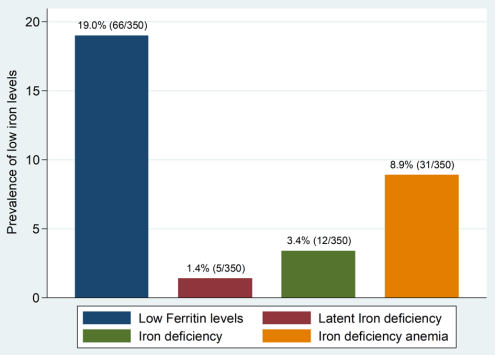
Background: It is estimated that, in Tanzania 11percent of babies are born prematurely each year. Preterm delivered infants are more prone to iron deficiency because most of mother to child iron transfer occurs in the third trimester. Methods: This was a hospital based cross sectional study, conducted in five selected health facilities in Mwanza city. Three hundred and fifty preterm delivered infants aged 6 to 30 weeks were included in the study. Participants’ information was obtained by using a pre-tested structured questionnaire. To determine body iron level, blood was collected to measure serum ferritin, full blood picture and C reactive protein. Results: In every 100 infants, 20 had low iron levels, 1 had latent iron deficiency, 3 had iron deficiency and 9 had iron deficiency anemia. Increase in infant’s age and complementary feeding with cow’s milk were significantly associated with iron deficiency anemia. In addition, hemoglobin level and mean corpuscular volume in combination is not a good alternative of serum ferritin in diagnosing low iron. Recommendations: Food fortification with iron and iron supplementation among preterm delivered infants are needed to prevent iron deficiency among these infants. Further studies to determine why older preterm delivered infants are more prone to iron deficiency anemia including type of food they eat are needed. Hemoglobin level and mean corpuscular volume can be used to rule out those without low iron but not to diagnose those with low iron level.
| Published in | European Journal of Preventive Medicine (Volume 12, Issue 5) |
| DOI | 10.11648/j.ejpm.20241205.11 |
| Page(s) | 111-120 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2024. Published by Science Publishing Group |
Iron Levels, Hemoglobin Levels, Infants, Preterm Birth
Variable | Number (n) | Percent (%) |
|---|---|---|
Health facility | ||
Makongoro Health Center | 66 | 18.9 |
Bugando Medical Center | 135 | 38.6 |
Buzuruga Health Center | 33 | 9.4 |
Nyamagana Hospital | 55 | 15.7 |
Sengerema District Hospital | 61 | 17.4 |
Age categories in weeks | ||
6 – 12 weeks | 192 | 54.9 |
13 – 23 weeks | 76 | 21.7 |
24 – 30 weeks | 82 | 23.4 |
Sex | ||
Male | 174 | 49.7 |
Female | 176 | 50.3 |
Care taker | ||
Mother | 348 | 99.4 |
Guardian | 2 | 0.6 |
Care taker’s age | ||
15 – 25 years | 170 | 48.6 |
26 – 35 years | 154 | 44.0 |
>35 years | 26 | 7.4 |
Care taker’s education level | ||
None | 18 | 5.1 |
Primary | 208 | 59.4 |
Secondary | 107 | 30.6 |
College/university | 17 | 4.9 |
Care taker’s employment status | ||
Employed | 254 | 72.6 |
Unemployed | 96 | 27.4 |
Variable | Number (n) | Percentage (%) |
|---|---|---|
Birth weight | ||
<1.5 Kg | 73.0 | 20.9 |
≥1.5 to 2.49 Kg | 277 | 79.1 |
Gestation status | ||
Single tone | 294 | 84.0 |
Twins | 53 | 15.1 |
Triplets | 3 | 0.9 |
Using iron supplements | ||
Yes | 16 | 4.6 |
No | 344 | 95.4 |
Received blood transfusion | ||
Yes | 28 | 8.0 |
No | 322 | 92.0 |
Nutritional status | ||
Normal | 209 | 59.7 |
Malnutrition | 98 | 28.0 |
Undetermined | 43 | 12.3 |
Palmar pallor | ||
Yes | 45 | 12.9 |
No | 305 | 87.1 |
Difficulty in breathing | ||
Yes | 1 | 0.3 |
No | 349 | 99.7 |
Presence of edema | ||
Yes | 0 | 0.0 |
No | 350 | 100.0 |
Hemoglobin level (g/dl) | ||
4.9 – 10.4 (low) | 210 | 60.0 |
10.5 – 14.0 (normal) | 120 | 34.3 |
14.1 – 19.5 (high) | 20 | 5.7 |
Serum Ferritin level (ug/l) | ||
0 – 11.9 (low) | 66 | 18.8 |
12 – 29.9 (normal) | 79 | 22.6 |
30 – 580 (high) | 205 | 58.6 |
Mean corpuscular volume (fl) | ||
38.4 – 71.9 (low) | 101 | 28.9 |
72 – 88 (normal) | 137 | 39.1 |
88.1 – 128 (high) | 112 | 32.0 |
CRP levels (mg/l) | ||
0 – 10 (normal) | 348 | 99.4 |
10.1 – 17 (high) | 2 | 0.6 |
Patient characteristics | Iron Deficiency Anemia | Univariate | Multivariate | |||
|---|---|---|---|---|---|---|
Yes | No | |||||
n (%) | n (%) | OR [95%CI] | p-value | OR [95%CI] | p-value | |
Age in weeks | ||||||
6 – 12 | 5 (2.6) | 187 (97.4) | 1.0 | |||
13 – 23 | 6 (7.9) | 70 (92.1) | 3.2 [0.9-10.8] | 0.061 | 3.2 [0.8-12.4] | 0.092 |
24 – 30 | 20 (24.3) | 62 (75.6) | 12 [4.3-33.5] | <0.001 | 8 [1.7-36.8] | 0.007 |
Nutritional status | ||||||
Normal | 19 (9.1) | 190 (90.9) | 1.0 | |||
Malnutrition | 11 (11.2) | 87 (88.8) | 1.3 [0.6-2.8] | 0.558 | 0.8 [0.3-2.0] | 0.565 |
Undetermined | 1 (2.3) | 42 (97.7) | 0.2 [0.0-1.8] | 0.168 | 0.8 [0.8-7.5] | 0.819 |
Age started complementary feeding | ||||||
Still on exclusive breast feeding | 10 (4.3) | 225 (95.7) | 1.0 | |||
Less than 12weeks | 2 (6.5) | 29 (93.5) | 1.6 [0.3-7.4] | 0.583 | 0.3 [0.0-2.1] | 0.224 |
From 12 -24weeks | 11 (27.5) | 29 (72.5) | 8.5 [3.3-21.8] | <0.001 | 1.2 [0.3-5.4] | 0.847 |
Above 24weeks | 8 (18.2) | 36 (81.8) | 5.0 [1.9-13.5] | 0.002 | 0.5 [0.1-2.6] | 0.380 |
Formula milk | ||||||
No | 29 (8.9) | 298 (91.1) | 1.0 | |||
Yes | 2 (8.7) | 21 (91.3) | 1.0 [0.2-4.4] | 0.978 | ||
Cow’s milk | ||||||
No | 20 (6.1) | 306 (93.9) | 1.0 | |||
Yes | 11 (47.8) | 12 (52.2) | 14.0 [5.5-35.7] | <0.001 | 8.8 [2.8-27.7] | < 0.001 |
Goat’s milk | ||||||
No | 30 (8.6) | 318 (91.4) | 1.0 | |||
Yes | 1 (50.0) | 1 (50.0) | 10.6 [0.6-173.8] | 0.098 | 5.8 [0.2-158.9] | 0.298 |
Porridge and other carbohydrate foods | ||||||
No | 12 (4.6) | 248 (95.4) | 1.0 | |||
Yes | 19 (21.1) | 71 (78.9) | 5.5 [2.6-11.9] | <0.001 | 2.6 [0.8-7.9] | 0.096 |
Ferritin deficiency | |||
|---|---|---|---|
Yes | No | Total | |
MCV-Hb together | n (%) | n (%) | n (%) |
Yes | 31 (47.0) | 45 (15.9) | 76 (21.7) |
No | 35 (53.0) | 239 (84.1) | 274 (78.3) |
Total | 66 (100) | 284 (100.0) | 350 (100.0) |
Health facility | Iron deficiency anemia | Total | P – value | |
|---|---|---|---|---|
Yes | No | |||
n (%) | n (%) | |||
Makongoro health center | 4 (6.06) | 62 (93.94) | 66 (100%) | 0.007 |
Bugando medical center | 22 (16.30) | 113 (83.70) | 135 (100%) | |
Buzuruga health center | 1 (3.03) | 32 (96.97) | 33 (100%) | |
Nyamagana district hospital | 2 (3.64) | 53 (96.36) | 55 (100%) | |
Sengerema district hospital | 2 (3.28) | 59 (96.72) | 61 (100%) | |
Health facility | Iron supplements | Total | P – value | |
|---|---|---|---|---|
Yes | No | |||
n (%) | n (%) | |||
Makongoro health center | 3 (4.55) | 63 (95.45) | 66 (100.00) | 0.733 |
Bugando medical center | 6 (4.44) | 129 (95.56) | 135 100.00) | |
Buzuruga health center | 0 (0.00) | 33 (100.00) | 33 (100.00) | |
Nyamagana district hospital | 3 (5.45) | 52 (94.55) | 55 (100.00) | |
Sengerema district hospital | 4 (6.56) | 57 (93.44) | 61 (100.00) | |
Clinical sign | Iron deficiency anemia | Totaln (%) | p- value | |
|---|---|---|---|---|
Yes | No | |||
n (%) | n (%) | |||
Palmar Palor | ||||
Yes | 13 (28.89) | 32 (71.11) | 45 (100%) | < 0.001 |
No | 18 (5.90) | 287 (94.10) | 305 (100%) | |
Difficulty in breathing | ||||
Yes | 0 (0.00) | 1 (100) | 1 (100) | 0.911 |
No | 31 (8.88) | 318 (91.12) | 349 (100) | |
Gallop rhythm | ||||
Yes | 2 (40.00) | 3 (60.00) | 5 (100.00) | 0.061 |
No | 28 (8.16) | 315 (91.84) | 343 (100.00) | |
BMC | Bugando Medical Centre |
CUHAS | Catholic University of Health and Allied Sciences |
MCV | Mean Corpuscular Volume |
Hb | Hemoglobin |
RBC | Red Blood Cell |
CRP | C-reactive Protein |
FBP | Full Blood Picture |
| [1] | Tanzania, RACH, The National Road Map Strategic Plan to Accelerate Reduction ofMaternal, Newborn and Child Deaths in Tanzania 2008 - 2015. Sanga C. et al, editor. Ministry of Health and Social Welfare, Tanzania. p. 6-7. |
| [2] | Blencowe H, Cousens S, Oestergaard MZ et al. National, regional, and worldwide estimatesof preterm birth rates in the year 2010 with time trends since 1990 for selected countries: asystematic analysis and implications. The Lancet. 2012; 379(9832): 2162-72. |
| [3] | Clardy S, Wang X, Zhao W et al. Acute and chronic effects of developmental irondeficiency on mRNA expression patterns in the brain. Oxidative Stress and Neuroprotection. 2006: 173-96. |
| [4] | deUngria M, Rao R, Wobken JD et al. Perinatal iron deficiency decreases cytochrome coxidase (CytOx) activity in selected regions of neonatal rat brain. Pediatric research.2000; 48(2): 169-76. |
| [5] | Kasasa A. Neurodevelopment of Low Birth Weight Born Infants in Relation to their IronStatus in Dar es salaam, Tanzania. 2011. |
| [6] | Lozoff B, Georgieff MK, editors. Iron deficiency and brain development. Seminars inpediatric neurology; 2006: Elsevier. |
| [7] | Tran PV, Fretham SJ, Carlson ES et al. Long-term reduction of hippocampal brain-derivedneurotrophic factor activity after fetal-neonatal iron deficiency in adult rats. Pediatricresearch. 2009; 65: 493-8. |
| [8] | Robert M. Kliegman et al. Nelson Textbook of Pediatrics, 20th ed. Philadephia, ElsevierInc. 2016. p 821-824. |
| [9] | Strauss RG. Anaemia of prematurity: pathophysiology and treatment. Blood reviews.2010; 24(6): 221-5. |
| [10] | Olivares M, Llaguno S, Marin V et al. Iron status in low-birth-weight infants, small andappropriate for gestational age. A follow-up study. ActaPaediatrica. 1992; 81(10): 824-8. |
| [11] | Chockalingam UM, Murphy E, Ophoven JC et al. Cord transferrin and ferritin values innewborn infants at risk for prenatal uteroplacental insufficiency and chronic hypoxia. TheJournal of pediatrics. 1987; 111(2): 283-6. |
| [12] |
AAP. Diagnosis and Prevention of Iron Deficiency and Iron-Deficiency Anemia in Infantsand Young Children (0 –3 Years of Age). Clinical Report. October, 2010
http://pediatrics.aappublications.org/content/pediatrics/early/2010/10/05/peds.20102576.full.pdf |
| [13] | Lundström U, Siimes MA, Dallman PR. At what age does iron supplementation becomenecessary in low-birth-weight infants? The Journal of pediatrics. 1977; 91(6): 878-83. |
| [14] | Puspitasari HA, Windiastuti E, Hendarto A. Iron profiles of preterm infants at two monthsof chronological age. PaediatricaIndonesiana. 2017; 56(5): 277-84. |
| [15] | World Health Organization. Serum ferritin concentrations for the assessment of iron statusand iron deficiency in populations. Vitamin and Mineral Nutrition Information SystemGeneva: 2011 (WHO/NMH/NHD/MNM/11.2). |
| [16] | Ferri C, Procianoy RS, Silveira RC. Prevalence and Risk Factors for Iron-Deficiency Anemia in Very-Low-Birth-Weight Preterm Infants at 1 Year of Corrected Age. Journal of Tropical Pediatrics. 2014; 60(1): 53-60. |
| [17] | Chandyo RK, Henjum S, Ulak M et al. The prevalence of anemia and iron deficiency ismore common in breastfed infants than their mothers in Bhaktapur, Nepal. European Journal of Clinical Nutrition. 2015; 70: 456. |
APA Style
Machangu, N. S., Kayange, N. M., Bakalemwa, R. C., Mabega, N. G., Kidenya, B. R. (2024). Iron levels and Associated Factors Among Preterm Delivered Infants in Five Selected Health Facilities in Mwanza Region, Northwestern Tanzania. European Journal of Preventive Medicine, 12(5), 111-120. https://doi.org/10.11648/j.ejpm.20241205.11
ACS Style
Machangu, N. S.; Kayange, N. M.; Bakalemwa, R. C.; Mabega, N. G.; Kidenya, B. R. Iron levels and Associated Factors Among Preterm Delivered Infants in Five Selected Health Facilities in Mwanza Region, Northwestern Tanzania. Eur. J. Prev. Med. 2024, 12(5), 111-120. doi: 10.11648/j.ejpm.20241205.11
AMA Style
Machangu NS, Kayange NM, Bakalemwa RC, Mabega NG, Kidenya BR. Iron levels and Associated Factors Among Preterm Delivered Infants in Five Selected Health Facilities in Mwanza Region, Northwestern Tanzania. Eur J Prev Med. 2024;12(5):111-120. doi: 10.11648/j.ejpm.20241205.11
@article{10.11648/j.ejpm.20241205.11,
author = {Nakiete Samwel Machangu and Neema Mathias Kayange and Respicious Christopher Bakalemwa and Ndakibae Gabriel Mabega and Benson Richard Kidenya},
title = {Iron levels and Associated Factors Among Preterm Delivered Infants in Five Selected Health Facilities in Mwanza Region, Northwestern Tanzania
},
journal = {European Journal of Preventive Medicine},
volume = {12},
number = {5},
pages = {111-120},
doi = {10.11648/j.ejpm.20241205.11},
url = {https://doi.org/10.11648/j.ejpm.20241205.11},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ejpm.20241205.11},
abstract = {Background: It is estimated that, in Tanzania 11percent of babies are born prematurely each year. Preterm delivered infants are more prone to iron deficiency because most of mother to child iron transfer occurs in the third trimester. Methods: This was a hospital based cross sectional study, conducted in five selected health facilities in Mwanza city. Three hundred and fifty preterm delivered infants aged 6 to 30 weeks were included in the study. Participants’ information was obtained by using a pre-tested structured questionnaire. To determine body iron level, blood was collected to measure serum ferritin, full blood picture and C reactive protein. Results: In every 100 infants, 20 had low iron levels, 1 had latent iron deficiency, 3 had iron deficiency and 9 had iron deficiency anemia. Increase in infant’s age and complementary feeding with cow’s milk were significantly associated with iron deficiency anemia. In addition, hemoglobin level and mean corpuscular volume in combination is not a good alternative of serum ferritin in diagnosing low iron. Recommendations: Food fortification with iron and iron supplementation among preterm delivered infants are needed to prevent iron deficiency among these infants. Further studies to determine why older preterm delivered infants are more prone to iron deficiency anemia including type of food they eat are needed. Hemoglobin level and mean corpuscular volume can be used to rule out those without low iron but not to diagnose those with low iron level.
},
year = {2024}
}
TY - JOUR T1 - Iron levels and Associated Factors Among Preterm Delivered Infants in Five Selected Health Facilities in Mwanza Region, Northwestern Tanzania AU - Nakiete Samwel Machangu AU - Neema Mathias Kayange AU - Respicious Christopher Bakalemwa AU - Ndakibae Gabriel Mabega AU - Benson Richard Kidenya Y1 - 2024/09/20 PY - 2024 N1 - https://doi.org/10.11648/j.ejpm.20241205.11 DO - 10.11648/j.ejpm.20241205.11 T2 - European Journal of Preventive Medicine JF - European Journal of Preventive Medicine JO - European Journal of Preventive Medicine SP - 111 EP - 120 PB - Science Publishing Group SN - 2330-8230 UR - https://doi.org/10.11648/j.ejpm.20241205.11 AB - Background: It is estimated that, in Tanzania 11percent of babies are born prematurely each year. Preterm delivered infants are more prone to iron deficiency because most of mother to child iron transfer occurs in the third trimester. Methods: This was a hospital based cross sectional study, conducted in five selected health facilities in Mwanza city. Three hundred and fifty preterm delivered infants aged 6 to 30 weeks were included in the study. Participants’ information was obtained by using a pre-tested structured questionnaire. To determine body iron level, blood was collected to measure serum ferritin, full blood picture and C reactive protein. Results: In every 100 infants, 20 had low iron levels, 1 had latent iron deficiency, 3 had iron deficiency and 9 had iron deficiency anemia. Increase in infant’s age and complementary feeding with cow’s milk were significantly associated with iron deficiency anemia. In addition, hemoglobin level and mean corpuscular volume in combination is not a good alternative of serum ferritin in diagnosing low iron. Recommendations: Food fortification with iron and iron supplementation among preterm delivered infants are needed to prevent iron deficiency among these infants. Further studies to determine why older preterm delivered infants are more prone to iron deficiency anemia including type of food they eat are needed. Hemoglobin level and mean corpuscular volume can be used to rule out those without low iron but not to diagnose those with low iron level. VL - 12 IS - 5 ER -
Department of Paediatrics and Child Health, Sekou Touré Regional Referral Hospital, Mwanza, United Republic of Tanzania
Department of Paediatrics and Child Health, Catholic University of Health and Allied Sciences, Mwanza, United Republic of Tanzania
Department of Paediatrics and Child Health, Catholic University of Health and Allied Sciences, Mwanza, United Republic of Tanzania
Department of Clinical Research, National Institute for Medical Research, Mwanza Research Centre, Mwanza, Republic of Tanzania
Department of Biochemistry, Catholic University of Health and Allied Sciences, Mwanza, United Republic of Tanzania
Information