Abstract
Health is a primary need for human wellbeing. An advance technology, the health sector has changed significantly on that day. However, the issue of women’s health is still a cause of concern for developing countries like India. Particularly, socio-economic backwards and the low position accorded to women by society have always kept the issue of women’s health as a secondary manner. To transform this perspective and provide noticeable medical facilities to give women for ensure their wellness. The present study is an attempt to look into the role of Community Health Worker (ASHA) which is very important in West Bengal. Accredited Social Health Activist (ASHA) is a grassroot level female health worker who selected from village for improving of women’s health awareness and providing basic medical services, such as encouraging women to give birth in govt. Hospital, taking kids to vaccination clinics, promoting family planning, administering first assistance for minor wounds and illnesses, maintaining demographic records, and enhancing community cleanliness. Women in West Bengal are dealing with a number of issues, including breast cancer, AIDS, and maternal health issues in addition to starvation. ASHA employees are crucial to the health protection of women, particularly in rural West Bengali villages. Therefore, research into their significance in preserving women's health is necessary. Using Galsi Gram Panchayat, East Bardhaman district, West Bengal, as a case study, an attempt has been made to examine the role that ASHA workers play in raising awareness and protecting women's health, as well as their successes and shortcomings.
|
Published in
|
European Journal of Preventive Medicine (Volume 13, Issue 4)
|
|
DOI
|
10.11648/j.ejpm.20251304.12
|
|
Page(s)
|
79-86 |
|
Creative Commons
|

This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited.
|
|
Copyright
|
Copyright © The Author(s), 2025. Published by Science Publishing Group
|
Keywords
Community Health Worker, ASHA, Women’s Health Awareness, Grassroot Level, Family Planning, AIDS
1. Introduction
The most crucial factor in human survival is health. It refers to the condition of not being ill or injured. A state of well-being in which a person can seek personal development is often referred to as health. The World Health Organization (WHO) states that health is a condition of whole physical, mental, and social well-being rather than only the absence of illness or disability. (Constitution of the world Health Organization 2006)
| [1] | Arvey, Sarah R., and Maria E. Fernandez, 2012: Identifying the Core Elements of Effective Community Health Worker Programs: A Research Agenda. American Journal of Public Health 102(9): 1633-1637. |
[1]
.
Men's and women's health are interconnected in the concept of human health. However, it is evident that women's health issues are given less attention in our nation, which has historically discriminated against women due to its patriarchal social structure. Due to the widespread preference for male children in many regions of the nation, girls are sometimes viewed as burdens, and as a result, women's health and wellness issues rarely receive the necessary attention that they otherwise should. This focus on women and issues pertaining to their health has a direct effect on society and the overall development of the state in addition to women.
| [10] | Bhatia, K. 2014: Community Health Worker Programs in India: A rights-based review. Perspectives in Public Health, 134(5), 276-282. |
[10]
.
The Indian constitution’s Articles 39 (e) (f) 42 and 47 clearly mentioned that state responsibility to ensure a health life for the people of our country to secure equal rights to health for all. It also claims that it is the state’s responsibility to improve public health and raise the level of nutrition and living standard. At present public health is primarily the responsibility of the state Governments. Both the central and state government are given top priority on health
| [11] | Bhatia, K, 2014: Performance-based incentives of the ASHA scheme: stakeholder’s perspectives. Economic and Political Weekly, 49(22), 145-151. |
[11]
. The central government has introduced a various of community base health care services with special focus on women’s health to decrease gender discrimination and provide women with proper access to health care. In this paper, I focus on role of community health worker (ASHA) for protection women’s health, with prime concentration on the ASHA programme was introduced in India 2005 as part of the National Rural Health Mission (NRHM). The idea behind the Accredited Social Health Activists (ASHA) was connected marginalized community to the health care system Galsi Gram Panchayat in East Bardhaman, West Bengal
.
2. Origin and Meaning of ASHA
The Indian Government established the rural health scheme in 1977 in response to the Shrivastav committee’s recommendation with the intention of “putting people’s health in people’s hands (1975)’’
| [12] | Datta, Pankuri., 2021: ‘Rural Healthcare in India’, Kurukshetra, A Journal on Rural Development, January. |
[12]
. The sub-centre, primary health centre (PHC), and community health centre (CHC) make the three-tier structure of primary health care infrastructure in rural areas of India. This time Alma Ata International Health Conference in 1978, the World Health Organization set the world -wide societal objective of “Health for All by 2000 AD”
.
Health care delivery and access have historically presented substantial difficulties in India’s diversified and highly populated environment. Among the many initiatives to address this pressing issue, the introduction of Accredited Social Health Activist (ASHA) in 2005, as a part of NRHM, marked a significant step towards improving grassroots health care delivery, particularly among women and children, and reducing geographical and socio-economic disparities
| [13] | Editors PIM., 2011: Health care systems and conflict: a state of affairs. PLoS Med, 8: 7. |
[13]
.
Accredited Social Health Activist (ASHA) is a grassroot level health worker who is selected from a village to sever that village. The success of several programmes under the NRHM lies on the shoulders of ASHA network. The ASHA works as a liaison between the local rural community and the public health system. They are educated, young members of the rural community who undergo rigorous and continuous training and development to serve the rural community better. They share information on basic health and hygiene practices, counsel women on child birth and related issues and act as the first point of repository of basic health kits. The ministry health and family welfare, Government of India describes an ASHA as: “…Health activists in community who will create awareness on health and its social determinants and mobilize the community towards local health planning and increased utilization and accountability of the existing health services.”
.
2.1. Key Components of ASHA
1) ASHA must primarily be a women resident of the village married/ widowed/divorced, preferably in the age group of 25 to 45 years. She should be a literate woman with due preference in selection to those who are qualified up to 10
th standard wherever they are interested and available in good numbers. This may be relaxed only if no suitable person with this qualification is available
| [3] | B-Lajoie, M-R, J. Hulme, and K. Johnson, 2014: Payday, ponchos, and promotions: a qualitative analysis of perspectives from non-governmental organization programme managers on community health worker motivation and incentives. Hum Resour Health 12: 66. |
[3]
.
2) ASHA is chosen through a rigorous process of selection involving various community group, Self-Help Group, Anganwadi institutions, the Block Nodal Officer, District Nodal Officer, the village health committee, and the Grame Sabha.
3) ASHA must undergo service of training to acquire the necessary knowledge, skills, and confidence for performing her spelled out roles
| [14] | Government of India Planning Commission., 2013: Poverty estimates for 2011-12. |
[14]
.
4) The ASHAs receives performance-based incentives for promoting universal immunization, referral, and escort services for Reproductive & child health (RCH) and others health care programmes, and construction of household toilets.
5) ASHA provides information to the community on determinants of health such as nutrition, basic sanitation & hygienic practices, healthy living and working conditions, information on existing health services and the need for timely utilization of health and family welfare services
| [5] | Bhattacharyya, Karabi, et al., 2001: Community health worker incentives and disincentives: How they affect motivation, retention, and sustainability. USAID. |
[5]
.
6) She counsels women on birth preparedness, importance of safe delivery, breast-feeding and complementary feeding, immunization, contraception, and prevention of common infections including Reproductive Tract Infection/sexually Transmitted Infections (RTI/STIs) and care of the young child
| [6] | Bhutta, Zulfiqar A., et al., 2010: Global Experience of Community Health Workers for Delivery of Health Related Millennium Development Goals. World Health Organization and the Global Health Workforce Alliance. |
[6]
.
At the village level it is recognized that ASHA cannot function without adequate institutional support. Women’s committees (like SHGs, or women’s health committees), village health and sanitation committee of the Gram panchayat, peripheral health workers especially ANMs and Anganwadi workers, and trainers of ASHA and in-service periodic training are the major sources of support to ASHA
| [15] | Goswami, S. 2020: “The cost of mental health: A socio-psycho analysis” published in IASSI Quarterly, Contributions to Indian Social Science, Vol 39, No. 1, (January-March, 2020) PP 33-41. |
[15]
. The programme is totally incentive based where in women who volunteer from local community are selected and trained to reinforce community action for universal immunization, safe delivery, newborn care, prevention of communicable and non-communicable disease, improved nutrition, are of the senior citizens and promotion of household/community toilet. ASHAs are in place, in all states of India except in Goa, Paduchery, Himachal Pradesh the non-tribal of Tamil Nadu and the union territory of Chandigarh
| [4] | Basilico, Matthew, et al., 2013: Health for all? Competing theories and geopolitics. In Reimagining Global Health: An Introduction. P. Farmer, J. Y. Kim, A. Kleinman, and M. Basilico, eds. Pp. 74-110. Berkeley: UC Press. |
[4]
.
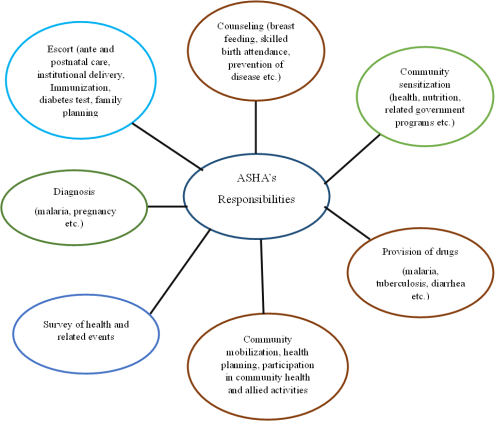
2.2. Key Responsibilities of ASHA
1) Identifying and recording new pregnancies, births and deaths.
2) Getting the community to demand and obtain health care through mobilizing, counselling, and supporting them.
3) Recognizing, managing, or referring sickness cases.
4) Assisting with the delivery of health service, through home visits, Frist-aid, and Immunization Programmes.
5) Keeping track of statistics and taking part in community health planning.
6) Participating in the Health and Nutrition Day in the village.
7) Encouraging women to have their babies in hospital.
8) Improving village cleanliness and encouraging family planning (e.g. surgical sterilization).
KEY RESPONSIBILITY OF ASHA
Figure 1. Diagram of various responsibilities.
3. The Area of Study: Galsi Gram Panchayat Under Galsi II CD Block
Galsi Gram Panchayat is located on the western side of Bardhaman city, district of East Bardhaman, West Bengal. It falls under the Galsi II CD Block. The Galsi Gram Panchayat has 19 booths under its administrative jurisdiction, covering an area of 700 hectares of land. According 2011 census, the total population under the panchayat is 19000
| [16] | Goswami, S. 2020, 2013: Persistent Inequalities: Gender Discrimination in Interior Rural India published in American International Journal of Research in Humanities, Arts and Social Sciences, 4(1), PP- 95-101. |
[16]
. Ther are four villages in Galsi Gram Panchayat namely Budbud, Chaktentul, Loapurkrishnarampur, and Galsi. This panchayat has mixed population comprising of Hindu, Muslim, and Adivasi. It falls under Block Primary Health Centre now its name is Loapurkrishnarampur Rural Hospital. Population of this panchayat is comparatively backward in relation to others. Hence, there are maximum population dependent on government health facilities
| [6] | Bhutta, Zulfiqar A., et al., 2010: Global Experience of Community Health Workers for Delivery of Health Related Millennium Development Goals. World Health Organization and the Global Health Workforce Alliance. |
[6]
.
4. Objectives of the Study
1. To investigate the benefits received by the women through ASHA workers.
2. To know the level of awareness among the women population of Galsi Gram Panchayat regarding the various functions of ASHA.
3. To study the satisfaction level of the women in getting required services through ASHA workers.
4. To know the problems faced by ASHA workers for implementation of their given duties.
5. Work Profile of ASHA in Selective Area
The ASHA worker in Galsi Gram Panchayat undertake the following activities:
1) Hole monthly awareness programme regarding women and child health which individual generating awareness, family planning, provision of adequate nutrition to children as per their age, care to be taken by women and her family during pregnancy etc.
| [17] | Jain, Devaki, 2006: “Women, Development, and the UN: A Sixty years Quest for equality and justice”, Orient Longman, India. |
[17]
.
2) Providing information to the newly married couple about the importance of adopting sexual practices to prevent the occurrence and spread of sexually transmitted diseases.
3) To promote women’s wellness, sanitation and hygiene, ASHA workers distribute sanitary napkin to the womenfolk and provide information regarding their usage and proper disposal
| [7] | Biehl, João, 2010: When people come first: Beyond technical and theoretical quick-fixes in global health. In Global Political Ecology. R. Peet, P. Robbins, and M. Watts, eds. Pp. 100-130. London: Routledge. |
[7]
.
4) They conduct home visit for promotion of health and preventive care wherein they gather information regarding the presence of pregnant women and girl child and provide them with necessary iron, folic acid, calcium tablets etc.
5) ASHAs also provide awareness regarding of safe child delivery practices and accompany the pregnant women to the government hospital for periodic health cheek up
| [21] | World Health Organization (WHO), 1978: Alma Ata Declaration, Geneva: World Health Organization. |
[21]
.
6) They ensure the proper conduct of immunization programmes to the newly born and infants.
6. Methodology
The study on the role of Community Health Worker (ASHA) for protection of women health in Galsi Gram Panchayat is both analytical and descriptive. The data used in this regard both primary and secondary. Primary data was collected through purposive random sampling method
| [18] | Jena, Vandana Kumar 1989: “Women and Development”, Indian Journal of Public Administration, October-December. |
[18]
. Number of twenty (20) ASHA workers engaged in the panchayat area, five (5) ASHA workers were directly interviewed through open ended questionnaire and the respondent of total 30 women beneficiaries under the supervision of the selected ASHA workers (one ASHA worker under 6 women beneficiaries) were collected through a questionnaire
| [8] | Biehl, João, and Adriana Petryna, 2013: Critical Global Health. In When People Come First: Critical Studies in Global Health. J. Biehl and A. Petryna, eds. Pp. 1-20. Princeton: Princeton University Press. |
[8]
.
7. Results and Discussions
It is already discussed that in this study 35 sample respondents are selected from Galsi Gram Panchayat. Their responses were collected and tabulated with the help of statistical tables. For analysis and interpreting data and obtaining meaningful conclusion, appropriate statistical measures are produced using various statistical methods.
Table 1. Classification of respondents.
Respondents | No. of respondents |
ASHA workers | 05 |
Beneficiaries (women) | 30 |
Source: primary Survey: 20204
From above table five (05) of respondents belongs to ASHA and remaining thirty (30) of the respondents belongs to beneficiaries’ group. The beneficiaries are more in numbers which is a clear indication of participation of women in various activities.
Table 2. Classification of women respondents (beneficiaries).
Division of female beneficiaries | No. of respondent | Percentage |
Unmarried | 13 | 43.3 |
Married | 17 | 56.6 |
Source: primary Survey: 2024
From the above table based on marital status, women (beneficiary) respondents are divided into two categories i.e. unmarried and married. Majority respondents are married (56.6) and rest of respondents are unmarried (43.3) selected for the study. The married woman has greater access to the scheme of Government. The need of running family expenses is also higher than unmarried.
Table 3. Education qualifications of ASHA workers.
Qualification | No of respondent | Percentage |
Below Secondary | 00 | 00 |
Secondary | 00 | 00 |
Higher Secondary | 02 | 40 |
Graduated | 03 | 60 |
Source: primary Survey: 2024
Form the above table, 40%of ASHA workers have passed the Higher Secondary and 60% of ASHA workers have passed graduate examination. ASHA workers have higher educated.
Table 4. Economic categories of ASHA workers.
Category | No. of respondents | Percentage |
APL | 05 | 100 |
BPL | 00 | 00 |
Source: primary Survey: 2024
From above table, all respondents are belonging APL category. They have stander of living approximately high from BPL category. The participants are mostly APL because they have the grater chances of political support.
Table 5. Problems regarding transportation.
Response | No. of respondents | Percentage |
Yes | 03 | 60 |
No | 02 | 40 |
Total | 05 | 100 |
Source: primary Survey: 2024
The above table shows the response of ASHA workers regarding transportation problem due to beneficiaries live at remote village. Three respondents opined that they have problem regarding transportation. It means 60% of ASHA workers facing problem. Only 40% do not have any problem for transportation.
Table 6. Satisfaction level on salary.
Response | No. of respondent | Percentage |
Highly satisfied | 00 | 00 |
Satisfied | 01 | 20 |
Not satisfied | 04 | 80 |
Source: primary Survey: 2024
The above table shows that 80% of ASHA employees are dissatisfied their remuneration for their work. Only 20% of respondents said she was satisfied her remuneration or salary.
Table 7. Home visit of ASHA worker.
Response | No. of respondents | Percentage |
Yes | 30 | 100 |
No | 00 | 00 |
Source: primary Survey: 2024
From the above table, 100% of the respondents’ houses are visited by ASHA workers and they are working very sincerely in the field. The result shows that the workers periodically visit the field which is very good practice.
Table 8. Frequency of visit of ASHA workers.
Frequency | No. of respondents | Percentage |
Once | 00 | 00 |
Twice | 06 | 20 |
Thrice | 05 | 16.6 |
More than that | 19 | 63.3 |
Total | 30 | 100 |
Source: primary Survey: 2024
The table shows the frequency of visit of ASHA workers among the houses. ASHA workers visited more time for beneficiaries’ home when they fell need and any kind of problem. It is shows that 0% of respondent’s house is visited only once, 20% of the respondents’ houses are visited twice, 16.6% of respondents’ houses were visited thrice, and 63.3% of the respondents’ opinion that ASHA workers visited more than that in month.
Table 9. Information provided by ASHA regarding health issues.
Information | No. of respondents | percentage |
Yes | 30 | 100 |
No | 00 | 00 |
Total | 30 | 100 |
Source: primary Survey: 2024
The above table shows that the provision of health-related information by ASHA workers. All respondents’ (100%) are received health-related information from ASHA workers.
Table 10. Opinion about ASHA workers.
Sl. no | Factors | Very good | Good | neutral | Bad |
01 | Minor health injuries/ first aid | 09 | 21 | 00 | 00 |
02 | Nutrition | 26 | 04 | 00 | 00 |
03 | Sanitation | 03 | 23 | 04 | 00 |
04 | Delivery | 24 | 06 | 00 | 00 |
05 | Immunization schedule of new born babies | 28 | 02 | 00 | 00 |
06 | Prevention from sexually transmitted disease | 02 | 28 | 00 | 00 |
Source: primary Survey: 2024
As can be seen from the table, ASHA’s performance on most of the tasks is deemed satisfactory. The vaccination schedule for new born babies is rated as very good by 28 out of 30 respondents, while the delivery performance of ASHA workers is rated as very good by 24 respondents, and sanitation-related activities of ASHA are rated as good by 23 respondents. In terms of nutrition, the most preferred service provided by ASHA workers. It is rated as very good by 26 respondents, while 21 respondents rated minor health tasks of ASHA workers as good, and 28 respondents rated sexual transmitted disease-related ASHA work as good. Here, all beneficiaries are aware their health problems and discuss regrading problem through ASHA workers. It is clear that rural women are protected by the ASHA workers
| [9] | Cueto, Marcos, 2004: The origins of primary health care and selective primary health care. American Journal of Public Health 94(11): 1864-1874. |
[9]
.
Table 11. Services rendered by ASHA workers.
Services | No. of respondents | Percentage |
Minor health injuries/ first aid | 10 | 10.87 |
Nutrition | 20 | 21.74 |
Sanitation | 07 | 7.61 |
Delivery | 22 | 23.91 |
Immunization schedule of new born babies | 28 | 30.43 |
Prevention from sexually transmitted disease | 05 | 5.43 |
Total | 92 | 100 |
Source: primary Survey: 2024
The services provided by ASHA workers to the community are listed in
Table 7 out of 30 respondents, 30.43% received delivery services, 23.91% received immunization schedules for new born babies, and 21.74% received nutrition services. 10.87% received information about minor health injuries, 7.61% received sanitation services, and 5.43% received information about sexually transmitted disease prevention.
Table 12. Satisfaction levels of beneficiaries.
Level | No. of respondent | Percentage |
Highly satisfied | 20 | 66.67 |
Satisfied | 07 | 23.33 |
Neutral | 02 | 6.67 |
Dissatisfied | 01 | 3.33 |
Total | 30 | 100 |
Source: primary Survey: 2024
This table offers information about respondents’ levels of satisfaction with ASHA workers’ performance. 66.67% of respondents are highly satisfied with ASHA workers, 23.33%of respondents are satisfied, 6.67% of respondents are neutral, 3.33% of respondents are dissatisfied for ASHA’s duties. Here, rural beneficiaries are always taken service for health-related issues from ASHA workers.
8. Major Findings
1) The purpose of retain monthly community meetings by the ASHA workers gets partially fulfilled because of low attendance of women and girl child.
2) The ASHA workers cannot ensure timely distribution of personal hygiene materials like sanitary napkins because they do not receive them from the Government regularly.
3) The ASHA can only distribute medicines to the women until stocks last. They do not have stock backups to meet additional requirements as well as in emergencies.
4) Hesitation on the part of women and girls to freely discus women related health issues with the workers.
5) Lack of realization on the part of women regarding observance of personal hygiene and proper sanitary waste disposal mechanism.
6) As the ASHA received the governmental incentive which does not ensure them for descent standard of living.
9. Suggestions
1) ASHA works on a population size of 1000. The population size should be reduced so that ASHA can adequately serve a small population.
2) Awareness programmes and campaigns must include the use of more visible to attract the attention of the audience.
3) The number of ASHA training programmes should be expanded.
4) ASHAs compensation must be increased for more people to volunteer to help uplift rural community.
5) More medical camps and seminars should be held by ASHA to raise public awareness.
10. Conclusion
Accredited Social Health Activists are the backbone of community healthcare in rural India. By reimaging their role, strengthening their capacities, and embracing technology, India can significantly improve healthcare access and outcomes for its underserved populations
| [20] | Pandey SK, Upadhyay R. 2020: Institutionalizing Health though NRHM: A study of Village Health Committees in Uttar Pradesh. MPJSS: 26. |
[20]
. To keep pace with the evolving healthcare landscape, their role must be rediscovered and enhanced
| [19] | Joshi S, Mathews G., 2012: Healthcare through community participation: role of ASHAs. EPW. 47(10): 70. |
[19]
. ASHA has been successful with its actives like immunization schedules for new born babies, sanitation, and various healthcare programmes. By transforming ASHA workers into informed health educators, digital health programmes, and integral components of the healthcare coverage and improved health outcomes for all citizen. A comprehensive approach that integrates ASHA workers into the broader healthcare system will pave the way for a healthier and more equitable nation
| [8] | Biehl, João, and Adriana Petryna, 2013: Critical Global Health. In When People Come First: Critical Studies in Global Health. J. Biehl and A. Petryna, eds. Pp. 1-20. Princeton: Princeton University Press. |
[8]
. The scope of future studies will definitely emerge from the present study. This research is an initiative to revisit the condition of primary health sector in West Bengal.
Abbreviations
AIDS | Acquired Immunodeficiency Syndrome |
ASHA | Accredited Social Health Activist |
NRHM | National Rural Health Mission |
PHC | Primary Health Centre |
CHC | Community Health Centre |
WHO | World Health Organization |
RTI | Reproductive Tract Infection |
STI | Sexually Transmitted Infections |
Author Contributions
Sribas Goswami is the sole author. The author read and approved the final manuscript.
Conflicts of Interest
The author declares no conflicts of Interest.
References
| [1] |
Arvey, Sarah R., and Maria E. Fernandez, 2012: Identifying the Core Elements of Effective Community Health Worker Programs: A Research Agenda. American Journal of Public Health 102(9): 1633-1637.
|
| [2] |
Ashraf, Nava, Oriana Bandiera, and B. Kelsey Jack, 2014: No margin, no mission? A field experiment on incentives for public service delivery. Journal of Public Economics.
http://dx.doi.org/10.1016/j.jpubeco.2014.06.014
|
| [3] |
B-Lajoie, M-R, J. Hulme, and K. Johnson, 2014: Payday, ponchos, and promotions: a qualitative analysis of perspectives from non-governmental organization programme managers on community health worker motivation and incentives. Hum Resour Health 12: 66.
|
| [4] |
Basilico, Matthew, et al., 2013: Health for all? Competing theories and geopolitics. In Reimagining Global Health: An Introduction. P. Farmer, J. Y. Kim, A. Kleinman, and M. Basilico, eds. Pp. 74-110. Berkeley: UC Press.
|
| [5] |
Bhattacharyya, Karabi, et al., 2001: Community health worker incentives and disincentives: How they affect motivation, retention, and sustainability. USAID.
|
| [6] |
Bhutta, Zulfiqar A., et al., 2010: Global Experience of Community Health Workers for Delivery of Health Related Millennium Development Goals. World Health Organization and the Global Health Workforce Alliance.
|
| [7] |
Biehl, João, 2010: When people come first: Beyond technical and theoretical quick-fixes in global health. In Global Political Ecology. R. Peet, P. Robbins, and M. Watts, eds. Pp. 100-130. London: Routledge.
|
| [8] |
Biehl, João, and Adriana Petryna, 2013: Critical Global Health. In When People Come First: Critical Studies in Global Health. J. Biehl and A. Petryna, eds. Pp. 1-20. Princeton: Princeton University Press.
|
| [9] |
Cueto, Marcos, 2004: The origins of primary health care and selective primary health care. American Journal of Public Health 94(11): 1864-1874.
|
| [10] |
Bhatia, K. 2014: Community Health Worker Programs in India: A rights-based review. Perspectives in Public Health, 134(5), 276-282.
|
| [11] |
Bhatia, K, 2014: Performance-based incentives of the ASHA scheme: stakeholder’s perspectives. Economic and Political Weekly, 49(22), 145-151.
|
| [12] |
Datta, Pankuri., 2021: ‘Rural Healthcare in India’, Kurukshetra, A Journal on Rural Development, January.
|
| [13] |
Editors PIM., 2011: Health care systems and conflict: a state of affairs. PLoS Med, 8: 7.
|
| [14] |
Government of India Planning Commission., 2013: Poverty estimates for 2011-12.
|
| [15] |
Goswami, S. 2020: “The cost of mental health: A socio-psycho analysis” published in IASSI Quarterly, Contributions to Indian Social Science, Vol 39, No. 1, (January-March, 2020) PP 33-41.
|
| [16] |
Goswami, S. 2020, 2013: Persistent Inequalities: Gender Discrimination in Interior Rural India published in American International Journal of Research in Humanities, Arts and Social Sciences, 4(1), PP- 95-101.
|
| [17] |
Jain, Devaki, 2006: “Women, Development, and the UN: A Sixty years Quest for equality and justice”, Orient Longman, India.
|
| [18] |
Jena, Vandana Kumar 1989: “Women and Development”, Indian Journal of Public Administration, October-December.
|
| [19] |
Joshi S, Mathews G., 2012: Healthcare through community participation: role of ASHAs. EPW. 47(10): 70.
|
| [20] |
Pandey SK, Upadhyay R. 2020: Institutionalizing Health though NRHM: A study of Village Health Committees in Uttar Pradesh. MPJSS: 26.
|
| [21] |
World Health Organization (WHO), 1978: Alma Ata Declaration, Geneva: World Health Organization.
|
Cite This Article
-
APA Style
Goswami, S. (2025). Lessons from Community Participation in Health Programmes: A Case of West Bengal. European Journal of Preventive Medicine, 13(4), 79-86. https://doi.org/10.11648/j.ejpm.20251304.12
 Copy
|
Copy
|
 Download
Download
ACS Style
Goswami, S. Lessons from Community Participation in Health Programmes: A Case of West Bengal. Eur. J. Prev. Med. 2025, 13(4), 79-86. doi: 10.11648/j.ejpm.20251304.12
Copy
|
Download
AMA Style
Goswami S. Lessons from Community Participation in Health Programmes: A Case of West Bengal. Eur J Prev Med. 2025;13(4):79-86. doi: 10.11648/j.ejpm.20251304.12
Copy
|
Download
-
@article{10.11648/j.ejpm.20251304.12,
author = {Sribas Goswami},
title = {Lessons from Community Participation in Health Programmes: A Case of West Bengal
},
journal = {European Journal of Preventive Medicine},
volume = {13},
number = {4},
pages = {79-86},
doi = {10.11648/j.ejpm.20251304.12},
url = {https://doi.org/10.11648/j.ejpm.20251304.12},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ejpm.20251304.12},
abstract = {Health is a primary need for human wellbeing. An advance technology, the health sector has changed significantly on that day. However, the issue of women’s health is still a cause of concern for developing countries like India. Particularly, socio-economic backwards and the low position accorded to women by society have always kept the issue of women’s health as a secondary manner. To transform this perspective and provide noticeable medical facilities to give women for ensure their wellness. The present study is an attempt to look into the role of Community Health Worker (ASHA) which is very important in West Bengal. Accredited Social Health Activist (ASHA) is a grassroot level female health worker who selected from village for improving of women’s health awareness and providing basic medical services, such as encouraging women to give birth in govt. Hospital, taking kids to vaccination clinics, promoting family planning, administering first assistance for minor wounds and illnesses, maintaining demographic records, and enhancing community cleanliness. Women in West Bengal are dealing with a number of issues, including breast cancer, AIDS, and maternal health issues in addition to starvation. ASHA employees are crucial to the health protection of women, particularly in rural West Bengali villages. Therefore, research into their significance in preserving women's health is necessary. Using Galsi Gram Panchayat, East Bardhaman district, West Bengal, as a case study, an attempt has been made to examine the role that ASHA workers play in raising awareness and protecting women's health, as well as their successes and shortcomings.
},
year = {2025}
}
Copy
|
Download
-
TY - JOUR
T1 - Lessons from Community Participation in Health Programmes: A Case of West Bengal
AU - Sribas Goswami
Y1 - 2025/09/09
PY - 2025
N1 - https://doi.org/10.11648/j.ejpm.20251304.12
DO - 10.11648/j.ejpm.20251304.12
T2 - European Journal of Preventive Medicine
JF - European Journal of Preventive Medicine
JO - European Journal of Preventive Medicine
SP - 79
EP - 86
PB - Science Publishing Group
SN - 2330-8230
UR - https://doi.org/10.11648/j.ejpm.20251304.12
AB - Health is a primary need for human wellbeing. An advance technology, the health sector has changed significantly on that day. However, the issue of women’s health is still a cause of concern for developing countries like India. Particularly, socio-economic backwards and the low position accorded to women by society have always kept the issue of women’s health as a secondary manner. To transform this perspective and provide noticeable medical facilities to give women for ensure their wellness. The present study is an attempt to look into the role of Community Health Worker (ASHA) which is very important in West Bengal. Accredited Social Health Activist (ASHA) is a grassroot level female health worker who selected from village for improving of women’s health awareness and providing basic medical services, such as encouraging women to give birth in govt. Hospital, taking kids to vaccination clinics, promoting family planning, administering first assistance for minor wounds and illnesses, maintaining demographic records, and enhancing community cleanliness. Women in West Bengal are dealing with a number of issues, including breast cancer, AIDS, and maternal health issues in addition to starvation. ASHA employees are crucial to the health protection of women, particularly in rural West Bengali villages. Therefore, research into their significance in preserving women's health is necessary. Using Galsi Gram Panchayat, East Bardhaman district, West Bengal, as a case study, an attempt has been made to examine the role that ASHA workers play in raising awareness and protecting women's health, as well as their successes and shortcomings.
VL - 13
IS - 4
ER -
Copy
|
Download