Background: Worldwide, the incidence of premature birth is increasing with its attending congenital anomalies, so complex surgical interventions to manage these congenital anomalies or complications are usually performed at early days of life. Neonates are vulnerable to apnea, and congenital cardiopulmonary problems and they have higher morbidity and mortality compared to older children and adults etc. In the preterm neonate, the risk of bronchopulmonary dysplasia and apnoea make their management complex and this is further compounded by their smaller size. Objective of study: The aim of the study was to determine the safety and efficacy of spinal anesthesia among neonates. Methodology: The study is a prospective study conducted in three tertiary health Institutions in northeast Nigeria. It includes all neonates scheduled for surgery amenable under SA. Sociodemographic variables, Haemodynamic variables, duration of surgery, and complications observed were all recorded. Results: Spinal anaesthesia SA was done in 230 patients, 90% of the patients were term, and only 10% were preterm. The majority were male with a mean weight of 3002 ± 660 grams and a mean age of 14.51±7.28 days. SA was successful in 93% of the patients in the first attempt. Heart rate, mean arterial pressure and oxygen saturation remained stable all through the duration of surgery. About 6% of the patients were converted to General Anaesthesia GA on account of prolonged surgery. The highest level of sympathetic block was recorded at the level of T4 while the lowest was at T6. Herniotomy was the most common surgery performed. The surgery lasted an average of 72 ± 28 minutes. No complication was recorded. Conclusion: Spinal anaesthesia provides a safe and reliable option for neonates who may require surgery early in life to improve their chances of survival. It serves as an alternative to GA with enhanced haemodynamic stability in this fragile population.
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited.
Spinal Anaesthesia, Preterm, Term Neonates, Haemodynamic Stability
1. Introduction
A full-term pregnancy typically lasts 40 weeks while a preterm is defined as a baby born alive before 37 weeks of pregnancy are completed. The preterm may not have fully developed vital organs such as the brain, kidneys liver, and lungs. The neonatal period is the first 28 days of life. Spinal anesthesia (SA) is also known as intrathecal or subarachnoid block. It is defined as the deposition of local anesthetic agents directly into the cerebrospinal fluid, resulting in dense surgical anesthesia inferior to the T8-9 dermatome. Subarachnoid block has shown a proven safety record, however its use as a substitute for General Anaesthesia (GA) in neonates, infants, and children has not been consistent over time
[1]
Whitaker EE, Wiemann BZ, DaJusta DG, Alpert SA, Ching CB, McLeod DJ, et al. Spinal anesthesia for pediatric urological surgery: reducing the theoretic neurotoxic effects of general anesthesia. Journal of pediatric urology. 2017; 13(4): 396-400.
. It has been used in term and preterm neonates undergoing surgery to reduce the risk of postoperative apnoea, desaturation, and bradycardia often associated with GA and to avoid possible neurotoxic effects of GA. Neonates are vulnerable to apnea, and congenital cardiopulmonary problems and they have higher morbidity and mortality compared to older children and adults, etc. In the preterm neonate, the risk of bronchopulmonary dysplasia and apnoea makes their management complex and this is further compounded by their smaller size
[2]
Williams RK, Adams DC, Aladjem EV, Kreutz JM, Sartorelli KH, Vane DW, et al. The safety and efficacy of spinal anesthesia for surgery in infants: the Vermont Infant Spinal Registry. Anesthesia & Analgesia. 2006; 102(1): 67-71.
. It is important to note that worldwide, the incidence of premature birth is increasing with its attending congenital anomalies, so complex surgical interventions to manage these congenital anomalies or complications are usually performed in early days of life. Some of these surgeries may be required to either improve the chances of survival or to correct a deformity, especially limb deformities. The preterm or term neonate may require surgery possibly on the second or third day of life to improve survival such as colostomy on account of imperforate anus. Other conditions include; testicular torsion, gastroschisis, omphalocele, necrotizing enterocolitis, incarcerated hernias, etc. SA offers an alternative to GA with enhanced haemodynamic stability in this fragile population. It provides an effective option for intra-operative and postoperative analgesia, allows for spontaneous ventilation, avoids airway manipulation and its attending risk, and also avoids multiple drug use associated with GA, especially opioid-related respiratory depression. SA is gaining popularity among Anaesthetists for use in neonates and infants to avoid the potential negative neurocognitive effects of GA
[3]
Subramaniam R. Anaesthetic concerns in preterm and term neonates. Indian Journal of Anaesthesia. 2019; 63(9): 771-9.
The study is a prospective study conducted in three tertiary health Institutions in northeast Nigeria. Institutional Ethical Clearance was obtained to conduct the study.
2.1. Inclusion and Exclusion Criteria
All the preterm and term neonates whose parents consented to participate in the study were included. Surgeries below the umbilicus such as herniotomy, colostomy, anal surgeries, and surgeries on the lower limb especially for correction of the defect, were included. Other surgeries included were omphalocele minor and major, gastroschisis repair, and surgeries on the genitourinary track. Surgeries lasting not more than 90 minutes were included. Patients whose parents or guardians refused to consent or have bleeding disorders, infection around the spine, vertebrae anomaly, or signs of raised intracranial pressure were excluded.
2.2. Spinal Anaesthesia Technique
Participants in the study were reviewed a day before the scheduled surgery date if on the elective case or two hours before surgery if on the emergency list. Patients were all cannulated while in the ward. On arrival at the theatre, patients were laid down supine and monitors were attached to record the baseline haemodynamic parameters (Mean Arterial Pressure MAP, Oxygen saturation SPO2, Heart rate HR, and Temperature). Ringer’s lactate was the chosen maintenance fluid of choice. While in the supine position, patients were positioned in the slightly flexed lateral position and care is taken to keep the head in a neutral position while an assistant administered oxygen via face mask. While the procedure was ongoing, a gauze soaked in 10% dextrose water was used as a pacifier. The procedure was carried out under aseptic conditions. Either L4 - L5 intervertebral space or L5 - S1 was used. The trocar of a size 24G cannula was improvised as the spinal need. Successful lumbar puncture was indicated by the presence of clear free-flowing CSF and 1mg/kg of 0.5% Bupivacaine equivalent to 0.2ml/kg was deposited into the subarachnoid space. No adjuvant was used. Cold stimuli using an Alcohol swab was used to test the level of block. Patients were immediately returned to the supine position and basic haemodynamic parameters (MAP, SPO2, HR, Temp) were recorded at T1- (immediately after the patient was returned to the supine position) and then at 5-minute intervals throughout the operation period and then up to one hour while in the recovery room.
3. Results
Descriptive statistical analysis results were presented as proportions and percentages for categorical variables and mean and standard deviation for continuous variables.
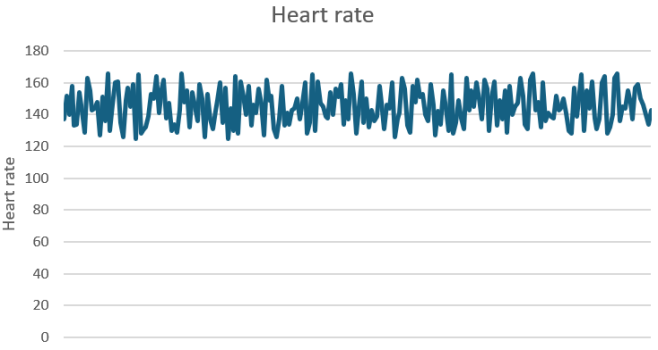
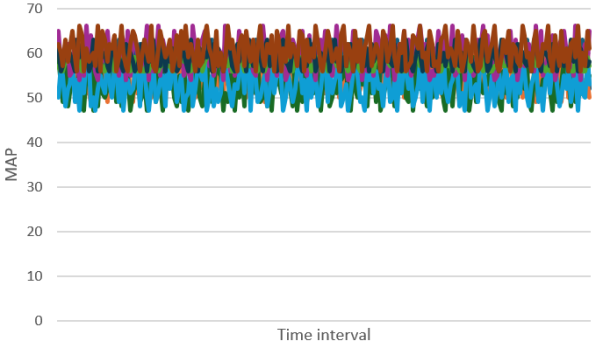
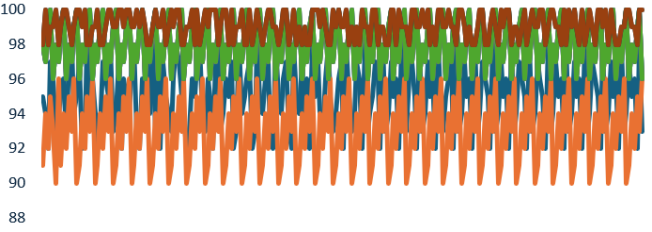
A total of 272 patients were screened for the study, however, only 230 preterm and termed neonates met the inclusion criteria. The majority of the patients (63%) were male. The mean age in days was 14.51 ± 7.728, mean weight in grams was 3002.37 ± 660.33. Only 10% (23) of the patients were preterm while the majority (90%) were term neonates. Indications for the surgery are presented in Table 1. Lumbar puncture was successful in the first attempt in 93% of the patients. Only 7% of the patients required a second attempt. Spinal Anaesthesia was successful in 96.8% of the patients. The highest level of block achieved was at the level of T4 while the lowest block was at T6. Supplemental anaesthesia using sevoflurane via facemask with or without intravenous fentanyl 1-2µg/kg was given in 3% of the patients. Only 6% of the patients needed conversion to General Anaesthesia on account of prolonged surgery. The mean duration of the surgery was 72 ± 28 minutes. Heart rate, Mean arterial pressure, and oxygen saturation remained stable throughout the surgery as shown in figures 1, 2 and 3 respectively. After a waiting period of 60 minutes in the recovery room to monitor the haemodynamic parameters (HR, MAP, SPO2 and Temperature) and any other complication that may arise, patients were transported back to the special care baby unit. No complication was observed in any of the patients.
Table 1. Type of Surgeries by specialty.
S/no
Specialty
Examples of procedure
Percentage
1.
General Surgery 1
Herniotomy
26.6%
2.
General Surgery 2
Colostomy, Gastrostomy, Exploratory laparotomy, Closure of gastrochisis, Repair of omphalocele minor, Rectal biopsy
Preterm and term neonates may require surgery during this early stage of life. Different anesthetic techniques such as general anesthesia, general anesthesia combined with either spinal or epidural anesthesia, SA alone, and SA combined with epidural anesthesia are available options to be used. SA has been established as an efficient and safe technique, with minimal cardiorespiratory disturbance when administered in the neonatal period
[4]
Sola C, Hertz L, Bringuier S, De La Arena P, Macq C, Deziel-Malouin S, et al. Spinal anaesthesia in neonates and infants: what about the cerebral oxygen saturation? BJA: British Journal of Anaesthesia. 2017; 119(5): 964-71.
. Spinal anaesthesia has been performed with success in the USA, Europe, and even in Africa. In 2012, Ilhan et al reported the successful repair of duodenal atresia in a low-birth-weight neonate under SA in Turkey
[5]
Ciftci I, Apiliogullari S, Kara I, Gunduz E, Duman A. Repair of duodenal atresia under spinal anesthesia in a low-birth-weight preterm neonate: case report. Journal of Pediatric Surgery. 2012; 47(8): e33-e5.
. In 2020, Randriamizao et al in a retrospective study reported the successful use of SA in 69 neonates and infants in Antananarivo, Madagascar
[6]
Randriamizao HM, Rakotondrainibe A, Razafindrabekoto LD, Ravoaviarivelo PF, Rajaonera AT, Andriamanarivo ML. Use of spinal anaesthesia in neonates and infants in Antananarivo, Madagascar: a retrospective descriptive study. BMC Research Notes. 2020; 13: 1-6.
. Ela AA et al reported the successful administration of spinal anaesthesia in 55 neonates and infants
[7]
Ela AA, Ngayap G, Etoundi PO, Esiene A, Bengono R, Mikone A. La rachianesthésie chez l’enfant: bilan d’une année d’expérience à l’Hôpital Central de Yaoundé. Health Sciences and Disease. 2013; 14(4).
[7]
. Reported cases of failed SA in neonates and infants ranges between 1 and 10%
[8]
Puncuh F, Lampugnani E, Kokki H. Use of spinal anaesthesia in paediatric patients: a single centre experience with 1132 cases. Pediatric anesthesia. 2004; 14(7): 564-7.
Ecoffey C, Lacroix F, Giaufré E, Orliaguet G, Courrèges P, Française AdARPdE. Epidemiology and morbidity of regional anesthesia in children: a follow-up one-year prospective survey of the French-Language Society of Paediatric Anaesthesiologists (ADARPEF). Pediatric Anesthesia. 2010; 20(12): 1061-9.
. In our study, spinal anaesthesia was successful in about 96.8% (223) of the patients. This is similar to findings by Williams et al in their study titled the safety and Efficacy of spinal anaesthesia for Surgery in infants
[2]
Williams RK, Adams DC, Aladjem EV, Kreutz JM, Sartorelli KH, Vane DW, et al. The safety and efficacy of spinal anesthesia for surgery in infants: the Vermont Infant Spinal Registry. Anesthesia & Analgesia. 2006; 102(1): 67-71.
. Similar results (94.2%) were obtained by Randriamizao et al, and 95.3% were reported successful by Kachko L et al.
[6]
Randriamizao HM, Rakotondrainibe A, Razafindrabekoto LD, Ravoaviarivelo PF, Rajaonera AT, Andriamanarivo ML. Use of spinal anaesthesia in neonates and infants in Antananarivo, Madagascar: a retrospective descriptive study. BMC Research Notes. 2020; 13: 1-6.
Kachko L, Simhi E, Tzeitlin E, Efrat R, Tarabikin E, Peled E, et al. Spinal anesthesia in neonates and infants–a single-center experience of 505 cases. Pediatric Anesthesia. 2007; 17(7): 647-53.
In a meta-analysis to determine whether SA reduces intraoperative and postoperative complications compared with GA, Dorms K et al reported that SA is at least as safe as GA for inguinal hernia repair in preterm neonates
[12]
Dohms K, Hein M, Rossaint R, Coburn M, Stoppe C, Ehret CB, et al. Inguinal hernia repair in preterm neonates: is there evidence that spinal or general anaesthesia is the better option regarding intraoperative and postoperative complications? A systematic review and meta-analysis. BMJ open. 2019; 9(10): e028728.
The majority of our patients (63%) were male, which is similar to studies by Ela AA et al, Randriamizao et al, and Nicola D et al
[6]
Randriamizao HM, Rakotondrainibe A, Razafindrabekoto LD, Ravoaviarivelo PF, Rajaonera AT, Andriamanarivo ML. Use of spinal anaesthesia in neonates and infants in Antananarivo, Madagascar: a retrospective descriptive study. BMC Research Notes. 2020; 13: 1-6.
Ela AA, Ngayap G, Etoundi PO, Esiene A, Bengono R, Mikone A. La rachianesthésie chez l’enfant: bilan d’une année d’expérience à l’Hôpital Central de Yaoundé. Health Sciences and Disease. 2013; 14(4).
[6, 7]
. This may not be unconnected with the fact that genitourinary surgeries and herniotomies which form up to 49% of the total procedure we performed are usually more common in the males than the females. Lloyd JC et al reported the absence of any female in 977 patients in a study to determine those diagnosed with Epispadia from 1997-2009
[13]
Lloyd JC, Wiener JS, Gargollo PC, Inman BA, Ross SS, Routh JC. Contemporary epidemiological trends in complex congenital genitourinary anomalies. The Journal of urology. 2013; 190(4): 1590-5.
. Hayaran et al reported males in their study titled Anaesthesia for genitourinary surgeries in neonates.
The mean age in our study was 14.51 ± 7.728 days while the mean weight was 3002.37 ± 660.33 grams. Shenkman Z et al reported a mean weight of 2140gram in their study while Disma et al reported 3286 ± 525 grams
[14]
Shenkman Ze, Erez I, Freud E, Arnon S. Risk factors for spinal anesthesia in preterm infants undergoing inguinal hernia repair. Jornal de Pediatria. 2012; 88: 222-6.
Disma N, Veyckemans F, Virag K, Hansen TG, Becke K, Harlet P, et al. Morbidity and mortality after anaesthesia in early life: results of the European prospective multicentre observational study, neonate and children audit of anaesthesia practice in Europe (NECTARINE). British journal of anaesthesia. 2021; 126(6): 1157-72.
Herniotomy was indicated in 26.6% of the patients, genitourinary surgeries were 22%, abdominal surgery in 21%, lower limb surgery 13%, while 17.4% were neurosurgeries. Herniotomy was the most common procedure performed. Among the genitourinary surgeries were hydrocelectomy, orchidectomy, hypospadias repairs, and bladder exploration. The abdominal surgeries included gastroschisis, repair of omphalocele, colostomy, and exploratory laparotomy.
Lumbar puncture was successful in 93% of the patients in the first attempt while only 7% required a second attempt. Spinal anaesthesia was successful in 96.8%. these findings are similar to studies reported by Randriamizao et al (94.2%), 97.4% by Williams et al and 92.5% by Dorms et al, and 91.4% by Frumiento et al
[2]
Williams RK, Adams DC, Aladjem EV, Kreutz JM, Sartorelli KH, Vane DW, et al. The safety and efficacy of spinal anesthesia for surgery in infants: the Vermont Infant Spinal Registry. Anesthesia & Analgesia. 2006; 102(1): 67-71.
Randriamizao HM, Rakotondrainibe A, Razafindrabekoto LD, Ravoaviarivelo PF, Rajaonera AT, Andriamanarivo ML. Use of spinal anaesthesia in neonates and infants in Antananarivo, Madagascar: a retrospective descriptive study. BMC Research Notes. 2020; 13: 1-6.
Dohms K, Hein M, Rossaint R, Coburn M, Stoppe C, Ehret CB, et al. Inguinal hernia repair in preterm neonates: is there evidence that spinal or general anaesthesia is the better option regarding intraoperative and postoperative complications? A systematic review and meta-analysis. BMJ open. 2019; 9(10): e028728.
. Only 6% of the patients needed conversion to GA.
Patients remained haemodynamically stable throughout the surgery. None of the patients developed apnoea, bradycardia or hypoxaemia. Heart remained stable all through the surgery and up to one hour postoperatively while the patient was being observed in the recovery. Oxygen saturation measured with a pulse oximeter ranges between 92-100% intra and post-operatively. Jones LJ et al, Tirmizi H et al and Gerber AC et al all reported the absence of bradycardia, apnea, and desaturation in high-risk neonates and infants
[17]
Jones LJ, Craven PD, Lakkundi A, Foster JP, Badawi N. Regional (spinal, epidural, caudal) versus general anaesthesia in preterm infants undergoing inguinal herniorrhaphy in early infancy. Cochrane database of systematic reviews. 2015(6).
Gerber AC, Weiss M. Awake spinal or caudal anaesthesia in preterms for herniotomies: what is the evidence based benefit compared with general anaesthesia? Current Opinion in Anesthesiology. 2003; 16(3): 315-20.
. On the other hand, complications such as bradycardia, hypotension, high block and apnoea were reported by
[2]
Williams RK, Adams DC, Aladjem EV, Kreutz JM, Sartorelli KH, Vane DW, et al. The safety and efficacy of spinal anesthesia for surgery in infants: the Vermont Infant Spinal Registry. Anesthesia & Analgesia. 2006; 102(1): 67-71.
Puncuh F, Lampugnani E, Kokki H. Use of spinal anaesthesia in paediatric patients: a single centre experience with 1132 cases. Pediatric anesthesia. 2004; 14(7): 564-7.
Ecoffey C, Lacroix F, Giaufré E, Orliaguet G, Courrèges P, Française AdARPdE. Epidemiology and morbidity of regional anesthesia in children: a follow-up one-year prospective survey of the French-Language Society of Paediatric Anaesthesiologists (ADARPEF). Pediatric Anesthesia. 2010; 20(12): 1061-9.
Kachko L, Simhi E, Tzeitlin E, Efrat R, Tarabikin E, Peled E, et al. Spinal anesthesia in neonates and infants–a single-center experience of 505 cases. Pediatric Anesthesia. 2007; 17(7): 647-53.
The surgery lasted an average of 72 ± 11 minutes. Ella et at reported a range from 25 to 78 min while Frumiento et al reported 15-130mins.
[7]
Ela AA, Ngayap G, Etoundi PO, Esiene A, Bengono R, Mikone A. La rachianesthésie chez l’enfant: bilan d’une année d’expérience à l’Hôpital Central de Yaoundé. Health Sciences and Disease. 2013; 14(4).
All patients were transported safely from the operating theatre to the special care baby unit of the participating hospitals one hour after close monitoring in the recovery room.
5. Conclusion
Spinal anaesthesia provides a safe and reliable option for neonates who may require surgery early in life to improve their chances of survival. It serves as an alternative to GA with enhanced haemodynamic stability in this fragile population. It is safe even in low-birth-weight patients. It provides an effective option for intra-operative and postoperative analgesia, allows for spontaneous ventilation, and avoids airway manipulation, and the use of multiple drugs associated with GA.
6. Limitation
At the onset of the study, size 26/27G quincke spinal needle was to be used, all site investigators reported difficulty with the use of the spinal needle. Due to the lack of the appropriate length needle, we improvised the trocar of a size 24G cannula and it was a success.
Abbreviations
GA
General Anaesthesia
HR
Heart Rate
MAP
Mean Arterial Pressure
SA
Spinal Anaesthesia
SPO2
Saturation of Oxygen
Acknowledgments
Prof. Ibironke Desalu read our article and gave advice.
Author Contributions
Adamu Yusuf Baffah: Conceptualization, Data curation, Formal Analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization
Abubakar Muhammad Ballah: Conceptualization, Data curation, Formal Analysis, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing
Whitaker EE, Wiemann BZ, DaJusta DG, Alpert SA, Ching CB, McLeod DJ, et al. Spinal anesthesia for pediatric urological surgery: reducing the theoretic neurotoxic effects of general anesthesia. Journal of pediatric urology. 2017; 13(4): 396-400.
Williams RK, Adams DC, Aladjem EV, Kreutz JM, Sartorelli KH, Vane DW, et al. The safety and efficacy of spinal anesthesia for surgery in infants: the Vermont Infant Spinal Registry. Anesthesia & Analgesia. 2006; 102(1): 67-71.
Sola C, Hertz L, Bringuier S, De La Arena P, Macq C, Deziel-Malouin S, et al. Spinal anaesthesia in neonates and infants: what about the cerebral oxygen saturation? BJA: British Journal of Anaesthesia. 2017; 119(5): 964-71.
Ciftci I, Apiliogullari S, Kara I, Gunduz E, Duman A. Repair of duodenal atresia under spinal anesthesia in a low-birth-weight preterm neonate: case report. Journal of Pediatric Surgery. 2012; 47(8): e33-e5.
Randriamizao HM, Rakotondrainibe A, Razafindrabekoto LD, Ravoaviarivelo PF, Rajaonera AT, Andriamanarivo ML. Use of spinal anaesthesia in neonates and infants in Antananarivo, Madagascar: a retrospective descriptive study. BMC Research Notes. 2020; 13: 1-6.
Ela AA, Ngayap G, Etoundi PO, Esiene A, Bengono R, Mikone A. La rachianesthésie chez l’enfant: bilan d’une année d’expérience à l’Hôpital Central de Yaoundé. Health Sciences and Disease. 2013; 14(4).
[8]
Puncuh F, Lampugnani E, Kokki H. Use of spinal anaesthesia in paediatric patients: a single centre experience with 1132 cases. Pediatric anesthesia. 2004; 14(7): 564-7.
Ecoffey C, Lacroix F, Giaufré E, Orliaguet G, Courrèges P, Française AdARPdE. Epidemiology and morbidity of regional anesthesia in children: a follow-up one-year prospective survey of the French-Language Society of Paediatric Anaesthesiologists (ADARPEF). Pediatric Anesthesia. 2010; 20(12): 1061-9.
Kachko L, Simhi E, Tzeitlin E, Efrat R, Tarabikin E, Peled E, et al. Spinal anesthesia in neonates and infants–a single-center experience of 505 cases. Pediatric Anesthesia. 2007; 17(7): 647-53.
Dohms K, Hein M, Rossaint R, Coburn M, Stoppe C, Ehret CB, et al. Inguinal hernia repair in preterm neonates: is there evidence that spinal or general anaesthesia is the better option regarding intraoperative and postoperative complications? A systematic review and meta-analysis. BMJ open. 2019; 9(10): e028728.
Shenkman Ze, Erez I, Freud E, Arnon S. Risk factors for spinal anesthesia in preterm infants undergoing inguinal hernia repair. Jornal de Pediatria. 2012; 88: 222-6.
Disma N, Veyckemans F, Virag K, Hansen TG, Becke K, Harlet P, et al. Morbidity and mortality after anaesthesia in early life: results of the European prospective multicentre observational study, neonate and children audit of anaesthesia practice in Europe (NECTARINE). British journal of anaesthesia. 2021; 126(6): 1157-72.
Jones LJ, Craven PD, Lakkundi A, Foster JP, Badawi N. Regional (spinal, epidural, caudal) versus general anaesthesia in preterm infants undergoing inguinal herniorrhaphy in early infancy. Cochrane database of systematic reviews. 2015(6).
Gerber AC, Weiss M. Awake spinal or caudal anaesthesia in preterms for herniotomies: what is the evidence based benefit compared with general anaesthesia? Current Opinion in Anesthesiology. 2003; 16(3): 315-20.
Baffah, A. Y., Ballah, A. M., Bidemi, Y. H., Mohammed, J. M., Njidda, G. A., et al. (2024). Assessing the Safety and Efficacy of Spinal Anesthesia in Preterm and Term Neonates: A Multicenter Experience. International Journal of Anesthesia and Clinical Medicine, 12(1), 47-52. https://doi.org/10.11648/j.ijacm.20241201.19
Baffah, A. Y.; Ballah, A. M.; Bidemi, Y. H.; Mohammed, J. M.; Njidda, G. A., et al. Assessing the Safety and Efficacy of Spinal Anesthesia in Preterm and Term Neonates: A Multicenter Experience. Int. J. Anesth. Clin. Med.2024, 12(1), 47-52. doi: 10.11648/j.ijacm.20241201.19
Baffah AY, Ballah AM, Bidemi YH, Mohammed JM, Njidda GA, et al. Assessing the Safety and Efficacy of Spinal Anesthesia in Preterm and Term Neonates: A Multicenter Experience. Int J Anesth Clin Med. 2024;12(1):47-52. doi: 10.11648/j.ijacm.20241201.19
@article{10.11648/j.ijacm.20241201.19,
author = {Adamu Yusuf Baffah and Abubakar Muhammad Ballah and Yahaya Halima Bidemi and Jika Mohammed Mohammed and Gyadale Abdulhamid Njidda and Nwokorie Rosemary Mabong and Galadima Hajara Aminu and Hassan Maina Ali and Ibrahim Naziru Joda and Abdullahi Muhammad Maryam and Adam Ibrahim Abdullahi and Andibanbang Franklin},
title = {Assessing the Safety and Efficacy of Spinal Anesthesia in Preterm and Term Neonates: A Multicenter Experience
},
journal = {International Journal of Anesthesia and Clinical Medicine},
volume = {12},
number = {1},
pages = {47-52},
doi = {10.11648/j.ijacm.20241201.19},
url = {https://doi.org/10.11648/j.ijacm.20241201.19},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ijacm.20241201.19},
abstract = {Background: Worldwide, the incidence of premature birth is increasing with its attending congenital anomalies, so complex surgical interventions to manage these congenital anomalies or complications are usually performed at early days of life. Neonates are vulnerable to apnea, and congenital cardiopulmonary problems and they have higher morbidity and mortality compared to older children and adults etc. In the preterm neonate, the risk of bronchopulmonary dysplasia and apnoea make their management complex and this is further compounded by their smaller size. Objective of study: The aim of the study was to determine the safety and efficacy of spinal anesthesia among neonates. Methodology: The study is a prospective study conducted in three tertiary health Institutions in northeast Nigeria. It includes all neonates scheduled for surgery amenable under SA. Sociodemographic variables, Haemodynamic variables, duration of surgery, and complications observed were all recorded. Results: Spinal anaesthesia SA was done in 230 patients, 90% of the patients were term, and only 10% were preterm. The majority were male with a mean weight of 3002 ± 660 grams and a mean age of 14.51±7.28 days. SA was successful in 93% of the patients in the first attempt. Heart rate, mean arterial pressure and oxygen saturation remained stable all through the duration of surgery. About 6% of the patients were converted to General Anaesthesia GA on account of prolonged surgery. The highest level of sympathetic block was recorded at the level of T4 while the lowest was at T6. Herniotomy was the most common surgery performed. The surgery lasted an average of 72 ± 28 minutes. No complication was recorded. Conclusion: Spinal anaesthesia provides a safe and reliable option for neonates who may require surgery early in life to improve their chances of survival. It serves as an alternative to GA with enhanced haemodynamic stability in this fragile population.
},
year = {2024}
}
TY - JOUR
T1 - Assessing the Safety and Efficacy of Spinal Anesthesia in Preterm and Term Neonates: A Multicenter Experience
AU - Adamu Yusuf Baffah
AU - Abubakar Muhammad Ballah
AU - Yahaya Halima Bidemi
AU - Jika Mohammed Mohammed
AU - Gyadale Abdulhamid Njidda
AU - Nwokorie Rosemary Mabong
AU - Galadima Hajara Aminu
AU - Hassan Maina Ali
AU - Ibrahim Naziru Joda
AU - Abdullahi Muhammad Maryam
AU - Adam Ibrahim Abdullahi
AU - Andibanbang Franklin
Y1 - 2024/06/14
PY - 2024
N1 - https://doi.org/10.11648/j.ijacm.20241201.19
DO - 10.11648/j.ijacm.20241201.19
T2 - International Journal of Anesthesia and Clinical Medicine
JF - International Journal of Anesthesia and Clinical Medicine
JO - International Journal of Anesthesia and Clinical Medicine
SP - 47
EP - 52
PB - Science Publishing Group
SN - 2997-2698
UR - https://doi.org/10.11648/j.ijacm.20241201.19
AB - Background: Worldwide, the incidence of premature birth is increasing with its attending congenital anomalies, so complex surgical interventions to manage these congenital anomalies or complications are usually performed at early days of life. Neonates are vulnerable to apnea, and congenital cardiopulmonary problems and they have higher morbidity and mortality compared to older children and adults etc. In the preterm neonate, the risk of bronchopulmonary dysplasia and apnoea make their management complex and this is further compounded by their smaller size. Objective of study: The aim of the study was to determine the safety and efficacy of spinal anesthesia among neonates. Methodology: The study is a prospective study conducted in three tertiary health Institutions in northeast Nigeria. It includes all neonates scheduled for surgery amenable under SA. Sociodemographic variables, Haemodynamic variables, duration of surgery, and complications observed were all recorded. Results: Spinal anaesthesia SA was done in 230 patients, 90% of the patients were term, and only 10% were preterm. The majority were male with a mean weight of 3002 ± 660 grams and a mean age of 14.51±7.28 days. SA was successful in 93% of the patients in the first attempt. Heart rate, mean arterial pressure and oxygen saturation remained stable all through the duration of surgery. About 6% of the patients were converted to General Anaesthesia GA on account of prolonged surgery. The highest level of sympathetic block was recorded at the level of T4 while the lowest was at T6. Herniotomy was the most common surgery performed. The surgery lasted an average of 72 ± 28 minutes. No complication was recorded. Conclusion: Spinal anaesthesia provides a safe and reliable option for neonates who may require surgery early in life to improve their chances of survival. It serves as an alternative to GA with enhanced haemodynamic stability in this fragile population.
VL - 12
IS - 1
ER -
Baffah, A. Y., Ballah, A. M., Bidemi, Y. H., Mohammed, J. M., Njidda, G. A., et al. (2024). Assessing the Safety and Efficacy of Spinal Anesthesia in Preterm and Term Neonates: A Multicenter Experience. International Journal of Anesthesia and Clinical Medicine, 12(1), 47-52. https://doi.org/10.11648/j.ijacm.20241201.19
Baffah, A. Y.; Ballah, A. M.; Bidemi, Y. H.; Mohammed, J. M.; Njidda, G. A., et al. Assessing the Safety and Efficacy of Spinal Anesthesia in Preterm and Term Neonates: A Multicenter Experience. Int. J. Anesth. Clin. Med.2024, 12(1), 47-52. doi: 10.11648/j.ijacm.20241201.19
Baffah AY, Ballah AM, Bidemi YH, Mohammed JM, Njidda GA, et al. Assessing the Safety and Efficacy of Spinal Anesthesia in Preterm and Term Neonates: A Multicenter Experience. Int J Anesth Clin Med. 2024;12(1):47-52. doi: 10.11648/j.ijacm.20241201.19
@article{10.11648/j.ijacm.20241201.19,
author = {Adamu Yusuf Baffah and Abubakar Muhammad Ballah and Yahaya Halima Bidemi and Jika Mohammed Mohammed and Gyadale Abdulhamid Njidda and Nwokorie Rosemary Mabong and Galadima Hajara Aminu and Hassan Maina Ali and Ibrahim Naziru Joda and Abdullahi Muhammad Maryam and Adam Ibrahim Abdullahi and Andibanbang Franklin},
title = {Assessing the Safety and Efficacy of Spinal Anesthesia in Preterm and Term Neonates: A Multicenter Experience
},
journal = {International Journal of Anesthesia and Clinical Medicine},
volume = {12},
number = {1},
pages = {47-52},
doi = {10.11648/j.ijacm.20241201.19},
url = {https://doi.org/10.11648/j.ijacm.20241201.19},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ijacm.20241201.19},
abstract = {Background: Worldwide, the incidence of premature birth is increasing with its attending congenital anomalies, so complex surgical interventions to manage these congenital anomalies or complications are usually performed at early days of life. Neonates are vulnerable to apnea, and congenital cardiopulmonary problems and they have higher morbidity and mortality compared to older children and adults etc. In the preterm neonate, the risk of bronchopulmonary dysplasia and apnoea make their management complex and this is further compounded by their smaller size. Objective of study: The aim of the study was to determine the safety and efficacy of spinal anesthesia among neonates. Methodology: The study is a prospective study conducted in three tertiary health Institutions in northeast Nigeria. It includes all neonates scheduled for surgery amenable under SA. Sociodemographic variables, Haemodynamic variables, duration of surgery, and complications observed were all recorded. Results: Spinal anaesthesia SA was done in 230 patients, 90% of the patients were term, and only 10% were preterm. The majority were male with a mean weight of 3002 ± 660 grams and a mean age of 14.51±7.28 days. SA was successful in 93% of the patients in the first attempt. Heart rate, mean arterial pressure and oxygen saturation remained stable all through the duration of surgery. About 6% of the patients were converted to General Anaesthesia GA on account of prolonged surgery. The highest level of sympathetic block was recorded at the level of T4 while the lowest was at T6. Herniotomy was the most common surgery performed. The surgery lasted an average of 72 ± 28 minutes. No complication was recorded. Conclusion: Spinal anaesthesia provides a safe and reliable option for neonates who may require surgery early in life to improve their chances of survival. It serves as an alternative to GA with enhanced haemodynamic stability in this fragile population.
},
year = {2024}
}
TY - JOUR
T1 - Assessing the Safety and Efficacy of Spinal Anesthesia in Preterm and Term Neonates: A Multicenter Experience
AU - Adamu Yusuf Baffah
AU - Abubakar Muhammad Ballah
AU - Yahaya Halima Bidemi
AU - Jika Mohammed Mohammed
AU - Gyadale Abdulhamid Njidda
AU - Nwokorie Rosemary Mabong
AU - Galadima Hajara Aminu
AU - Hassan Maina Ali
AU - Ibrahim Naziru Joda
AU - Abdullahi Muhammad Maryam
AU - Adam Ibrahim Abdullahi
AU - Andibanbang Franklin
Y1 - 2024/06/14
PY - 2024
N1 - https://doi.org/10.11648/j.ijacm.20241201.19
DO - 10.11648/j.ijacm.20241201.19
T2 - International Journal of Anesthesia and Clinical Medicine
JF - International Journal of Anesthesia and Clinical Medicine
JO - International Journal of Anesthesia and Clinical Medicine
SP - 47
EP - 52
PB - Science Publishing Group
SN - 2997-2698
UR - https://doi.org/10.11648/j.ijacm.20241201.19
AB - Background: Worldwide, the incidence of premature birth is increasing with its attending congenital anomalies, so complex surgical interventions to manage these congenital anomalies or complications are usually performed at early days of life. Neonates are vulnerable to apnea, and congenital cardiopulmonary problems and they have higher morbidity and mortality compared to older children and adults etc. In the preterm neonate, the risk of bronchopulmonary dysplasia and apnoea make their management complex and this is further compounded by their smaller size. Objective of study: The aim of the study was to determine the safety and efficacy of spinal anesthesia among neonates. Methodology: The study is a prospective study conducted in three tertiary health Institutions in northeast Nigeria. It includes all neonates scheduled for surgery amenable under SA. Sociodemographic variables, Haemodynamic variables, duration of surgery, and complications observed were all recorded. Results: Spinal anaesthesia SA was done in 230 patients, 90% of the patients were term, and only 10% were preterm. The majority were male with a mean weight of 3002 ± 660 grams and a mean age of 14.51±7.28 days. SA was successful in 93% of the patients in the first attempt. Heart rate, mean arterial pressure and oxygen saturation remained stable all through the duration of surgery. About 6% of the patients were converted to General Anaesthesia GA on account of prolonged surgery. The highest level of sympathetic block was recorded at the level of T4 while the lowest was at T6. Herniotomy was the most common surgery performed. The surgery lasted an average of 72 ± 28 minutes. No complication was recorded. Conclusion: Spinal anaesthesia provides a safe and reliable option for neonates who may require surgery early in life to improve their chances of survival. It serves as an alternative to GA with enhanced haemodynamic stability in this fragile population.
VL - 12
IS - 1
ER -