Background: Emergency cholecystectomy is the standard treatment for acute cholecystitis worldwide. However, in Ethiopia, it's only performed in a limited number of healthcare facilities, despite its recognition as the preferred treatment by many physicians. To date, there is no study examining the prevalence and outcomes of emergency cholecystectomy in Ethiopia. In our setting, this practice is relatively new, and its outcomes remain unstudied. Purpose: To assess the trends and outcome of emergency cholecystectomy at Yekatit 12 hospital medical college. Method: We employed a longitudinal study design, encompassing all patients who underwent emergency cholecystectomy throughout the study period. Data entry and analysis were conducted using SPSS statistical software version 25. Qualitative variables were depicted in frequencies and percentages, while continuous variables were summarized with mean and standard deviation (SD). Binary logistic regression was applied to evaluate the impact of independent variables on the outcome variable. A significance level of p < 0.05 was taken for statistical significance. Result: Between January 2022 and December 2023, 68 emergency cholecystectomies were performed. Females comprised 60.3% of the cases, with a mean age of 42.43 ± 14.03 years. Surgery for 44.1% of patients occurred between days 4 and 7 after symptom onset, while five patients underwent surgery after 10 days. The mean duration of surgery was 63.9 ± 17.14 minutes. Hospital stays ranged from 2 to 12 days, with a mean of 4.4 ± 2.47 days. Serum creatinine levels exceeding 1 mg/dl (p=0.004) were significantly linked to poor outcomes.
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited.
Acute cholecystitis, inflammation of the gallbladder, is mainly caused by gallstones, a common GI disorder affecting 10% of Western society. Over 80% of those with gallstones show no symptoms. However, 1-3% of symptomatic gallstone patients develop acute cholecystitis. According to a review, it occurs in 6-11% of patients with symptomatic gallstones over 7-11 years
[1]
Csikesz, N. G., et al., Surgeon volume metrics in laparoscopic cholecystectomy. Digestive diseases and sciences, 2010. 55: p. 2398-2405.
[2]
Gebresellassie, H. W. and G. Tamerat, Audit of surgical services in a teaching hospital in Addis Ababa, Ethiopia. BMC research notes, 2019. 12: p. 1-5.
[1, 2]
.
Cholecystectomy, the removal of the gallbladder, is the gold standard treatment for symptomatic gallstones and is common in the West. Whether emergency or elective, itis done via open surgery or laparoscopy. It is established since the late 1980s and widely adopted in the West. In the US, by 2019, 52.7% of acute cholecystitis patients received cholecystectomy during their first hospital stay
[2]
Gebresellassie, H. W. and G. Tamerat, Audit of surgical services in a teaching hospital in Addis Ababa, Ethiopia. BMC research notes, 2019. 12: p. 1-5.
[3]
Brunicardi, F., et al., Schwartz's principles of surgery, 10e. 2014: McGraw-hill.
[4]
Järvinen, H.. and J. Hästbacka, Early cholecystectomy for acute cholecystitis: a prospective randomized study. Annals of surgery, 1980. 191(4): p. 501-505.
[5]
Al-Khuwaitir, S. A., Early Versus Delayed Surgery for Acute Cholecystitis. Annals of Saudi Medicine, 1985. 5(2): p. 63-66.
[6]
Mytton, J., et al., Outcomes following an index emergency admission with cholecystitis: a national cohort study. Annals of surgery, 2021. 274(2): p. 367-374.
[2-6]
.
Currently emergency cholecystectomy is preferred for acute cholecystitis due to its better outcomes, including improved quality of life, lower morbidity rates, reduced hospital costs, and shorter stays
[7]
Thangavelu, A., S. Rosenbaum, and D. Thangavelu, Timing of cholecystectomy in acute cholecystitis. The Journal of emergency medicine, 2018. 54(6): p. 892-897.
[7]
. In New Zealand since March 2005, increased emergency cholecystectomies have reduced acute cases and likely decreased elective surgeries and waiting lists
[8]
Sakowska, M. M. and S. Connor, Index cholecystectomy for management of acute gallstone disease: a change of practice at a major New Zealand metropolitan centre. HPB, 2011. 13(10): p. 687-691.
[8]
. However, index cholecystectomy is limited in low and middle-income countries like Ethiopia, leading to worsened outcomes including higher morbidity, longer hospital stays, increased readmission rates, and higher costs for patients
[9]
Escartín, A., et al., Failure to perform index cholecystectomy during acute cholecystitis results in significant morbidity for patients who present with recurrence. HPB, 2019. 21(7): p. 876-882.
[10]
Banz, V., et al., Population-based analysis of 4113 patients with acute cholecystitis: defining the optimal time-point for laparoscopic cholecystectomy. Annals of surgery, 2011. 254(6): p. 964-970.
[9, 10]
.
In Ethiopia, there's limited research on acute cholecystitis treatment, and no report on the use of emergency cholecystectomy. Studying the trends and outcomes of emergency cholecystectomy would be highly beneficial, given the scarcity of published studies in Ethiopia on this topic.
2. Materials and Methods
2.1. Study Area and Period
The study was conducted in Y12HMC which is an academic institution found in Addis Ababa, Ethiopia under Addis Ababa City Administration. The study conductedfromJanuary 1st / 2022 - December 31st/2022 G. C.
2.2. Study Design
A longitudinal study design was used to assess trend and outcome of emergency cholecystectomy donein Yekatit 12 Hospital Medical College.
2.3. Source and Study Population
Source population: All patients admitted to surgical ward on emergency basis during the study period were considered as source population while those patients underwent emergency cholecystectomy for acute cholecystitis taken as study population.
2.4. Inclusion and Exclusion Criteria
All patients above age≥18 year-old who underwent emergency cholecystectomy for acute cholecystitis included in the study where as patients underwent emergency cholecystectomy for gall stone pancreatitis excluded from study population.
2.5. Study Variable
Independent variables:-Sociodemographic factors: age, sex; Disease related factors: duration of Illnesses, comorbidity, ASA, Grade of acute cholecystitis; Treatment related factors: timing of surgery, type of surgery, placement of drain, bile duct injury. Dependent Variable:-outcomeof emergency cholecystectomy.
2.6. Data Collection Technique and Quality Control
Data were gathered using a data extraction checklist from the electronic medical records and these checklists were designed through literature review and a pretest was done. Data collectors were trained junior surgery residents on the data collection tool and how to conduct data collection. The principal investigator supervised the data collection process and checked the completeness and consistency.
2.7. Data Analysis and Presentation
SPSS statistical software version 25 was used to enter and analyze data. Descriptive statistics such as frequency, percentage, mean, standard deviation (SD), or median were used for most of the variables, and results were presented using graphs, tables and narrative descriptions. Predictors with P-value ≤0.25 for univariate analysis were taken to the multivariable binary logistic regression to identify factors associated with emergency cholecystectomy outcome. A statistically significant association was declared based on adjusted odds ratio (AOR) with 95% confidence interval (CI) and p-values < 0.05. Model fitness was checked using Hosmer and Lemeshow goodness-of-fit test.
2.8. Ethical Consideration
Ethical clearance was obtained from the Institutional Review Board of Y12HMC (Reference number: Y12HMC 089/22, dated April 07/2022). Permission and written consent were taken from the college management. The information gained from the patients upon data collection was kept confidential by using codes for each card throughout the study. The procedures followed were by the ethical standards of the Helsinki Declaration.
3. Results
3.1. Patient Characteristics
The gender distribution shows that 60.3% of the population is female. The minimum and maximum age is 23 and 75 respectively. The mean age is 42.43 ± 14.03. Young adults, age range between 20 – 40 years of age, account for majority of the population. Only one patient has two previous history of acute cholecystitis while majority of the population has no previous attack of acute cholecystitis. Regarding patients physical status, only two patients are classified as ASA IV while majority are ASA I accounting for 76.5%. Most patients had mild form of cholecystitis (52.9%) and 4.4% had severe form. The rest has moderate acute cholecystitis. Most of the patients (85.3%) have no comorbidity. Diabetes mellitus (DM) is the most common comorbidity identified in this study followed by hypertension (HTN). Three patients had both DM and HTN (Table 1).
Table 1. Shows patient characteristics and profile.
Variables
Frequency
Percentage
P value
Sex
Male
27
39.7
Female
41
60.3
Age
20-40
39
50.6
40-60
20
25.6
60-80
9
13.7
Previous history of cholecystitis
0
48
70.6
1
19
27.99
2
1
1.5
ASA score
ASA I
52
76.5
ASA II
14
20.6
ASA III
2
2.9
Comorbidity
Yes
10
14.7
No
58
85.3
Severity grading
Mild
36
52.9
Moderate
30
42.6
Severe
4
4.4
Serum creatinine
< 1
54
79.4
≥ 1
14
20.6
0.004
3.2. Timing and Type of the Surgery
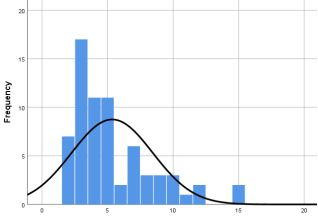
Of the patients who underwent surgery, 44.1% had their surgery between days 4 and 7 after the onset of symptoms. Five patients had their surgery after 10 days of onset of symptoms. This means that 79.4% of patients had their surgery in the first seven days after symptoms onset. The majority of surgeries were open, with only 4 patients undergoing laparoscopy (figure 1).
3.3. Duration of Surgery and Length of Hospital Stay
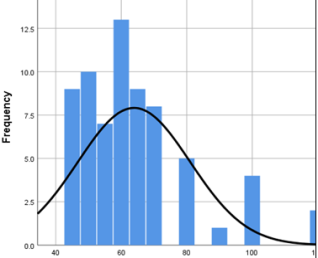
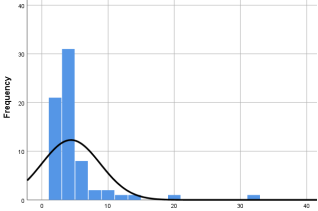
The duration of surgery ranges from 45 – 120 minutes with the mean of 63.9 ±17.14 minutes (figure 2). The length of hospital stay after surgery ranges from 2 – 12 days with the mean of 4.4 ± 2.47 days (figure 3).
Intraoperative biliary spillage was the most common intraoperative complication, with no biliary duct injuries observed. Nine patients had a sub-hepatic drain placed. Seven patients developed postoperative complications, with pulmonary complications (7.4%) being the most common, followed by surgical site infection (Table 2).
Table 2. Shows Intra Operative profile and out come.
Variables
Frequency
Percentage
Type of surgery
Open
4
5.9
laparoscopic
64
94.1
Timing of surgery
1-3
24
35.3
4-7
30
44.1
7-10
9
13.2
11-15
5
7.4
CVS achieved
Yes
51
75
No
17
25
Intraoperative accident
Yes
9
13.2
No
59
86.8
Bile duct injury
Yes
0
No
68
100
Duration of surgery
≤60
39
57.4
61-75
17
25.0
≥76
12
8.8
Placement of drain
Yes
9
13.2
No
59
86.8
SSI
Yes
6
8.8
No
62
91.2
3.5. Bailout Procedure and Achievement of Critical View of Safety (CVS)
CVS is achieved in 77.9% of the cases, fundus down approach and partial cholecystectomy is utilized in 20.6% and 1.5% of the cases respectively. In the bivariate analysis the factors that were found to be significantly associated with poor outcome (p-value <0.05) were serum creatinine. The odds of poor outcome among patients with serum creatinine ≥ 1 mg/dl was 9.7 times (COR; 95% CI: 2.1-44.9) higher than those with serum creatinine level ˂ 1 mg/dl (Table 2).
4. Discussion
Gallstones pose a significant health concern, with prevalence estimates ranging from 11% to 36%. They can result in various complications, including surgical morbidity and admissions. Acute cholecystitis, a frequent presentation of gallstone disease, contributes to 5% of emergency admissions. The preferred treatment for acute cholecystitis is emergency laparoscopic cholecystectomy
[1]
Csikesz, N. G., et al., Surgeon volume metrics in laparoscopic cholecystectomy. Digestive diseases and sciences, 2010. 55: p. 2398-2405.
[1]
. However, this practice is not widely available in our country due to a lack of expertise and equipment. Additionally there is neither population nor institutional based study on the trends and outcome of emergency cholecystectomy
[10]
Banz, V., et al., Population-based analysis of 4113 patients with acute cholecystitis: defining the optimal time-point for laparoscopic cholecystectomy. Annals of surgery, 2011. 254(6): p. 964-970.
[10]
.
The mean age of the patients in this study group is comparable to what has been reported in other studies
[11]
Babu, H., et al., A prospective study on emergency laparoscopic or open cholecystectomy in acute cholecystitis in a tertiary care hospital. International Surgery Journal, 2019. 6(7): p. 2525-2532.
[12]
Amer, N. M., et al., Emergency versus elective cholecystectomy: Experience at a university hospital in the Eastern Province, Saudi Arabia. Journal of Family and Community Medicine, 2023. 30(1): p. 37-41.
[13]
Tayeb, M., F. Rauf, and N. Bakhtiar, Safety and feasibility of laparoscopic cholecystectomy in acute cholecystitis. J Coll Physicians Surg Pak, 2018. 28(10): p. 798-800.
[14]
Shafqat, R., A. Muhammad, and B. Muhammad Qasim, Outcomes of laparoscopic cholecystectomy in acute cholecystitis. 2017.
[11-14]
and younger than reported in some of studies
[10]
Banz, V., et al., Population-based analysis of 4113 patients with acute cholecystitis: defining the optimal time-point for laparoscopic cholecystectomy. Annals of surgery, 2011. 254(6): p. 964-970.
[15]
Khan, M. N., et al., Urgent cholecystectomy for acute cholecystitis in a district general hospital–is it feasible? The Annals of The Royal College of Surgeons of England, 2009. 91(1): p. 30-34.
[10, 15]
. The high female preponderance observed in this study is a well-established finding that is consistent with the results of other studies
[10]
Banz, V., et al., Population-based analysis of 4113 patients with acute cholecystitis: defining the optimal time-point for laparoscopic cholecystectomy. Annals of surgery, 2011. 254(6): p. 964-970.
[11]
Babu, H., et al., A prospective study on emergency laparoscopic or open cholecystectomy in acute cholecystitis in a tertiary care hospital. International Surgery Journal, 2019. 6(7): p. 2525-2532.
[12]
Amer, N. M., et al., Emergency versus elective cholecystectomy: Experience at a university hospital in the Eastern Province, Saudi Arabia. Journal of Family and Community Medicine, 2023. 30(1): p. 37-41.
[13]
Tayeb, M., F. Rauf, and N. Bakhtiar, Safety and feasibility of laparoscopic cholecystectomy in acute cholecystitis. J Coll Physicians Surg Pak, 2018. 28(10): p. 798-800.
[14]
Shafqat, R., A. Muhammad, and B. Muhammad Qasim, Outcomes of laparoscopic cholecystectomy in acute cholecystitis. 2017.
[16]
Gurusamy, K. S., et al., Early versus delayed laparoscopic cholecystectomy for people with acute cholecystitis. Cochrane Database of Systematic Reviews, 2013(6).
[10-14, 16]
. However compared to elective cases it is much lower
[2]
Gebresellassie, H. W. and G. Tamerat, Audit of surgical services in a teaching hospital in Addis Ababa, Ethiopia. BMC research notes, 2019. 12: p. 1-5.
[12]
Amer, N. M., et al., Emergency versus elective cholecystectomy: Experience at a university hospital in the Eastern Province, Saudi Arabia. Journal of Family and Community Medicine, 2023. 30(1): p. 37-41.
[2, 12]
. In this study, the most common age range for the cases was 20-60 years old. This is lower than the most common age range in other studies, which is 40-60 years old
[11]
Babu, H., et al., A prospective study on emergency laparoscopic or open cholecystectomy in acute cholecystitis in a tertiary care hospital. International Surgery Journal, 2019. 6(7): p. 2525-2532.
[17]
Csikesz, N. G., J. F. Tseng, and S. A. Shah, Trends in surgical management for acute cholecystitis. Surgery, 2008. 144(2): p. 283-289.
[11, 17]
.
The rate of previous admission for AC is important because it can affect the patient's risk of complications and the outcome of surgery. Patients with a previous admission for AC are more likely to have a more severe case of AC and are more likely to experience complications after surgery. The rate of previous admission for acute cholecystitis varies depending on the study population. It was lower in this study compared to other studies
[1]
Csikesz, N. G., et al., Surgeon volume metrics in laparoscopic cholecystectomy. Digestive diseases and sciences, 2010. 55: p. 2398-2405.
[15]
Khan, M. N., et al., Urgent cholecystectomy for acute cholecystitis in a district general hospital–is it feasible? The Annals of The Royal College of Surgeons of England, 2009. 91(1): p. 30-34.
[1, 15]
.
Studies found that patients with comorbidities are more likely to experience complications after emergency cholecystectomy. Patients with comorbidities should be carefully evaluated before surgery to ensure that they are good candidates for the procedure. The results of the study showed that the rate of comorbidity was lower in this study (14.7%) than in studies done in developed countries 20-40. The study also found that the rate of comorbidity was lower than the rate in patients undergoing elective cholecystectomy in our country (20%)
[2]
Gebresellassie, H. W. and G. Tamerat, Audit of surgical services in a teaching hospital in Addis Ababa, Ethiopia. BMC research notes, 2019. 12: p. 1-5.
[2]
. The lower rate of comorbidity in this study may be due to the fact that the study population was younger and had less severe disease than the populations in the studies done in developed countries.
The severity of acute cholecystitis has a significant effect on the outcome of emergency cholecystectomy. Patients with more severe acute cholecystitis are more likely to experience complications after surgery and have a longer hospital stay
[17]
Csikesz, N. G., J. F. Tseng, and S. A. Shah, Trends in surgical management for acute cholecystitis. Surgery, 2008. 144(2): p. 283-289.
[17]
. The rate of mild form acute cholecystitis in this study
[18]
Abebe, H. and M. Bekele, Trends and Outcomes of Cholecystectomy; a comparative study of open and laparoscopic cholecystectomy, a Three Year Experience in a Teaching Hospital, Addis Ababa. Ethiopian Medical Journal, 2021. 59(01).
[18]
(52.9) is less common compared to studies done in Singapore (56.4%) and South Africa (94%)
[1]
Csikesz, N. G., et al., Surgeon volume metrics in laparoscopic cholecystectomy. Digestive diseases and sciences, 2010. 55: p. 2398-2405.
[19]
Yokoe, M., et al., Tokyo Guidelines 2018: diagnostic criteria and severity grading of acute cholecystitis (with videos). Journal of Hepato‐biliary‐pancreatic Sciences, 2018. 25(1): p. 41-54.
[1, 19]
and one patient with severe cholecystitis died during the course of this study. In this study, the likelihood of using bailout procedures and drains increased as the severity of the disease increased. The median operating time also increased as the severity of the disease increased. The risk of poor outcomes also increased.
An increase in the complication rate and need of conversion to open cholecystectomy has been reported when the time from symptom appearance to surgery was prolonged
[16]
Gurusamy, K. S., et al., Early versus delayed laparoscopic cholecystectomy for people with acute cholecystitis. Cochrane Database of Systematic Reviews, 2013(6).
[16]
World Society of Emergency Surgery updated guidelines for the diagnosis and treatment of acute calculus cholecystitis 2020 recommend Emergency cholecystectomy be performed as soon as possible, within 7 days from hospital admission and within 10 days from the onset of symptoms
[4]
Järvinen, H.. and J. Hästbacka, Early cholecystectomy for acute cholecystitis: a prospective randomized study. Annals of surgery, 1980. 191(4): p. 501-505.
[4]
. In this study, 44% of patients were operated on 4-7 days after the onset of symptoms, and 7% were operated on 11-14 days after the onset of symptoms. Data from all consecutive patients undergoing surgery for acute cholecystitis on index admission in England from 1997 to 2012 shows, 64.6% of patients underwent surgery between days 0 and 3 of admission, 24.3% between days 4–7 and 11.0% had surgery after day 8
[20]
Wiggins, T., et al., Optimum timing of emergency cholecystectomy for acute cholecystitis in England: population-based cohort study. Surgical Endoscopy, 2019. 33: p. 2495-2502.
[20]
.
Bile duct injuries (BDIs) are dangerous complications of cholecystectomy, occurring more often since the introduction and widespread adoption of laparoscopy (0.4–1.5% of cases) compared to open cholecystectomy (0.2–0.3% of cases)
[3]
Brunicardi, F., et al., Schwartz's principles of surgery, 10e. 2014: McGraw-hill.
[4]
Järvinen, H.. and J. Hästbacka, Early cholecystectomy for acute cholecystitis: a prospective randomized study. Annals of surgery, 1980. 191(4): p. 501-505.
[3, 4]
. However there is no bile duct injury is documented in this study.
The mean duration of surgery of emergency cholecystectomy varies from study to study. This is likely due to a number of factors, including the type of surgery performed (open vs. laparoscopic), the severity of the patient's condition, and the experience of the surgeon. The mean operation time in this study was higher than those observed in laparoscopic cholecystectomy, but comparable to open cholecystectomy. It was much lower than the mean operation time in a study conducted in South Africa
[13]
Tayeb, M., F. Rauf, and N. Bakhtiar, Safety and feasibility of laparoscopic cholecystectomy in acute cholecystitis. J Coll Physicians Surg Pak, 2018. 28(10): p. 798-800.
[14]
Shafqat, R., A. Muhammad, and B. Muhammad Qasim, Outcomes of laparoscopic cholecystectomy in acute cholecystitis. 2017.
[15]
Khan, M. N., et al., Urgent cholecystectomy for acute cholecystitis in a district general hospital–is it feasible? The Annals of The Royal College of Surgeons of England, 2009. 91(1): p. 30-34.
[17]
Csikesz, N. G., J. F. Tseng, and S. A. Shah, Trends in surgical management for acute cholecystitis. Surgery, 2008. 144(2): p. 283-289.
[13-15, 17]
.
The mean duration of hospital stay after emergency cholecystectomy varies from study to study. This is likely due to a number of factors, including the type of surgery performed (open vs. laparoscopic), the severity of the patient's condition, and the availability of resources. In this study it is lower than in most of the study but higher than in elective group
[2]
Gebresellassie, H. W. and G. Tamerat, Audit of surgical services in a teaching hospital in Addis Ababa, Ethiopia. BMC research notes, 2019. 12: p. 1-5.
[12]
Amer, N. M., et al., Emergency versus elective cholecystectomy: Experience at a university hospital in the Eastern Province, Saudi Arabia. Journal of Family and Community Medicine, 2023. 30(1): p. 37-41.
[13]
Tayeb, M., F. Rauf, and N. Bakhtiar, Safety and feasibility of laparoscopic cholecystectomy in acute cholecystitis. J Coll Physicians Surg Pak, 2018. 28(10): p. 798-800.
[21]
Prakash, K., et al., Laparoscopic cholecystectomy in acute cholecystitis. Surgical Endoscopy and Other Interventional Techniques, 2002. 16: p. 180-183.
[22]
Coccolini, F., et al., Open versus laparoscopic cholecystectomy in acute cholecystitis. Systematic review and meta-analysis. International journal of surgery, 2015. 18: p. 196-204.
[2, 12, 13, 21, 22]
.
In this study, 5 (6.5%) patients were considered to have a poor outcome, either due to death or postoperative complications and it is less compared with other studies
[4]
Järvinen, H.. and J. Hästbacka, Early cholecystectomy for acute cholecystitis: a prospective randomized study. Annals of surgery, 1980. 191(4): p. 501-505.
[10]
Banz, V., et al., Population-based analysis of 4113 patients with acute cholecystitis: defining the optimal time-point for laparoscopic cholecystectomy. Annals of surgery, 2011. 254(6): p. 964-970.
[12]
Amer, N. M., et al., Emergency versus elective cholecystectomy: Experience at a university hospital in the Eastern Province, Saudi Arabia. Journal of Family and Community Medicine, 2023. 30(1): p. 37-41.
[15]
Khan, M. N., et al., Urgent cholecystectomy for acute cholecystitis in a district general hospital–is it feasible? The Annals of The Royal College of Surgeons of England, 2009. 91(1): p. 30-34.
[22]
Coccolini, F., et al., Open versus laparoscopic cholecystectomy in acute cholecystitis. Systematic review and meta-analysis. International journal of surgery, 2015. 18: p. 196-204.
[4, 10, 12, 15, 22]
.
The main limitation of this study is the small sample size, which makes the results statistically insignificant. The strength of this study is that it is the first of its kind in our country. This means that it provides valuable insights into the topic, and it will serve as a baseline for similar research in the future.
5. Conclusion
In conclusion, the outcome of emergency cholecystectomy is generally favorable, with low mortality and morbidity rates. This study found that the overall mortality rate for emergency cholecystectomy was 1.5%. The morbidity rate was 6.5%, with the most common complications being surgical site infection (8.8%). The study also found that the outcome was better for patients who were younger, and serum creatinine less than 1 mg/dl.
Limitation
The study was conducted in a single institution, and the results may not be generalizable to other studies.
Abbreviations
AC
Acute Cholecystitis
ASA
American Society of Anesthesiologist
BDI
Bile Duct Injury
CVS
Critical View of Safety
WSES
World Society of Emergency Surgery
Conflicts of Interest
The authors declare no conflicts of interest.
References
[1]
Csikesz, N. G., et al., Surgeon volume metrics in laparoscopic cholecystectomy. Digestive diseases and sciences, 2010. 55: p. 2398-2405.
[2]
Gebresellassie, H. W. and G. Tamerat, Audit of surgical services in a teaching hospital in Addis Ababa, Ethiopia. BMC research notes, 2019. 12: p. 1-5.
[3]
Brunicardi, F., et al., Schwartz's principles of surgery, 10e. 2014: McGraw-hill.
[4]
Järvinen, H.. and J. Hästbacka, Early cholecystectomy for acute cholecystitis: a prospective randomized study. Annals of surgery, 1980. 191(4): p. 501-505.
[5]
Al-Khuwaitir, S. A., Early Versus Delayed Surgery for Acute Cholecystitis. Annals of Saudi Medicine, 1985. 5(2): p. 63-66.
[6]
Mytton, J., et al., Outcomes following an index emergency admission with cholecystitis: a national cohort study. Annals of surgery, 2021. 274(2): p. 367-374.
[7]
Thangavelu, A., S. Rosenbaum, and D. Thangavelu, Timing of cholecystectomy in acute cholecystitis. The Journal of emergency medicine, 2018. 54(6): p. 892-897.
[8]
Sakowska, M. M. and S. Connor, Index cholecystectomy for management of acute gallstone disease: a change of practice at a major New Zealand metropolitan centre. HPB, 2011. 13(10): p. 687-691.
[9]
Escartín, A., et al., Failure to perform index cholecystectomy during acute cholecystitis results in significant morbidity for patients who present with recurrence. HPB, 2019. 21(7): p. 876-882.
[10]
Banz, V., et al., Population-based analysis of 4113 patients with acute cholecystitis: defining the optimal time-point for laparoscopic cholecystectomy. Annals of surgery, 2011. 254(6): p. 964-970.
[11]
Babu, H., et al., A prospective study on emergency laparoscopic or open cholecystectomy in acute cholecystitis in a tertiary care hospital. International Surgery Journal, 2019. 6(7): p. 2525-2532.
[12]
Amer, N. M., et al., Emergency versus elective cholecystectomy: Experience at a university hospital in the Eastern Province, Saudi Arabia. Journal of Family and Community Medicine, 2023. 30(1): p. 37-41.
[13]
Tayeb, M., F. Rauf, and N. Bakhtiar, Safety and feasibility of laparoscopic cholecystectomy in acute cholecystitis. J Coll Physicians Surg Pak, 2018. 28(10): p. 798-800.
[14]
Shafqat, R., A. Muhammad, and B. Muhammad Qasim, Outcomes of laparoscopic cholecystectomy in acute cholecystitis. 2017.
[15]
Khan, M. N., et al., Urgent cholecystectomy for acute cholecystitis in a district general hospital–is it feasible? The Annals of The Royal College of Surgeons of England, 2009. 91(1): p. 30-34.
[16]
Gurusamy, K. S., et al., Early versus delayed laparoscopic cholecystectomy for people with acute cholecystitis. Cochrane Database of Systematic Reviews, 2013(6).
[17]
Csikesz, N. G., J. F. Tseng, and S. A. Shah, Trends in surgical management for acute cholecystitis. Surgery, 2008. 144(2): p. 283-289.
[18]
Abebe, H. and M. Bekele, Trends and Outcomes of Cholecystectomy; a comparative study of open and laparoscopic cholecystectomy, a Three Year Experience in a Teaching Hospital, Addis Ababa. Ethiopian Medical Journal, 2021. 59(01).
[19]
Yokoe, M., et al., Tokyo Guidelines 2018: diagnostic criteria and severity grading of acute cholecystitis (with videos). Journal of Hepato‐biliary‐pancreatic Sciences, 2018. 25(1): p. 41-54.
[20]
Wiggins, T., et al., Optimum timing of emergency cholecystectomy for acute cholecystitis in England: population-based cohort study. Surgical Endoscopy, 2019. 33: p. 2495-2502.
[21]
Prakash, K., et al., Laparoscopic cholecystectomy in acute cholecystitis. Surgical Endoscopy and Other Interventional Techniques, 2002. 16: p. 180-183.
[22]
Coccolini, F., et al., Open versus laparoscopic cholecystectomy in acute cholecystitis. Systematic review and meta-analysis. International journal of surgery, 2015. 18: p. 196-204.
Kebede, T., Desta, G., Kibret, A., Amtataw, W. (2024). Outcome of Emergency Cholecystectomy at Yekatit 12 Hospital Medical College, Addis Ababa, Ethiopia. Clinical Medicine Research, 13(4), 39-44. https://doi.org/10.11648/j.cmr.20241304.11
Kebede T, Desta G, Kibret A, Amtataw W. Outcome of Emergency Cholecystectomy at Yekatit 12 Hospital Medical College, Addis Ababa, Ethiopia. Clin Med Res. 2024;13(4):39-44. doi: 10.11648/j.cmr.20241304.11
@article{10.11648/j.cmr.20241304.11,
author = {Tolera Kebede and Getachew Desta and Alemu Kibret and Wondwossen Amtataw},
title = {Outcome of Emergency Cholecystectomy at Yekatit 12 Hospital Medical College, Addis Ababa, Ethiopia
},
journal = {Clinical Medicine Research},
volume = {13},
number = {4},
pages = {39-44},
doi = {10.11648/j.cmr.20241304.11},
url = {https://doi.org/10.11648/j.cmr.20241304.11},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.cmr.20241304.11},
abstract = {Background: Emergency cholecystectomy is the standard treatment for acute cholecystitis worldwide. However, in Ethiopia, it's only performed in a limited number of healthcare facilities, despite its recognition as the preferred treatment by many physicians. To date, there is no study examining the prevalence and outcomes of emergency cholecystectomy in Ethiopia. In our setting, this practice is relatively new, and its outcomes remain unstudied. Purpose: To assess the trends and outcome of emergency cholecystectomy at Yekatit 12 hospital medical college. Method: We employed a longitudinal study design, encompassing all patients who underwent emergency cholecystectomy throughout the study period. Data entry and analysis were conducted using SPSS statistical software version 25. Qualitative variables were depicted in frequencies and percentages, while continuous variables were summarized with mean and standard deviation (SD). Binary logistic regression was applied to evaluate the impact of independent variables on the outcome variable. A significance level of p Result: Between January 2022 and December 2023, 68 emergency cholecystectomies were performed. Females comprised 60.3% of the cases, with a mean age of 42.43 ± 14.03 years. Surgery for 44.1% of patients occurred between days 4 and 7 after symptom onset, while five patients underwent surgery after 10 days. The mean duration of surgery was 63.9 ± 17.14 minutes. Hospital stays ranged from 2 to 12 days, with a mean of 4.4 ± 2.47 days. Serum creatinine levels exceeding 1 mg/dl (p=0.004) were significantly linked to poor outcomes.},
year = {2024}
}
TY - JOUR
T1 - Outcome of Emergency Cholecystectomy at Yekatit 12 Hospital Medical College, Addis Ababa, Ethiopia
AU - Tolera Kebede
AU - Getachew Desta
AU - Alemu Kibret
AU - Wondwossen Amtataw
Y1 - 2024/07/23
PY - 2024
N1 - https://doi.org/10.11648/j.cmr.20241304.11
DO - 10.11648/j.cmr.20241304.11
T2 - Clinical Medicine Research
JF - Clinical Medicine Research
JO - Clinical Medicine Research
SP - 39
EP - 44
PB - Science Publishing Group
SN - 2326-9057
UR - https://doi.org/10.11648/j.cmr.20241304.11
AB - Background: Emergency cholecystectomy is the standard treatment for acute cholecystitis worldwide. However, in Ethiopia, it's only performed in a limited number of healthcare facilities, despite its recognition as the preferred treatment by many physicians. To date, there is no study examining the prevalence and outcomes of emergency cholecystectomy in Ethiopia. In our setting, this practice is relatively new, and its outcomes remain unstudied. Purpose: To assess the trends and outcome of emergency cholecystectomy at Yekatit 12 hospital medical college. Method: We employed a longitudinal study design, encompassing all patients who underwent emergency cholecystectomy throughout the study period. Data entry and analysis were conducted using SPSS statistical software version 25. Qualitative variables were depicted in frequencies and percentages, while continuous variables were summarized with mean and standard deviation (SD). Binary logistic regression was applied to evaluate the impact of independent variables on the outcome variable. A significance level of p Result: Between January 2022 and December 2023, 68 emergency cholecystectomies were performed. Females comprised 60.3% of the cases, with a mean age of 42.43 ± 14.03 years. Surgery for 44.1% of patients occurred between days 4 and 7 after symptom onset, while five patients underwent surgery after 10 days. The mean duration of surgery was 63.9 ± 17.14 minutes. Hospital stays ranged from 2 to 12 days, with a mean of 4.4 ± 2.47 days. Serum creatinine levels exceeding 1 mg/dl (p=0.004) were significantly linked to poor outcomes.
VL - 13
IS - 4
ER -
Kebede, T., Desta, G., Kibret, A., Amtataw, W. (2024). Outcome of Emergency Cholecystectomy at Yekatit 12 Hospital Medical College, Addis Ababa, Ethiopia. Clinical Medicine Research, 13(4), 39-44. https://doi.org/10.11648/j.cmr.20241304.11
Kebede T, Desta G, Kibret A, Amtataw W. Outcome of Emergency Cholecystectomy at Yekatit 12 Hospital Medical College, Addis Ababa, Ethiopia. Clin Med Res. 2024;13(4):39-44. doi: 10.11648/j.cmr.20241304.11
@article{10.11648/j.cmr.20241304.11,
author = {Tolera Kebede and Getachew Desta and Alemu Kibret and Wondwossen Amtataw},
title = {Outcome of Emergency Cholecystectomy at Yekatit 12 Hospital Medical College, Addis Ababa, Ethiopia
},
journal = {Clinical Medicine Research},
volume = {13},
number = {4},
pages = {39-44},
doi = {10.11648/j.cmr.20241304.11},
url = {https://doi.org/10.11648/j.cmr.20241304.11},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.cmr.20241304.11},
abstract = {Background: Emergency cholecystectomy is the standard treatment for acute cholecystitis worldwide. However, in Ethiopia, it's only performed in a limited number of healthcare facilities, despite its recognition as the preferred treatment by many physicians. To date, there is no study examining the prevalence and outcomes of emergency cholecystectomy in Ethiopia. In our setting, this practice is relatively new, and its outcomes remain unstudied. Purpose: To assess the trends and outcome of emergency cholecystectomy at Yekatit 12 hospital medical college. Method: We employed a longitudinal study design, encompassing all patients who underwent emergency cholecystectomy throughout the study period. Data entry and analysis were conducted using SPSS statistical software version 25. Qualitative variables were depicted in frequencies and percentages, while continuous variables were summarized with mean and standard deviation (SD). Binary logistic regression was applied to evaluate the impact of independent variables on the outcome variable. A significance level of p Result: Between January 2022 and December 2023, 68 emergency cholecystectomies were performed. Females comprised 60.3% of the cases, with a mean age of 42.43 ± 14.03 years. Surgery for 44.1% of patients occurred between days 4 and 7 after symptom onset, while five patients underwent surgery after 10 days. The mean duration of surgery was 63.9 ± 17.14 minutes. Hospital stays ranged from 2 to 12 days, with a mean of 4.4 ± 2.47 days. Serum creatinine levels exceeding 1 mg/dl (p=0.004) were significantly linked to poor outcomes.},
year = {2024}
}
TY - JOUR
T1 - Outcome of Emergency Cholecystectomy at Yekatit 12 Hospital Medical College, Addis Ababa, Ethiopia
AU - Tolera Kebede
AU - Getachew Desta
AU - Alemu Kibret
AU - Wondwossen Amtataw
Y1 - 2024/07/23
PY - 2024
N1 - https://doi.org/10.11648/j.cmr.20241304.11
DO - 10.11648/j.cmr.20241304.11
T2 - Clinical Medicine Research
JF - Clinical Medicine Research
JO - Clinical Medicine Research
SP - 39
EP - 44
PB - Science Publishing Group
SN - 2326-9057
UR - https://doi.org/10.11648/j.cmr.20241304.11
AB - Background: Emergency cholecystectomy is the standard treatment for acute cholecystitis worldwide. However, in Ethiopia, it's only performed in a limited number of healthcare facilities, despite its recognition as the preferred treatment by many physicians. To date, there is no study examining the prevalence and outcomes of emergency cholecystectomy in Ethiopia. In our setting, this practice is relatively new, and its outcomes remain unstudied. Purpose: To assess the trends and outcome of emergency cholecystectomy at Yekatit 12 hospital medical college. Method: We employed a longitudinal study design, encompassing all patients who underwent emergency cholecystectomy throughout the study period. Data entry and analysis were conducted using SPSS statistical software version 25. Qualitative variables were depicted in frequencies and percentages, while continuous variables were summarized with mean and standard deviation (SD). Binary logistic regression was applied to evaluate the impact of independent variables on the outcome variable. A significance level of p Result: Between January 2022 and December 2023, 68 emergency cholecystectomies were performed. Females comprised 60.3% of the cases, with a mean age of 42.43 ± 14.03 years. Surgery for 44.1% of patients occurred between days 4 and 7 after symptom onset, while five patients underwent surgery after 10 days. The mean duration of surgery was 63.9 ± 17.14 minutes. Hospital stays ranged from 2 to 12 days, with a mean of 4.4 ± 2.47 days. Serum creatinine levels exceeding 1 mg/dl (p=0.004) were significantly linked to poor outcomes.
VL - 13
IS - 4
ER -