when enteral intake was inadequate. While guidelines recommend considering supplemental PN when enteral nutrition fails to meet ≥60% of targets by day 3, the survey revealed considerable variation in timing, with some intensivists delaying PN beyond 5 days of intolerance.
[16]
Bayer-Berger M, Chioléro R, Freeman J, Hirschi B. Incidence of phlebitis in peripheral parenteral nutrition: effect of the different nutrient solutions. Clin Nutr. 1989; 8(4): 181-186.
Delays in PN may exacerbate cumulative caloric deficits and protein catabolism, particularly in catabolic conditions such as sepsis or trauma.
Feeding intolerance assessment exhibited marked heterogeneity. Most respondents relied on GRV measurements, although thresholds varied widely, ranging from more than 50% of the previous feed to fixed volumes, such as 300 ml. This variability aligns with the broader literature, which reflects significant inconsistency in definitions of feeding intolerance and GRV cutoffs, reported to range from 50 to 500 ml.
[17]
Blaser AR, Starkopf J, Kirsimägi Ü, Deane AM. Definition, prevalence, and outcome of feeding intolerance in intensive care: a systematic review and meta-analysis. Acta Anaesthesiol Scand. 2014; 58(8): 914-922.
Contemporary guidelines recommend using higher thresholds (approximately 500 ml) and incorporating clinical symptoms, as overly conservative cutoffs may lead to unnecessary feed interruptions and undernutrition.
[18]
Reintam Blaser A, Starkopf J, Alhazzani W, Berger MM, Casaer MP, Deane AM, et al. Early enteral nutrition in critically ill patients: ESICM clinical practice guidelines. Intensive Care Med. 2017; 43(3): 380-398.
McClave SA, Taylor BE, Martindale RG, Warren MM, Johnson DR, Braunschweig C, et al. Guidelines for the Provision and Assessment of Nutrition Support Therapy in the Adult Critically Ill Patient: Society of Critical Care Medicine (SCCM) and American Society for Parenteral and Enteral Nutrition (A.S.P.E.N.). JPEN J Parenter Enteral Nutr. 2016; 40(2): 159-211.
Some respondents applied considerably lower thresholds, echoing earlier studies that advocate for GRVs between 50 and 200 ml.
[20]
Reintam Blaser A, Padar M, Mändul M, Elke G, Engel C, Fischer K, et al. Development of the Gastrointestinal Dysfunction Score (GIDS) for critically ill patients - A prospective multicenter observational study (iSOFA study). Clin Nutr. 2021; 40(8): 4932-4940.
Ozen N, Blot S, Ozen V, Arikan Donmez A, Gurun P, Cinar FI, et al. Gastric residual volume measurement in the intensive care unit: an international survey reporting nursing practice. Nurs Crit Care. 2018; 23(5): 263-269.
The continued reliance on low cutoffs underscores the need for harmonised institutional guidance and educational interventions. Although gastric ultrasound has shown promise for assessing gastric volume,
[22]
Sharma V, Gudivada D, Gueret R, Bailitz J. Ultrasound-Assessed Gastric Antral Area Correlates With Aspirated Tube Feed Volume in Enterally Fed Critically Ill Patients. Nutr Clin Pract. 2017; 32(2): 206-211.
it was not reported in this survey, consistent with its limited uptake globally.
Feeding modality also varied, with intermittent bolus feeding preferred by many respondents. Intermittent feeding offers practical advantages, such as reduced infusion time and convenience for gastric placement, yet it increases the risk of gastrointestinal symptoms, including vomiting or diarrhoea, in situations where continuous feeding may be superior.
[23]
Bankhead R, Boullata J, Brantley S, Corkins M, Guenter P, Krenitsky J, et al. Enteral nutrition practice recommendations. JPEN J Parenter Enteral Nutr. 2009; 33(2): 122-167.
Enhanced access to expertise in post-pyloric tube placement may improve tolerance and reduce aspirations.
Nutritional assessment practices revealed a strong reliance on serum protein markers, particularly albumin. Although low albumin levels correlate with malnutrition in stable populations,
[26]
Zhang Z, Pereira SL, Luo M, Matheson EM. Evaluation of Blood Biomarkers Associated with Risk of Malnutrition in Older Adults: A Systematic Review and Meta-Analysis. Nutrients. 2017; 9(8): 829.
they are unreliable markers during acute illness due to their sensitivity to inflammation and fluid shifts. Prealbumin, with a shorter half-life, more accurately reflects short-term nutritional changes,
[27]
Takeda H, Ishihama K, Fukui T, Fujishima S, Orii T, Nakazawa Y, et al. Significance of rapid turnover proteins in protein-losing gastroenteropathy. Hepatogastroenterology. 2003; 50(54): 1963-1965.
[27]
yet its use was not prominent in the responses. Daily nutritional assessment, reported by 80% of respondents, is commendable and consistent with guidelines, especially in unstable patients.
A major gap identified was the lack of structured post-ICU nutritional follow-up. Only 7% of intensivists continued monitoring nutrition after ICU discharge, despite known challenges such as anorexia, dysphagia, altered taste, and ICU-acquired weakness, all of which reduce voluntary intake.
[2]
Moisey LL, Merriweather JL, Drover JW. The role of nutrition rehabilitation in the recovery of survivors of critical illness: underrecognized and underappreciated. Crit Care. 2022; 26: 270.
Post-ICU patients are at risk of persistent malnutrition, and caloric needs often increase during rehabilitation. Evidence increasingly supports the continuation of enteral feeding post-ICU discharge, which is associated with improved protein-calorie adequacy and reduced unplanned readmissions.
[28]
ApSimon M, Steel C, Johnston C, Winder B, Cohen S, Reichert H, et al. Enteral nutrition on discharge from intensive care and 30-day unplanned readmission: An exploratory, retrospective study of association. Clin Nutr ESPEN. 2024; 61: 15–21.
The finding that only 12% of patients were discharged with enteral tubes suggests substantial missed opportunities to optimise recovery, even though supplemental feeding can significantly improve long-term outcomes.
[29]
Rousseau AF, Lucania S, Fadeur M, Verbrugge AM, Cavalier E, Colson C, et al. Adequacy of Nutritional Intakes during the Year after Critical Illness: An Observational Study in a Post-ICU Follow-Up Clinic. Nutrients. 2022; 14(18): 3797.
This study has limitations. Survey data rely on self-reporting and are susceptible to recall and desirability bias. Representation was skewed toward urban private hospitals, and the absence of rural respondents limits generalisability. Moreover, the survey did not categorize outcomes by hospital level or resource capacity, which likely influences practice variability. Nevertheless, the findings underscore the need for locally adapted, evidence-based nutritional protocols, improved staff training, integration of dietitians, and a stronger emphasis on post-ICU nutritional continuity.
Overall, this survey highlights meaningful disparities between current ICU nutritional practices and guideline recommendations. Addressing these gaps through systematic protocol development, multidisciplinary education, and targeted resource strengthening is essential for enhancing the nutritional management of critically ill patients and improving their recovery trajectories.
5. Conclusion
This survey reveals substantial heterogeneity in ICU nutritional practices, with notable discrepancies between guideline recommendations and real-world implementation. While early enteral nutrition and guideline-based calculations are widely adopted, variability persists in assessing feeding intolerance, initiating parenteral nutrition, and providing post-ICU nutritional follow-up. Ensuring consistent, evidence-based nutritional care requires improved access to trained dietitians, standardized institutional protocols, enhanced professional training, and strengthened multidisciplinary collaboration. A unified approach to nutritional management has the potential to improve outcomes for critically ill patients and support better long-term recovery.
Lambell KJ, Tatucu-Babet OA, Chapple LA, Gantner D, Ridley EJ. Nutrition therapy in critical illness: a review of the literature for clinicians. Crit Care. 2020; 24(1): 35.
Moisey LL, Merriweather JL, Drover JW. The role of nutrition rehabilitation in the recovery of survivors of critical illness: underrecognized and underappreciated. Crit Care. 2022; 26: 270.
Elmezoughi E, de Vasconcellos K. An evaluation of feeding practices and determination of barriers to providing nutritional support in a multidisciplinary South African intensive care unit. South Afr J Crit Care. 2020; 36(1).
Ghorra S, Reinert SE, Cioffi W, Buczko G, Simms HH. Analysis of the effect of conversion from open to closed surgical intensive care unit. Ann Surg. 1999; 229: 163–171.
Belkin O, Fernandez-Nava L, Sheikh M, Pang A, Schmitz B, Vogt C, et al. The benefits of a closed ICU: a systematic review. The Southwest Respiratory and Critical Care Chronicles. 2024; 12(50): 30–37.
Gajic O, Afessa B, Hanson AC, Krpata T, Yilmaz M, Mohamed SF, et al. Effect of 24-hour mandatory versus on-demand critical care specialist presence on quality of care and family and provider satisfaction in the intensive care unit of a teaching hospital. Crit Care Med. 2008; 36(1): 36–44.
Mokhalalati JK, Druyan ME, Shott SB, Comer GM. Microbial, nutritional and physical quality of commercial and hospital prepared tube feedings in Saudi Arabia. Saudi Med J. 2004; 25(3): 331–341.
[9]
Cahill NE, Murch L, Cook D, Heyland DK; Canadian Critical Care Trials Group. Barriers to feeding critically ill patients: a multicenter survey of critical care nurses. J Crit Care. 2012; 27(6): 727-734.
Fadeur M, Preiser JC, Verbrugge AM, Misset B, Rousseau AF. Oral Nutrition during and after Critical Illness: SPICES for Quality of Care! Nutrients. 2020; 12(11): 3509.
Allingstrup MJ, Kondrup J, Wiis J, Claudius C, Pedersen UG, Hein-Rasmussen R, et al. Early goal-directed nutrition versus standard of care in adult intensive care patients: the single-centre, randomised, outcome assessor-blinded EAT-ICU trial. Intensive Care Med. 2017; 43(11): 1637-1647.
Singer P, Blaser AR, Berger MM, Alhazzani W, Calder PC, Casaer MP, et al. ESPEN guideline on clinical nutrition in the intensive care unit. Clin Nutr. 2019; 38(1): 48–79.
DOIg GS, Simpson F, Heighes PT, Bellomo R, Chesher D, Caterson ID, et al. Restricted versus continued standard caloric intake during the management of refeeding syndrome in critically ill adults: a randomised, parallel-group, multicentre, single-blind controlled trial. Lancet Respir Med. 2015; 3(12): 943-952.
Desachy A, Clavel M, Vuagnat A, Normand S, Gissot V, François B. Initial efficacy and tolerability of early enteral nutrition with immediate or gradual introduction in intubated patients. Intensive Care Med. 2008; 34(6): 1054-1059.
Bayer-Berger M, Chioléro R, Freeman J, Hirschi B. Incidence of phlebitis in peripheral parenteral nutrition: effect of the different nutrient solutions. Clin Nutr. 1989; 8(4): 181-186.
Reintam Blaser A, Starkopf J, Alhazzani W, Berger MM, Casaer MP, Deane AM, et al. Early enteral nutrition in critically ill patients: ESICM clinical practice guidelines. Intensive Care Med. 2017; 43(3): 380-398.
McClave SA, Taylor BE, Martindale RG, Warren MM, Johnson DR, Braunschweig C, et al. Guidelines for the Provision and Assessment of Nutrition Support Therapy in the Adult Critically Ill Patient: Society of Critical Care Medicine (SCCM) and American Society for Parenteral and Enteral Nutrition (A.S.P.E.N.). JPEN J Parenter Enteral Nutr. 2016; 40(2): 159-211.
Reintam Blaser A, Padar M, Mändul M, Elke G, Engel C, Fischer K, et al. Development of the Gastrointestinal Dysfunction Score (GIDS) for critically ill patients - A prospective multicenter observational study (iSOFA study). Clin Nutr. 2021; 40(8): 4932-4940.
Ozen N, Blot S, Ozen V, Arikan Donmez A, Gurun P, Cinar FI, et al. Gastric residual volume measurement in the intensive care unit: an international survey reporting nursing practice. Nurs Crit Care. 2018; 23(5): 263-269.
Zhang Z, Pereira SL, Luo M, Matheson EM. Evaluation of Blood Biomarkers Associated with Risk of Malnutrition in Older Adults: A Systematic Review and Meta-Analysis. Nutrients. 2017; 9(8): 829.
Takeda H, Ishihama K, Fukui T, Fujishima S, Orii T, Nakazawa Y, et al. Significance of rapid turnover proteins in protein-losing gastroenteropathy. Hepatogastroenterology. 2003; 50(54): 1963-1965.
[28]
ApSimon M, Steel C, Johnston C, Winder B, Cohen S, Reichert H, et al. Enteral nutrition on discharge from intensive care and 30-day unplanned readmission: An exploratory, retrospective study of association. Clin Nutr ESPEN. 2024; 61: 15–21.
Rousseau AF, Lucania S, Fadeur M, Verbrugge AM, Cavalier E, Colson C, et al. Adequacy of Nutritional Intakes during the Year after Critical Illness: An Observational Study in a Post-ICU Follow-Up Clinic. Nutrients. 2022; 14(18): 3797.
Hazarika, A., Ganesh, V., Singla, K. (2026). Real-world Nutritional Management in the ICU: Findings from a Survey of Intensivist Practices and Challenges from a Developing Country. International Journal of Anesthesia and Clinical Medicine, 14(1), 84-91. https://doi.org/10.11648/j.ijacm.20261401.23
Hazarika, A.; Ganesh, V.; Singla, K. Real-world Nutritional Management in the ICU: Findings from a Survey of Intensivist Practices and Challenges from a Developing Country. Int. J. Anesth. Clin. Med.2026, 14(1), 84-91. doi: 10.11648/j.ijacm.20261401.23
Hazarika A, Ganesh V, Singla K. Real-world Nutritional Management in the ICU: Findings from a Survey of Intensivist Practices and Challenges from a Developing Country. Int J Anesth Clin Med. 2026;14(1):84-91. doi: 10.11648/j.ijacm.20261401.23
@article{10.11648/j.ijacm.20261401.23,
author = {Amarjyoti Hazarika and Venkata Ganesh and Karan Singla},
title = {Real-world Nutritional Management in the ICU: Findings from a Survey of Intensivist Practices and Challenges from a Developing Country},
journal = {International Journal of Anesthesia and Clinical Medicine},
volume = {14},
number = {1},
pages = {84-91},
doi = {10.11648/j.ijacm.20261401.23},
url = {https://doi.org/10.11648/j.ijacm.20261401.23},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ijacm.20261401.23},
abstract = {Objective: Although international guidelines outline best practices for assessing and delivering nutrition to critically ill patients, their implementation varies considerably across Intensive Care Units (ICUs). This study aimed to evaluate current nutritional practices among intensivists, identify challenges in meeting nutritional goals in the ICU, and describe strategies used for post-ICU nutritional care. Methods: An online survey was disseminated to certified intensivists, who were invited to complete a structured questionnaire electronically. Institutional ethics approval (INT/ECI2023/P2/1344) and clinical trial registration (CTRI/2024/01/061457) were obtained. Results: Of 201 respondents, 53% had more than 10 years of clinical experience, and 33% performed in-hospital ICU duties. Most institutions provided patient nutrition 79% reported awareness of established nutritional protocols, yet 69% cited the unavailability of qualified ICU dietitians. Only 6% used indirect calorimetry for caloric assessment. Enteral nutrition was initiated in 95% of patients, predominantly via intermittent bolus feeding (70%), and 80% commenced feeding soon after ICU admission when feasible. Feed intolerance was assessed in 87% of cases using gastric residual volumes, with a threshold of greater than 50% of the previous feed being the common criterion. Nearly 60% initiated parenteral nutrition within 48–72 hours of developing enteral feed intolerance. Protein or albumin levels were used by 69% to assess nutritional status. Only 7% reported structured post-ICU nutritional follow-up. Conclusions: Substantial variability exists in ICU nutritional practices, with limited adherence to international recommendations and significant resource-related barriers.},
year = {2026}
}
TY - JOUR
T1 - Real-world Nutritional Management in the ICU: Findings from a Survey of Intensivist Practices and Challenges from a Developing Country
AU - Amarjyoti Hazarika
AU - Venkata Ganesh
AU - Karan Singla
Y1 - 2026/04/07
PY - 2026
N1 - https://doi.org/10.11648/j.ijacm.20261401.23
DO - 10.11648/j.ijacm.20261401.23
T2 - International Journal of Anesthesia and Clinical Medicine
JF - International Journal of Anesthesia and Clinical Medicine
JO - International Journal of Anesthesia and Clinical Medicine
SP - 84
EP - 91
PB - Science Publishing Group
SN - 2997-2698
UR - https://doi.org/10.11648/j.ijacm.20261401.23
AB - Objective: Although international guidelines outline best practices for assessing and delivering nutrition to critically ill patients, their implementation varies considerably across Intensive Care Units (ICUs). This study aimed to evaluate current nutritional practices among intensivists, identify challenges in meeting nutritional goals in the ICU, and describe strategies used for post-ICU nutritional care. Methods: An online survey was disseminated to certified intensivists, who were invited to complete a structured questionnaire electronically. Institutional ethics approval (INT/ECI2023/P2/1344) and clinical trial registration (CTRI/2024/01/061457) were obtained. Results: Of 201 respondents, 53% had more than 10 years of clinical experience, and 33% performed in-hospital ICU duties. Most institutions provided patient nutrition 79% reported awareness of established nutritional protocols, yet 69% cited the unavailability of qualified ICU dietitians. Only 6% used indirect calorimetry for caloric assessment. Enteral nutrition was initiated in 95% of patients, predominantly via intermittent bolus feeding (70%), and 80% commenced feeding soon after ICU admission when feasible. Feed intolerance was assessed in 87% of cases using gastric residual volumes, with a threshold of greater than 50% of the previous feed being the common criterion. Nearly 60% initiated parenteral nutrition within 48–72 hours of developing enteral feed intolerance. Protein or albumin levels were used by 69% to assess nutritional status. Only 7% reported structured post-ICU nutritional follow-up. Conclusions: Substantial variability exists in ICU nutritional practices, with limited adherence to international recommendations and significant resource-related barriers.
VL - 14
IS - 1
ER -
Hazarika, A., Ganesh, V., Singla, K. (2026). Real-world Nutritional Management in the ICU: Findings from a Survey of Intensivist Practices and Challenges from a Developing Country. International Journal of Anesthesia and Clinical Medicine, 14(1), 84-91. https://doi.org/10.11648/j.ijacm.20261401.23
Hazarika, A.; Ganesh, V.; Singla, K. Real-world Nutritional Management in the ICU: Findings from a Survey of Intensivist Practices and Challenges from a Developing Country. Int. J. Anesth. Clin. Med.2026, 14(1), 84-91. doi: 10.11648/j.ijacm.20261401.23
Hazarika A, Ganesh V, Singla K. Real-world Nutritional Management in the ICU: Findings from a Survey of Intensivist Practices and Challenges from a Developing Country. Int J Anesth Clin Med. 2026;14(1):84-91. doi: 10.11648/j.ijacm.20261401.23
@article{10.11648/j.ijacm.20261401.23,
author = {Amarjyoti Hazarika and Venkata Ganesh and Karan Singla},
title = {Real-world Nutritional Management in the ICU: Findings from a Survey of Intensivist Practices and Challenges from a Developing Country},
journal = {International Journal of Anesthesia and Clinical Medicine},
volume = {14},
number = {1},
pages = {84-91},
doi = {10.11648/j.ijacm.20261401.23},
url = {https://doi.org/10.11648/j.ijacm.20261401.23},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ijacm.20261401.23},
abstract = {Objective: Although international guidelines outline best practices for assessing and delivering nutrition to critically ill patients, their implementation varies considerably across Intensive Care Units (ICUs). This study aimed to evaluate current nutritional practices among intensivists, identify challenges in meeting nutritional goals in the ICU, and describe strategies used for post-ICU nutritional care. Methods: An online survey was disseminated to certified intensivists, who were invited to complete a structured questionnaire electronically. Institutional ethics approval (INT/ECI2023/P2/1344) and clinical trial registration (CTRI/2024/01/061457) were obtained. Results: Of 201 respondents, 53% had more than 10 years of clinical experience, and 33% performed in-hospital ICU duties. Most institutions provided patient nutrition 79% reported awareness of established nutritional protocols, yet 69% cited the unavailability of qualified ICU dietitians. Only 6% used indirect calorimetry for caloric assessment. Enteral nutrition was initiated in 95% of patients, predominantly via intermittent bolus feeding (70%), and 80% commenced feeding soon after ICU admission when feasible. Feed intolerance was assessed in 87% of cases using gastric residual volumes, with a threshold of greater than 50% of the previous feed being the common criterion. Nearly 60% initiated parenteral nutrition within 48–72 hours of developing enteral feed intolerance. Protein or albumin levels were used by 69% to assess nutritional status. Only 7% reported structured post-ICU nutritional follow-up. Conclusions: Substantial variability exists in ICU nutritional practices, with limited adherence to international recommendations and significant resource-related barriers.},
year = {2026}
}
TY - JOUR
T1 - Real-world Nutritional Management in the ICU: Findings from a Survey of Intensivist Practices and Challenges from a Developing Country
AU - Amarjyoti Hazarika
AU - Venkata Ganesh
AU - Karan Singla
Y1 - 2026/04/07
PY - 2026
N1 - https://doi.org/10.11648/j.ijacm.20261401.23
DO - 10.11648/j.ijacm.20261401.23
T2 - International Journal of Anesthesia and Clinical Medicine
JF - International Journal of Anesthesia and Clinical Medicine
JO - International Journal of Anesthesia and Clinical Medicine
SP - 84
EP - 91
PB - Science Publishing Group
SN - 2997-2698
UR - https://doi.org/10.11648/j.ijacm.20261401.23
AB - Objective: Although international guidelines outline best practices for assessing and delivering nutrition to critically ill patients, their implementation varies considerably across Intensive Care Units (ICUs). This study aimed to evaluate current nutritional practices among intensivists, identify challenges in meeting nutritional goals in the ICU, and describe strategies used for post-ICU nutritional care. Methods: An online survey was disseminated to certified intensivists, who were invited to complete a structured questionnaire electronically. Institutional ethics approval (INT/ECI2023/P2/1344) and clinical trial registration (CTRI/2024/01/061457) were obtained. Results: Of 201 respondents, 53% had more than 10 years of clinical experience, and 33% performed in-hospital ICU duties. Most institutions provided patient nutrition 79% reported awareness of established nutritional protocols, yet 69% cited the unavailability of qualified ICU dietitians. Only 6% used indirect calorimetry for caloric assessment. Enteral nutrition was initiated in 95% of patients, predominantly via intermittent bolus feeding (70%), and 80% commenced feeding soon after ICU admission when feasible. Feed intolerance was assessed in 87% of cases using gastric residual volumes, with a threshold of greater than 50% of the previous feed being the common criterion. Nearly 60% initiated parenteral nutrition within 48–72 hours of developing enteral feed intolerance. Protein or albumin levels were used by 69% to assess nutritional status. Only 7% reported structured post-ICU nutritional follow-up. Conclusions: Substantial variability exists in ICU nutritional practices, with limited adherence to international recommendations and significant resource-related barriers.
VL - 14
IS - 1
ER -