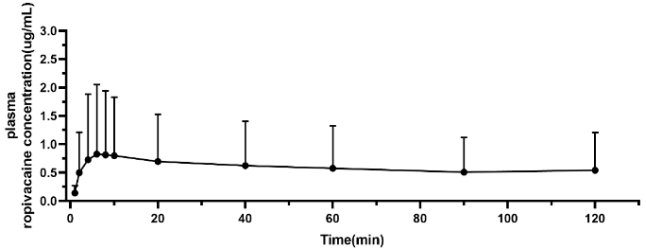
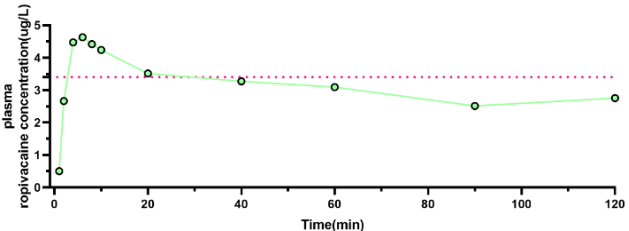
Background: Fascial plane block (FPB) has gained increasing clinical attention for its favorable safety and operational simplicity, yet its pharmacokinetic profiles and the associated risk of local anesthetic systemic toxicity (LAST) remain inadequately elucidated in clinical practice. Methods: A sample size calculation was performed based on the single-sample proportion formula, with a preset expected non-occurrence rate of LAST of 90%, a margin of error of 10%, and a 95% confidence level, determining a minimum sample size of 14 patients. A retrospective analysis was conducted on 14 patients with hip fracture undergoing total hip arthroplasty (THA) who received ultrasound-guided fascia iliaca compartment block (FICB) with 30 mL of 0.33% ropivacaine (100 mg) from July to September 2024. Plasma ropivacaine concentrations were measured at serial time points via high-performance liquid chromatography-tandem mass spectrometry (HPLC-MS/MS, Agilent 1290-6470, USA), and block-related adverse events were closely monitored. Results: No cases of LAST were observed in all patients. The mean peak plasma concentration (Cmax) of ropivacaine was 0.88±1.13 μg/mL, with a median time to peak concentration (Tmax) of 15 (interquartile range, 6–40) minutes; individual Cmax values ranged from 0.22 to 4.63 μg/mL. Statistical analysis revealed a significant negative correlation between Cmax and body mass index (BMI) (P<0.05), while Tmax showed no significant correlation with clinical characteristics including age and BMI (P>0.05). Conclusion: Ultrasound-guided FICB with 30 mL of 0.33% ropivacaine (100 mg) demonstrates good clinical safety in patients undergoing THA. Marked individual variability exists in plasma ropivacaine concentrations, and Cmax is negatively correlated with patient BMI.
| Published in | International Journal of Anesthesia and Clinical Medicine (Volume 14, Issue 1) |
| DOI | 10.11648/j.ijacm.20261401.19 |
| Page(s) | 53-60 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2026. Published by Science Publishing Group |
Fascia Iliaca Compartment Block, Ropivacaine, Pharmacokinetics, Plasma Concentration, Body Mass Index
Patient | Gender | Age (years) | Height (cm) | Weight (kg) | BMI (kg/m²) |
|---|---|---|---|---|---|
1 | Male | 69 | 165 | 75.0 | 27.55 |
2 | Male | 46 | 173 | 92.5 | 30.91 |
3 | Male | 26 | 170 | 50.0 | 17.30 |
4 | Male | 49 | 155 | 67.0 | 27.89 |
5 | Male | 66 | 175 | 60.0 | 19.59 |
6 | Male | 59 | 165 | 45.0 | 16.53 |
7 | Female | 67 | 142 | 45.5 | 22.56 |
8 | Female | 64 | 152 | 55.0 | 23.81 |
9 | Female | 72 | 155 | 51.0 | 21.23 |
10 | Female | 39 | 118 | 36.0 | 25.85 |
11 | Female | 70 | 156 | 58.5 | 24.04 |
12 | Male | 67 | 149 | 57.0 | 25.67 |
13 | Male | 51 | 168 | 62.0 | 21.97 |
14 | Male | 41 | 172 | 72.5 | 24.51 |
Max | — | 72 | 175 | 92.5 | 30.91 |
Min | — | 26 | 118 | 36.0 | 16.53 |
Mean | — | 56 | 158 | 59.1 | 23.53 |
SD | — | 14 | 15 | 13.9 | 3.90 |
Variables | Correlation coefficient | P value |
|---|---|---|
Cmax (μg/ml) | ||
BMI (kg/m²) | −0.552 | 0.041* |
Age (years) | −0.506 | 0.065 |
Sex | 0.300 | 0.297 |
Body weight (kg) | −0.158 | 0.590 |
Tmax (min) | ||
BMI (kg/m²) | 0.479 | 0.083 |
Age (years) | 0.293 | 0.309 |
Sex | −0.008 | 0.978 |
Body weight (kg) | 0.341 | 0.233 |
AUC | Area Under the Plasma Concentration-Time Curve |
BMI | Body Mass Index |
Cmax | Peak Plasma Concentration |
FPB | Fascial Plane Block |
FICB | Fascia Iliaca Compartment Block |
IQR | Interquartile Range |
LAST | Local Anesthetic Systemic Toxicity |
PNB | Peripheral Nerve Block |
SD | Standard Deviation |
THA | Total Hip Arthroplasty |
Tmax | Time to Peak Concentration |
VAS | Visual Analog Scale |
HPLC-MS/MS | High-Performance Liquid Chromatography-Tandem Mass Spectrometry |
ESRA | European Society of Regional Anesthesia and Pain Medicine |
CV | Coefficient of Variation |
OR | Odds Ratio |
| [1] | Chin K J, Lirk P, Hollmann M W, Schwarz S K W. Mechanisms of action of fascial plane blocks: a narrative review [J]. Regional Anesthesia and Pain Medicine, 2021, 46(7): 618-628. |
| [2] | Kim D H, Kim S J, Liu J, Beathe J, Memtsoudis S G. Fascial plane blocks: a narrative review of the literature [J]. Regional Anesthesia and Pain Medicine, 2021, 46(7): 600-617. |
| [3] | Chen L, Shen Y, Liu S, Cao Y, Zhu Z. Ultrasound-guided supra-inguinal fascia iliaca compartment block for older adults with hip fracture in the emergency department: a randomized controlled double-blind trial [J]. BMC Geriatrics, 2021, 21(1): 669. |
| [4] | Gao Y, Tan H, Sun R, Zhu J. Fascia iliaca compartment block reduces pain and opioid consumption after total hip arthroplasty: a systematic review and meta-analysis [J]. International Journal of Surgery, 2019, 65: 70-79. |
| [5] | Cooper G, Chan V W, White A C. Local anesthetic systemic toxicity: updated guidelines for management [J]. Anesthesiology, 2021, 134(1): 118-130. |
| [6] | Neal J M, Bernards C M, Butterworth J F 4th, et al. Third American Society of Regional Anesthesia and Pain Medicine/American Academy of Emergency Medicine guideline on the management of local anesthetic systemic toxicity [J]. Regional Anesthesia and Pain Medicine, 2018, 43(1): 17-34. |
| [7] | Elia N, Greco S, Casati A, Fanelli G. Pharmacokinetics of local anesthetics after peripheral nerve blocks: a narrative review [J]. European Journal of Anaesthesiology, 2018, 35(1): 36-48. |
| [8] | McLeod G A, Sawchuk R J, Katz J. Clinical pharmacokinetics of local anesthetics [J]. Clinical Pharmacokinetics, 1989, 16(5): 309-335. |
| [9] | Orebaugh S L, Trautmann K M. Local anesthetic systemic toxicity: recognition and management [J]. Journal of Emergency Medicine, 2020, 58(6): e135-e141. |
| [10] | Tsui B C, Finucane B T. Pharmacokinetics of ropivacaine: a review [J]. Clinical Pharmacokinetics, 1995, 28(1): 10-25. |
| [11] | Hadzic A, Arlotti M, Brandes S, et al. Practice guidelines for acute pain management in the perioperative setting: an updated report by the American Society of Anesthesiologists Task Force on Acute Pain Management [J]. Anesthesiology, 2020, 132(2): 322-344. |
| [12] | Knudsen K, Beckman Suurkula M, Blomberg S, Sjovall J, Edvardsson N. Central nervous and cardiovascular effects of i.v. infusions of ropivacaine, bupivacaine and placebo in volunteers [J]. British Journal of Anaesthesia, 1997, 78(5): 507-514. |
| [13] | Schwender D, Meissner K, Kretzschmar M, et al. CYP3A4/5 genetic polymorphisms affect ropivacaine metabolism and systemic toxicity risk [J]. Pharmacogenomics Journal, 2023, 23(2): 189-198. |
| [14] | Zhang F F, Lv C, Yang L Y, Wang S P, Zhang M, Guo X W. Pharmacokinetics of ropivacaine in elderly patients receiving fascia iliaca compartment block [J]. Experimental and Therapeutic Medicine, 2019, 18(4): 2648-2652. |
| [15] | Dalens B, Vanneuville G, Tanguy A. The fascia iliaca compartment block: a new approach to analgesia for the hip and thigh [J]. Anesthesia & Analgesia, 1989, 68(3): 392-395. |
| [16] | Li M, Wang H, Zhang Y, et al. Safety of fixed-volume ropivacaine for fascia iliaca compartment block in adult total hip arthroplasty: a multicenter retrospective study [J]. Journal of Orthopaedic Surgery and Research, 2023, 18(1): 512. |
| [17] | Schumann R, Kirchhoff C, Meier S, et al. Body mass index affects plasma concentrations of ropivacaine after ultrasound-guided transversus abdominis plane block [J]. Journal of Clinical Anesthesia, 2022, 76: 110646. |
| [18] | Wang X, Liu Y, Zhang L, et al. Low body mass index is an independent risk factor for elevated ropivacaine peak plasma concentration after fascia iliaca compartment block [J]. Regional Anesthesia and Pain Medicine, 2024, 49(3): 215-221. |
| [19] | Paut O, Schreiber E, Lacroix F, Meyrieux V, Simon N, Lavrut T, Camboulives J, Bruguerolle B. High plasma ropivacaine concentrations after fascia iliaca compartment block in children [J]. British Journal of Anaesthesia, 2004, 92(3): 416-418. |
| [20] | Garcia J, Fernandez M, Lopez R, et al. 3D reconstruction of the fascia iliaca compartment: age-related differences in vascular density and volume [J]. Clinical Anatomy, 2023, 36(5): 789-796. |
| [21] | Marhofer P, Schmid E, Willschke H, et al. Ultrasound-guided regional anesthesia: current perspectives [J]. British Journal of Anaesthesia, 2010, 104(1): 90-101. |
| [22] | White R D, Neilson C P. Adipose tissue as a determinant of local anesthetic pharmacokinetics after peripheral nerve block [J]. Anesthesiology, 2008, 109(3): 548-550. |
| [23] | Patel N, Smith A, Jones B, et al. Adipose tissue content and lipophilic local anesthetic pharmacokinetics: a meta-analysis of 12 clinical studies [J]. Anesthesia & Analgesia, 2022, 135(4): 892-901. |
| [24] | European Society of Regional Anesthesia and Pain Medicine (ESRA). Clinical Practice Guideline for Lower Extremity Fascial Plane Blocks [J]. Regional Anesthesia and Pain Medicine, 2023, 48(6): 497-510. |
| [25] | Rahiri J, Tuhoe J, Svirskis D, Lightfoot N J, Lirk P B, Hill A G. Systematic review of the systemic concentrations of local anaesthetic after transversus abdominis plane block and rectus sheath block [J]. British Journal of Anaesthesia, 2017, 118(4): 517-526. |
| [26] | Zhao J, Hu S, Chen W, et al. Incidence of local anesthetic systemic toxicity after ultrasound-guided fascia iliaca compartment block with large-volume local anesthetics: a national registry real-world study [J]. Anesthesiology, 2024, 140(2): 201-209. |
| [27] | Knezevic N N, Kanazi G E, Brull S J. Fascial plane blocks: a critical appraisal of the evidence [J]. Regional Anesthesia and Pain Medicine, 2019, 44(2): 208-220. |
| [28] | Smith T, Johnson R, Williams C, et al. Personalized fascial plane block dosing: a systematic review and future directions [J]. British Journal of Anaesthesia, 2024, 132(4): 689-700. |
| [29] | Brown J, Davis S, Miller T, et al. Surgical stress-induced changes in serum albumin and free local anesthetic concentration: a clinical study [J]. Anesthesia & Analgesia, 2023, 137(2): 312-319. |
APA Style
Liu, Y. (2026). Plasma Pharmacokinetics of Ropivacaine in Patients Undergoing Fascia Iliaca Compartment Block. International Journal of Anesthesia and Clinical Medicine, 14(1), 53-60. https://doi.org/10.11648/j.ijacm.20261401.19
ACS Style
Liu, Y. Plasma Pharmacokinetics of Ropivacaine in Patients Undergoing Fascia Iliaca Compartment Block. Int. J. Anesth. Clin. Med. 2026, 14(1), 53-60. doi: 10.11648/j.ijacm.20261401.19
@article{10.11648/j.ijacm.20261401.19,
author = {Yong Liu},
title = {Plasma Pharmacokinetics of Ropivacaine in Patients Undergoing Fascia Iliaca Compartment Block},
journal = {International Journal of Anesthesia and Clinical Medicine},
volume = {14},
number = {1},
pages = {53-60},
doi = {10.11648/j.ijacm.20261401.19},
url = {https://doi.org/10.11648/j.ijacm.20261401.19},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ijacm.20261401.19},
abstract = {Background: Fascial plane block (FPB) has gained increasing clinical attention for its favorable safety and operational simplicity, yet its pharmacokinetic profiles and the associated risk of local anesthetic systemic toxicity (LAST) remain inadequately elucidated in clinical practice. Methods: A sample size calculation was performed based on the single-sample proportion formula, with a preset expected non-occurrence rate of LAST of 90%, a margin of error of 10%, and a 95% confidence level, determining a minimum sample size of 14 patients. A retrospective analysis was conducted on 14 patients with hip fracture undergoing total hip arthroplasty (THA) who received ultrasound-guided fascia iliaca compartment block (FICB) with 30 mL of 0.33% ropivacaine (100 mg) from July to September 2024. Plasma ropivacaine concentrations were measured at serial time points via high-performance liquid chromatography-tandem mass spectrometry (HPLC-MS/MS, Agilent 1290-6470, USA), and block-related adverse events were closely monitored. Results: No cases of LAST were observed in all patients. The mean peak plasma concentration (Cmax) of ropivacaine was 0.88±1.13 μg/mL, with a median time to peak concentration (Tmax) of 15 (interquartile range, 6–40) minutes; individual Cmax values ranged from 0.22 to 4.63 μg/mL. Statistical analysis revealed a significant negative correlation between Cmax and body mass index (BMI) (P0.05). Conclusion: Ultrasound-guided FICB with 30 mL of 0.33% ropivacaine (100 mg) demonstrates good clinical safety in patients undergoing THA. Marked individual variability exists in plasma ropivacaine concentrations, and Cmax is negatively correlated with patient BMI.},
year = {2026}
}
TY - JOUR T1 - Plasma Pharmacokinetics of Ropivacaine in Patients Undergoing Fascia Iliaca Compartment Block AU - Yong Liu Y1 - 2026/03/09 PY - 2026 N1 - https://doi.org/10.11648/j.ijacm.20261401.19 DO - 10.11648/j.ijacm.20261401.19 T2 - International Journal of Anesthesia and Clinical Medicine JF - International Journal of Anesthesia and Clinical Medicine JO - International Journal of Anesthesia and Clinical Medicine SP - 53 EP - 60 PB - Science Publishing Group SN - 2997-2698 UR - https://doi.org/10.11648/j.ijacm.20261401.19 AB - Background: Fascial plane block (FPB) has gained increasing clinical attention for its favorable safety and operational simplicity, yet its pharmacokinetic profiles and the associated risk of local anesthetic systemic toxicity (LAST) remain inadequately elucidated in clinical practice. Methods: A sample size calculation was performed based on the single-sample proportion formula, with a preset expected non-occurrence rate of LAST of 90%, a margin of error of 10%, and a 95% confidence level, determining a minimum sample size of 14 patients. A retrospective analysis was conducted on 14 patients with hip fracture undergoing total hip arthroplasty (THA) who received ultrasound-guided fascia iliaca compartment block (FICB) with 30 mL of 0.33% ropivacaine (100 mg) from July to September 2024. Plasma ropivacaine concentrations were measured at serial time points via high-performance liquid chromatography-tandem mass spectrometry (HPLC-MS/MS, Agilent 1290-6470, USA), and block-related adverse events were closely monitored. Results: No cases of LAST were observed in all patients. The mean peak plasma concentration (Cmax) of ropivacaine was 0.88±1.13 μg/mL, with a median time to peak concentration (Tmax) of 15 (interquartile range, 6–40) minutes; individual Cmax values ranged from 0.22 to 4.63 μg/mL. Statistical analysis revealed a significant negative correlation between Cmax and body mass index (BMI) (P0.05). Conclusion: Ultrasound-guided FICB with 30 mL of 0.33% ropivacaine (100 mg) demonstrates good clinical safety in patients undergoing THA. Marked individual variability exists in plasma ropivacaine concentrations, and Cmax is negatively correlated with patient BMI. VL - 14 IS - 1 ER -
Department of Anesthesiology, West China Hospital, Sichuan University, Chengdu, China
Biography: Yong Liu is a physician in the Department of Anesthesiology at West China Hospital, Sichuan University. Dr. Liu received his Bachelor of Medicine degree from Xi'an Jiaotong University in 2020. He completed his standardized residency training in anesthesiology at West China Hospital, Sichuan University, in 2023. His current research interests focus on nerve block and clinical anesthesiology.
Research Fields: research field perioperative neurocognitive disorders, research field local anesthetic toxicity, research field nerve block, research field perioperative lung protection strategies, and research field clinical anesthesiology

Information