Objective: To assess clinicians’ perspectives and preferences in hypertension management, with a focus on telmisartan-based therapies in Indian settings. Methodology: The cross-sectional study was conducted among 973 clinicians across India using a 23-item structured questionnaire, which collected information on treatment approaches, the use of fixed-dose combinations (FDCs), and treatment preferences. Additionally, an extended analysis comprising 15 supplementary questions was conducted with a subset of clinicians (n = 93) to further explore clinical practices in specific scenarios. The data were analyzed using descriptive statistics and presented as frequencies and percentages. Results: A large proportion of clinicians (76.67%) preferred FDCs when two or more drugs are required for hypertension management. Telmisartan was the most commonly preferred angiotensin receptor blocker (ARB), as reported by the majority (96.92%) of clinicians, with approximately 52% reporting its frequent use in combination with calcium channel blockers (CCBs). Among these, amlodipine is the most commonly preferred agent in young patients with uncontrolled hypertension, as reported by 67% of participants. Nearly half (50.15%) of respondents reported that chlorthalidone is the preferred diuretic in combination with telmisartan. About 57% of participants reported that metoprolol is the most commonly used beta-blocker in patients with hypertension and coronary artery disease. Telmisartan + CCB + beta-blocker is the most commonly preferred triple-drug combination, as indicated by 49% of participants, and 64% reported preferring this combination, particularly in young patients with uncontrolled hypertension. Conclusion: The survey findings highlight a strong preference for telmisartan-based therapies and FDCs among Indian clinicians, reflecting current clinical practices in hypertension management. The widespread use of ARBs, particularly in younger patients, underscores their perceived efficacy and tolerability.
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited.
Hypertension remains a major and growing clinical and public health challenge due to its high prevalence and persistently inadequate blood pressure (BP) control in routine practice. Globally, the burden has nearly doubled from 650 million adults in 1990 to approximately 1.4 billion, with a disproportionate impact on low- and middle-income countries.
[1]
World Health Organization. Hypertension. [cited 2026 Apr 14]. Available from:
Despite advances in diagnosis and treatment, BP control remains suboptimal, increasing the risk of complications such as stroke, myocardial infarction, and heart failure.
[2]
Kim HJ, Kim BS, Kim H, Lee J, Shin JH, Sung KC. Impact of blood pressure and medication adherence on clinical outcomes in patients with hypertension. Front Med (Lausanne). 2025; 12: 1564791.
In India, hypertension affects approximately 25-30% of adults, with the National Family Health Survey (NFHS-5) estimating a prevalence of 22.6%, higher among men (24.1%) than women (21.2%), and rising to 48.4% among individuals aged ≥60 years.
[3]
Gupta R, Gupta S. Hypertension in India: Trends in Prevalence, Awareness, Treatment and Control. RUHS Journal of Health Science. 2017; 2: 40.
[4]
Mohammad R, Bansod DW. Hypertension in India: a gender-based study of prevalence and associated risk factors. BMC Public Health. 2024; 24(1): 2681.
Urban populations show slightly higher prevalence than rural populations, reflecting the impact of urbanization, sedentary lifestyles, unhealthy dietary habits, and psychosocial stress.
[4]
Mohammad R, Bansod DW. Hypertension in India: a gender-based study of prevalence and associated risk factors. BMC Public Health. 2024; 24(1): 2681.
However, persistent gaps in awareness, treatment, and long-term adherence continue to limit effective BP control.
[5]
Londoño Agudelo E, Pérez Ospina V, Battaglioli T, Taborda Pérez C, Gómez-Arias R, Van der Stuyft P. Gaps in hypertension care and control: a population-based study in low-income urban Medellin, Colombia. Trop Med Int Health. 2021; 26(8): 895-907.
Optimal management of hypertension often requires a combination of pharmacological agents, particularly in patients with uncontrolled BP or high cardiovascular risk. Fixed-dose combinations (FDCs) are increasingly recommended in clinical guidelines due to their ability to improve adherence, reduce pill burden, and enhance therapeutic efficacy. However, the treatment patterns may vary based on physician preferences, patient characteristics, and healthcare system factors.
[6]
DiPette DJ, Skeete J, Ridley E, Campbell NRC, Lopez-Jaramillo P, Kishore SP, et al. Fixed-dose combination pharmacologic therapy to improve hypertension control worldwide: Clinical perspective and policy implications. J Clin Hypertens (Greenwich). 2018; 21(1): 4-15.
Jafari EA. Fixed-dose combination antihypertensive therapy and healthcare utilization in U.S. adults with hypertension: a propensity score–based analysis of a nationally representative population. Front. Pharmacol. 17: 1787754.
Among the available antihypertensive agents, angiotensin receptor blockers (ARBs) are widely utilized due to their favorable efficacy and tolerability profile.
[8]
Patel P, Launico MV. Angiotensin II Receptor Blockers (ARB). In: StatPearls. StatPearls Publishing; 2026. Available from:
Telmisartan, in particular, has gained prominence owing to its long half-life, sustained 24-hour BP control, and additional cardiometabolic benefits.
[9]
Gosse P. A Review of Telmisartan in the Treatment of Hypertension: Blood Pressure Control in the Early Morning Hours. Vasc Health Risk Manag. 2006; 2(3): 195-201.
It is frequently preferred both as monotherapy and in combination with other drug classes, including calcium channel blockers (CCBs), diuretics, and beta-blockers, especially in patients requiring intensified therapy.
[10]
Kant S, Sharma A, Kumar V, Gore P, Pramanik S, Bhushan S, et al. A cross-sectional study on the drug utilization of fixed-dose combination of telmisartan plus metoprolol in patients with hypertension across various clinics in India. Hypertens Open Access. 2026; 3: 105.
It exerts its antihypertensive effect by selectively blocking the angiotensin II type 1 (AT1) receptor, thereby inhibiting vasoconstriction, aldosterone secretion, and sympathetic activation. This results in vasodilation and reduced peripheral vascular resistance. In addition, telmisartan has been shown to possess partial peroxisome proliferator-activated receptor-gamma (PPAR-γ) agonistic activity, which may contribute to its beneficial effects on metabolic parameters. Its pharmacological profile, along with its frequent use in combination with other antihypertensive agents such as CCBs, diuretics, and beta-blockers, underscores its role in contemporary hypertension management.
[11]
Telmisartan. In: LiverTox: Clinical and Research Information on Drug-Induced Liver Injury. National Institute of Diabetes and Digestive and Kidney Diseases; 2012. Available from:
While clinical studies provide robust evidence for the efficacy and safety of antihypertensive therapies, there is a dearth of studies among clinicians in actual practice. Understanding clinicians’ practices and preferences, especially with respect to commonly used agents such as telmisartan and its combinations, is essential to bridge the gap between evidence and practice. Therefore, the present survey aims to assess clinicians’ perspectives and preferences in hypertension management, with a particular focus on the utilization, perceived safety, and effectiveness of telmisartan-based therapies in the management of hypertension among Indian clinicians.
2. Materials and Methods
2.1. Study Settings
A cross-sectional study was carried out among clinicians specialized in managing hypertension across various clinical settings in India from June 2025 to December 2025. The study was performed in accordance with Bangalore Ethics, an Independent Ethics Committee (ECR/355/Indt/KA/2022), which was recognized by the Indian Regulatory Authority, the Drug Controller General of India.
2.2. Study Participants
A convenient sampling technique was used, and an invitation was sent to professionals across India based on their expertise and experience in treating hypertension in the month of March 2025 for participation in this Indian survey. About 973 clinicians from major cities of all Indian states, representing the geographical distribution, shared their willingness to participate and provide necessary data.
2.3. Study Procedure
The questionnaire booklet titled HyTec (Hypertension therapy in combination study) was sent to 973 doctors (Cardiologists, Cardiothoracic Surgeons, Neurologists, Nephrologists, Diabetologists, Endocrinologists, and Consulting physicians) who were interested in participating in the study. The questionnaire comprised 23 items common to both phases of the study, focusing on the burden and types of hypertension, treatment approaches, use of fixed-dose combinations, and treatment patterns, particularly related to ARBs and telmisartan-based therapies. In addition, 15 supplementary questions were administered to a subset of clinicians (n = 93) as part of an extended survey to further explore aspects such as BP variability, treatment challenges, patient adherence, and physician preferences in clinical practice. Reliability, as determined by a split-half test (coefficient alpha), was adequate but should be improved in future versions of the questionnaire. A study of criterion validity was undertaken to test the questionnaire and to develop methods of testing the validity of measures of clinicians' Perspectives. However, the extraneous variables in this include the clinician's experience, usage of the newer drugs, etc. The two criteria used were the doctors' perspectives from clinical practice and the assessment of an external assessor and statistician. Clinicians were instructed to complete the questionnaire independently without consulting colleagues. Written informed consent was obtained from each participant before the study began.
2.4. Statistical Analysis
Data were analyzed using descriptive statistical methods. Categorical variables were summarized as frequencies and percentages to describe the distribution of responses. The relative proportion of each response category was calculated for all survey items. Graphical representations were generated to illustrate response patterns using Microsoft Excel (version 16.0.18025.20030).
3. Results
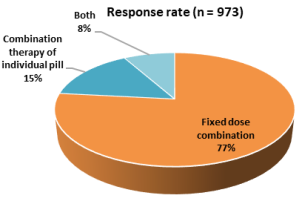
A total of 973 physicians participated in the primary analysis, while an additional subset of 93 physicians contributed to the extended analysis. The majority of respondents (44.91%) reported that 26–50% of their patients have essential (primary) hypertension. Half (50.05%) of clinicians indicated that secondary hypertension was present in 6–15% of patients. A large proportion of clinicians (76.67%) preferred fixed-dose combinations (FDCs) when two or more drugs are required for hypertension management (Figure 1). Approximately 44% of participants reported that FDCs were most commonly used in patients with uncontrolled hypertension.
Figure 1. Distribution of responses on the preferred requirement of two or more drugs for the management of hypertension.
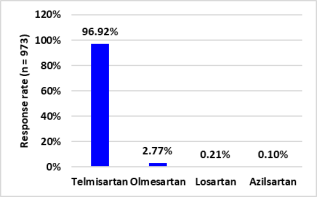
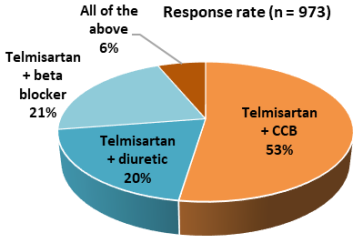
Approximately half (52.11%) of respondents indicated that 25–50% of patients with uncontrolled hypertension are on dual-drug FDCs. Approximately 52% of the clinicians reported that 11–20% of patients with uncontrolled hypertension were on triple-drug FDCs. Telmisartan is identified as the most commonly preferred angiotensin receptor blocker (ARB) by the majority (96.92%) of clinicians (Figure 2). Most of the participants (81.81%) opined that there were no adverse drug reactions with telmisartan. Around 48% of clinicians rated BP control with telmisartan as showing marked improvement. Approximately 52% of clinicians reported that telmisartan was most commonly preferred in combination with CCBs in patients with hypertension (Figure 3).
Figure 3. Distribution of responses on the commonly preferred combination therapy along with telmisartan in patients with hypertension.
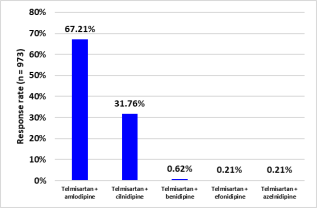
The most commonly preferred CCB in combination with telmisartan in young patients with uncontrolled hypertension was amlodipine, as reported by 67% of respondents (Figure 4). Almost half (50.15%) of participants reported that their preferred diuretic in combination with telmisartan in young patients with uncontrolled hypertension was chlorthalidone, while 46% reported preferring hydrochlorothiazide as the most commonly used diuretic (Table 1).
In patients with comorbid diabetes, around 55% of practitioners preferred the telmisartan + CCB combination therapy. As indicated by 57% of participants, the preferred beta-blocker in combination with telmisartan in patients with hypertension and coronary artery disease (CAD) is metoprolol (Table 2). About 62% of clinicians reported using the telmisartan + metoprolol combination in 11–25% of patients with uncontrolled hypertension.
Figure 4. Distribution of responses on the most commonly preferred calcium channel blocker, along with telmisartan, in young uncontrolled hypertensives.
Table 1. Distribution of responses on the preferred diuretic in combination with telmisartan in young uncontrolled hypertensives.
Diuretics
Response rate (n = 973)
Hydrochlorothiazide
46.45%
Chlorthalidone
50.15%
Indapamide
2.26%
All of the above
1.13%
Table 2. Distribution of responses on the preferred beta-blocker in combination with telmisartan in patients with hypertension and CAD.
Drugs
Response rate (n = 973)
Telmisartan + metoprolol
57.14%
Telmisartan + bisoprolol
39.88%
Telmisartan + carvedilol
1.34%
All of the above
1.64%
As reported by 49% of clinicians, telmisartan + CCB + beta-blocker was the most commonly preferred triple-drug combination (Table 3). Nearly 51% of participants reported that, in 11–20% of patients with uncontrolled hypertension, they prefer the telmisartan + metoprolol + chlorthalidone FDC. Approximately 58% of participants reported a preference for an FDC containing chlorthalidone at a dose of 12.5 mg. As indicated by 64% of respondents, telmisartan + CCB + beta-blocker was the preferred triple-drug combination in young patients with uncontrolled hypertension (Table 4). In elderly patients with uncontrolled hypertension, the preferred triple-drug combination was telmisartan + CCB + beta-blocker, as reported by 49% of experts, while 45% preferred telmisartan + CCB + diuretic.
Table 3. Distribution of responses on the most commonly used triple drug combination, along with telmisartan.
Drugs
Response rate (n = 973)
Telmisartan + CCB + diuretic
39.67%
Telmisartan + CCB + beta blocker
49.02%
Telmisartan + beta blocker + diuretic
9.97%
All of the above
1.34%
Table 4. Distribution of responses to the preferred triple drug combination in uncontrolled young hypertensive patients with CVD risk.
Drugs
Response rate (n = 973)
Telmisartan + CCB + diuretic
29.29%
Telmisartan + CCB + beta blocker
63.62%
CCB + beta blocker + diuretic
6.58%
All of the above
0.51%
Nearly 41% of experts noted that counselling was the most effective way to improve treatment and dietary adherence for achieving target BP. According to 49% of respondents, resistant hypertension was reported in 11–20% of patients.
The extended analysis involving a subset of 93 clinicians revealed the following findings. About 70% reported that 11–20% of patients experience BP variability. A majority (60.22%) of clinicians identified factors such as a sedentary lifestyle, stress, lack of awareness, and obesity as contributors to the increasing burden of hypertension in India.
Elderly patients with uncontrolled hypertension were considered the most challenging subgroup, as reported by 45% of clinicians. According to 37% of clinicians, a key limitation in current hypertension management was the lack of awareness. In patients with BP variability, 54% of respondents preferred home BP monitoring. Approximately 35% of clinicians reported recommending home BP monitoring in fewer than 10% of patients, while 33% reported recommending it in 21–30% of patients. Reduced pill burden is identified as the main advantage of FDCs by more than half (53.76%) of participants.
More than half (58.06%) of clinicians reported most frequently prescribing FDC therapy to middle-aged patients (35–50 years). Approximately 55% of respondents stated that patient compliance with regular medication was the most challenging aspect of hypertension management. Approximately 38% of clinicians reported that medication cost was a major factor associated with non-adherence, while 32% identified lack of patient education as the leading cause.
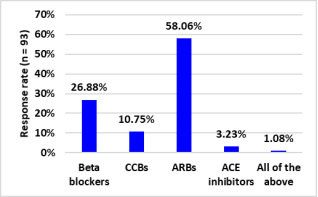
As reported by 38% of participants, mass education strategies were the preferred approach for educating patients with hypertension. More than half (58.06%) of clinicians indicated that ARBs were the most preferred first-line therapy in young patients with hypertension (Figure 5).
Figure 5. Distribution of responses on the parameters considered most important when choosing a brand in clinical practice.
As reported by 39% of clinicians, CCBs are the preferred first-line drug in elderly patients with hypertension. About 44% reported that the telmisartan + amlodipine FDC was most commonly used in 11–25% of patients, while 40% preferred its use in 23–50% of patients.
4. Discussion
The present large-scale, multicentric survey provides important insights into hypertension management practices among Indian clinicians, highlighting prevailing treatment patterns, therapeutic preferences, and key challenges in achieving optimal BP control. In the present study, a high preference for FDCs was observed, particularly when multiple drugs were required for effective hypertension management. This finding is consistent with existing evidence, which indicates that a majority of patients with hypertension require combination therapy to achieve optimal BP control.
Furthermore, FDCs have been associated with improved medication adherence compared to multiple-pill regimens, primarily due to reduced pill burden and simplified treatment schedules. Improved adherence with FDC therapy has, in turn, been linked to better clinical outcomes, including enhanced BP control and a reduction in cardiovascular events. In addition, the use of combination therapy involving agents with complementary mechanisms of action allows for more rapid and effective BP reduction while maintaining a favorable tolerability profile. Collectively, these factors likely contribute to the strong clinician preference for FDC-based strategies observed in the present study.
[12]
Verma AA, Khuu W, Tadrous M, Gomes T, Mamdani MM. Fixed-dose combination antihypertensive medications, adherence, and clinical outcomes: A population-based retrospective cohort study. PLoS Med. 2018; 15(6): e1002584.
Kawalec P, Holko P, Gawin M, Pilc A. Effectiveness of fixed-dose combination therapy in hypertension: systematic review and meta-analysis. Arch Med Sci. 2018; 14(5): 1125-1136.
da Silva PM. Efficacy of fixed-dose combination therapy in the treatment of patients with hypertension: focus on amlodipine/valsartan. Clin Drug Investig. 2010; 30(9): 625-641.
Telmisartan was identified as the most commonly preferred ARB by the majority of clinicians in the present survey, with a notable preference for its use in combination with CCBs. This pattern is consistent with existing literature. Chopda et al. reported that ARBs are the preferred class of antihypertensive agents among clinicians, with approximately 90.76% of experts indicating a preference for telmisartan for achieving sustained 24-hour BP control.
[16]
Chopda MB, Gadkar SG, Lakshmaiah YA, Lambata RK, Dabhade DC, Newale SR. Nationwide surveillance for Telmisartan alone or with combination at real world therapy in Indian patients with hypertension (START). International Journal of Research in Medical Sciences. 2021; 9(10): 3091-3094.
Similarly, Ramakrishnan et al. found that nearly 73% of clinicians in India selected telmisartan as the preferred first-line treatment for essential hypertension.
[17]
Ramakrishnan S, Ingole S, Dey A, Jain R. Management of Hypertension: Insights Into Prescribing Behavior with Focus on Angiotensin Receptor Blockers. Journal of the Practice of Cardiovascular Sciences. 2017; 3(1): 22.
The preference for telmisartan-based combination therapy observed in the present survey is further supported by clinical evidence. Segura and Ruilope demonstrated that the combination of telmisartan and amlodipine results in significantly greater BP reduction compared to either agent used as monotherapy, particularly in patients with moderate-to-severe hypertension.
[18]
Segura J, Ruilope LM. Clinical utility of fixed-combination telmisartan-amlodipine in the treatment of hypertension. Integr Blood Press Control. 2011; 4: 27-34.
In line with these findings, Sharma et al. also concluded that telmisartan combined with a CCB, such as amlodipine, is more effective than either drug alone in achieving optimal BP control.
[19]
Sharma AM, Bakris G, Neutel JM, Littlejohn TW, Kobe M, Ting N, et al. Single-pill combination of telmisartan/amlodipine versus amlodipine monotherapy in diabetic hypertensive patients: an 8-week randomized, parallel-group, double-blind trial. Clinical Therapeutics. 2012; 34(3): 537-551.
As per the findings of the current survey, the most commonly prescribed CCB in combination with telmisartan in young patients with uncontrolled hypertension was amlodipine. Similar findings have been reported by Dalal et al., who concluded that the combination of telmisartan and amlodipine is recommended as a preferred initial treatment for newly diagnosed Indian patients with hypertension, owing to its potential to achieve better BP control and improve cardiovascular outcomes.
[20]
Dalal J, Guha S, Reddy YVC, Ponde CK, Shrivastava S, Badani R, et al. Telmisartan plus amlodipine as the preferred initial combination in newly diagnosed Indian patients with hypertension: an expert consensus statement. J Assoc Physicians India. 2023; 71(12): 56-61.
Das et al. also reported that the telmisartan and amlodipine fixed-dose combination (FDC) is among the preferred single-pill combinations within the ARB + CCB class and is endorsed by major guidelines for the management of hypertension.
[21]
Das AK, Tiwaskar M, Abdullakutty J, Pande A, Kumar V, Zalte N, et al. Effectiveness and safety of the telmisartan and amlodipine fixed-dose combination in managing hypertension among Indian patients (TACT India study): rationale and study design. J Assoc Physicians India. 2024; 72(11): e16-e20.
In the present survey, a majority of young patients with uncontrolled hypertension were treated with a combination of telmisartan and a diuretic, with chlorthalidone emerging as the most preferred option. Supporting this observation, Sagarad et al. reported that patients who do not achieve target BP levels with telmisartan and hydrochlorothiazide may be effectively transitioned to a telmisartan and chlorthalidone combination, which has been shown to be both effective and well tolerated.
[22]
Sagarad SV, Kerure SB, Kumar S C, MR R. The Antihypertensive Efficacy of Chlorthalidone and Telmisartan in Indian Hypertensive Patients who were Uncontrolled with Hydrochlorothiazide and Telmisartan Combination-A Prospective and an Open Label Study. J Clin Diagn Res. 2013; 7(4): 687-690.
Furthermore, large-scale trials such as the ALLHAT study have established chlorthalidone as an effective agent for BP control and cardiovascular risk reduction.
[23]
Einhorn PT, Davis BR, Massie BM, Cushman WC, Piller LB, Simpson LM, et al.; ALLHAT Collaborative Research Group. The antihypertensive and lipid-lowering treatment to prevent heart attack trial (ALLHAT) heart failure validation study: diagnosis and prognosis. Am Heart J. 2007; 153(1): 42-53.
Ernst et al., in a comparative study, demonstrated that chlorthalidone has a longer half-life and provides more sustained 24-hour BP control, making it a more effective option for hypertension management.
[24]
Ernst ME, Carter BL, Goerdt CJ, Steffensmeier JJG, Phillips BB, Zimmerman MB, et al. Comparative antihypertensive effects of hydrochlorothiazide and chlorthalidone on ambulatory and office blood pressure. Hypertension. 2006; 47(3): 352-358.
The results of the current survey indicated that metoprolol was the preferred beta-blocker for use in combination with telmisartan in patients with hypertension and CAD. In line with this finding, a pan-Indian survey by Kathiresan et al. reported that telmisartan was preferred by 97% of physicians, while metoprolol was favored by 86%. Additionally, 91% of respondents preferred the combination of telmisartan and metoprolol, citing improvements in BP control, heart rate regulation, patient compliance, and overall adherence to therapy.
[25]
Kathiresan M, Saxena A, Tripathy P, Tripathi S, Upendra G. Management of hypertensive patients with ischemic heart disease and the role of a fixed-dose combination of telmisartan and metoprolol: a physician-based research survey. International Journal of Advances in Medicine. 2023; 10(5): 367-376.
A previous study by the present authors also reported a preference for the telmisartan and metoprolol combination in patients with hypertension and CAD.
[26]
Manjula S and Krishna Kumar M. Expert opinion on the prescription pattern of telmisartan and its combination for the management of Hypertension in the Indian setting. Int J Cardiol Res. 2024; 6(1): 24-29.
Furthermore, a multicenter phase III study by Sarkar et al., evaluating a FDC of telmisartan, metoprolol, and chlorthalidone, demonstrated significant BP reduction and good tolerability in patients with hypertension and stable coronary artery disease.
[27]
Sarkar G, Gaikwad VB, Sharma A, Halder SK, Kumar DA, Anand J, et al. Fixed-dose combination of metoprolol, telmisartan, and chlorthalidone for essential hypertension in adults with stable coronary artery disease: phase III study. Adv Ther. 2022; 39(2): 923-942.
As per the present survey findings, the most commonly preferred triple-drug combination was telmisartan, a CCB, and a beta-blocker. Additionally, a significant proportion of clinicians also favored a triple-drug combination consisting of telmisartan, a CCB, and a diuretic. Cho et al. reported that a phase III trial demonstrated that the standard-dose triple combination of telmisartan 80 mg, amlodipine 5 mg, and chlorthalidone 25 mg is both efficacious and safe for the treatment of primary hypertension.
[28]
Cho EJ, Kim MH, Kim YH, Chang K, Choi DJ, Kang WC, et al. Efficacy and safety of standard-dose triple combination of telmisartan 80 mg/amlodipine 5 mg/chlorthalidone 25 mg in primary hypertension: a randomized, double-blind, active-controlled, multicentre phase 3 trial. The Journal of Clinical Hypertension. 2023; 25(9): 817-827.
Some studies have also identified telmisartan as the most commonly prescribed ARB, with telmisartan + amlodipine + hydrochlorothiazide (i.e., ARB + CCB + diuretic) being the most frequently used triple combination in clinical practice.
[29]
Suman RK, Singh HK, Patil VG. Prescribing patterns of antihypertensive drugs in tertiary care teaching hospital. International Journal of Basic & Clinical Pharmacology. 2021; 10(4): 420-424.
Gupta A, Barman S, Roy D. Prescription Pattern of Anti-Hypertensive Medications In Patients with Hypertension at a Tertiary Care Hospital, Assam. Asian J Pharm Clin Res. 2024; 17(10): 85-89.
A similar cross-sectional survey conducted by the present authors reported that 63% of experts preferred the triple combination of telmisartan + CCB + beta-blocker for managing hypertension in young patients at risk of cardiovascular disease.
[26]
Manjula S and Krishna Kumar M. Expert opinion on the prescription pattern of telmisartan and its combination for the management of Hypertension in the Indian setting. Int J Cardiol Res. 2024; 6(1): 24-29.
Consistent with these findings, the present survey also reported that telmisartan + CCB + beta-blocker was the preferred triple-drug combination in young patients with uncontrolled hypertension.
The current survey noted that ARBs were the most preferred first-line therapy in young patients with hypertension. Consistent with this finding, Jadhav et al. reported that over 60% of respondents across various specialties preferred ARBs for treating hypertension in young adults.
[31]
Jadhav U, Tiwaskar M, Khan A, Kalmath BC, Ponde CK, Sawhney JP, et al. Hypertension in young adults in India: perspectives and therapeutic options amongst clinicians in a cross-sectional observational study. J Assoc Physicians India. 2021; 69(11): 11-12.
[31]
Similarly, Roy et al., in recent real-world evidence from India (CATCH-22 survey), demonstrated that ARBs were the most commonly prescribed initial antihypertensive agents, accounting for nearly half of first-line monotherapy prescriptions.
[32]
Roy D, Naik N, Kumar D, Mantoo MR, Banerjee PS, Srivastava P, et al. Cardinal aspects of treatment to control hypertension in India-2022 (CATCH 22): a survey on arterial hypertension management in young Indian adults: a report from Cardiology Society of India. Indian Heart Journal. 2026; 78(1): 25-31.
One of the key strengths of the present survey is its large clinician sample size, which enhances the representativeness of the findings across diverse clinical settings in India. However, as a questionnaire-based survey, the findings are based on self-reported responses and are therefore subject to recall and response bias. The results reflect clinicians’ perceptions of their treatment behavior rather than objectively verified prescription data or patient-level outcomes. Furthermore, the absence of direct clinical or follow-up data limits the ability to correlate these practices with actual effectiveness or safety outcomes. Regional variations in clinical practice were not specifically analyzed, which may affect the generalizability of the findings. Additionally, the supplementary analysis was conducted in a smaller subset of participants, which may limit the robustness of those observations. Further prospective, real-world studies are warranted to substantiate these observations.
5. Conclusions
The present survey demonstrates a clear preference among clinicians for telmisartan-based therapies and fixed-dose combinations in the management of hypertension. Combination regimens, particularly those involving CCBs and beta-blockers, are widely utilized, with ARBs emerging as the preferred first-line agents in younger patients. These findings provide valuable insights into contemporary hypertension management practices among Indian clinicians and highlight the importance of simplified treatment strategies for optimizing blood pressure control and improving adherence. Further real-world and prospective studies are warranted to evaluate the impact of these prescribing preferences on long-term clinical outcomes and cardiovascular risk reduction.
Kim HJ, Kim BS, Kim H, Lee J, Shin JH, Sung KC. Impact of blood pressure and medication adherence on clinical outcomes in patients with hypertension. Front Med (Lausanne). 2025; 12: 1564791.
Londoño Agudelo E, Pérez Ospina V, Battaglioli T, Taborda Pérez C, Gómez-Arias R, Van der Stuyft P. Gaps in hypertension care and control: a population-based study in low-income urban Medellin, Colombia. Trop Med Int Health. 2021; 26(8): 895-907.
Jafari EA. Fixed-dose combination antihypertensive therapy and healthcare utilization in U.S. adults with hypertension: a propensity score–based analysis of a nationally representative population. Front. Pharmacol. 17: 1787754.
Gosse P. A Review of Telmisartan in the Treatment of Hypertension: Blood Pressure Control in the Early Morning Hours. Vasc Health Risk Manag. 2006; 2(3): 195-201.
Kant S, Sharma A, Kumar V, Gore P, Pramanik S, Bhushan S, et al. A cross-sectional study on the drug utilization of fixed-dose combination of telmisartan plus metoprolol in patients with hypertension across various clinics in India. Hypertens Open Access. 2026; 3: 105.
Telmisartan. In: LiverTox: Clinical and Research Information on Drug-Induced Liver Injury. National Institute of Diabetes and Digestive and Kidney Diseases; 2012. Available from:
Kawalec P, Holko P, Gawin M, Pilc A. Effectiveness of fixed-dose combination therapy in hypertension: systematic review and meta-analysis. Arch Med Sci. 2018; 14(5): 1125-1136.
da Silva PM. Efficacy of fixed-dose combination therapy in the treatment of patients with hypertension: focus on amlodipine/valsartan. Clin Drug Investig. 2010; 30(9): 625-641.
Chopda MB, Gadkar SG, Lakshmaiah YA, Lambata RK, Dabhade DC, Newale SR. Nationwide surveillance for Telmisartan alone or with combination at real world therapy in Indian patients with hypertension (START). International Journal of Research in Medical Sciences. 2021; 9(10): 3091-3094.
Ramakrishnan S, Ingole S, Dey A, Jain R. Management of Hypertension: Insights Into Prescribing Behavior with Focus on Angiotensin Receptor Blockers. Journal of the Practice of Cardiovascular Sciences. 2017; 3(1): 22.
Dalal J, Guha S, Reddy YVC, Ponde CK, Shrivastava S, Badani R, et al. Telmisartan plus amlodipine as the preferred initial combination in newly diagnosed Indian patients with hypertension: an expert consensus statement. J Assoc Physicians India. 2023; 71(12): 56-61.
Das AK, Tiwaskar M, Abdullakutty J, Pande A, Kumar V, Zalte N, et al. Effectiveness and safety of the telmisartan and amlodipine fixed-dose combination in managing hypertension among Indian patients (TACT India study): rationale and study design. J Assoc Physicians India. 2024; 72(11): e16-e20.
Sagarad SV, Kerure SB, Kumar S C, MR R. The Antihypertensive Efficacy of Chlorthalidone and Telmisartan in Indian Hypertensive Patients who were Uncontrolled with Hydrochlorothiazide and Telmisartan Combination-A Prospective and an Open Label Study. J Clin Diagn Res. 2013; 7(4): 687-690.
Einhorn PT, Davis BR, Massie BM, Cushman WC, Piller LB, Simpson LM, et al.; ALLHAT Collaborative Research Group. The antihypertensive and lipid-lowering treatment to prevent heart attack trial (ALLHAT) heart failure validation study: diagnosis and prognosis. Am Heart J. 2007; 153(1): 42-53.
Ernst ME, Carter BL, Goerdt CJ, Steffensmeier JJG, Phillips BB, Zimmerman MB, et al. Comparative antihypertensive effects of hydrochlorothiazide and chlorthalidone on ambulatory and office blood pressure. Hypertension. 2006; 47(3): 352-358.
Kathiresan M, Saxena A, Tripathy P, Tripathi S, Upendra G. Management of hypertensive patients with ischemic heart disease and the role of a fixed-dose combination of telmisartan and metoprolol: a physician-based research survey. International Journal of Advances in Medicine. 2023; 10(5): 367-376.
Manjula S and Krishna Kumar M. Expert opinion on the prescription pattern of telmisartan and its combination for the management of Hypertension in the Indian setting. Int J Cardiol Res. 2024; 6(1): 24-29.
Sarkar G, Gaikwad VB, Sharma A, Halder SK, Kumar DA, Anand J, et al. Fixed-dose combination of metoprolol, telmisartan, and chlorthalidone for essential hypertension in adults with stable coronary artery disease: phase III study. Adv Ther. 2022; 39(2): 923-942.
Cho EJ, Kim MH, Kim YH, Chang K, Choi DJ, Kang WC, et al. Efficacy and safety of standard-dose triple combination of telmisartan 80 mg/amlodipine 5 mg/chlorthalidone 25 mg in primary hypertension: a randomized, double-blind, active-controlled, multicentre phase 3 trial. The Journal of Clinical Hypertension. 2023; 25(9): 817-827.
Gupta A, Barman S, Roy D. Prescription Pattern of Anti-Hypertensive Medications In Patients with Hypertension at a Tertiary Care Hospital, Assam. Asian J Pharm Clin Res. 2024; 17(10): 85-89.
Jadhav U, Tiwaskar M, Khan A, Kalmath BC, Ponde CK, Sawhney JP, et al. Hypertension in young adults in India: perspectives and therapeutic options amongst clinicians in a cross-sectional observational study. J Assoc Physicians India. 2021; 69(11): 11-12.
[32]
Roy D, Naik N, Kumar D, Mantoo MR, Banerjee PS, Srivastava P, et al. Cardinal aspects of treatment to control hypertension in India-2022 (CATCH 22): a survey on arterial hypertension management in young Indian adults: a report from Cardiology Society of India. Indian Heart Journal. 2026; 78(1): 25-31.
Suresh, M., Manjunath, K. K. (2026). Expert Perspectives and Preferences in the Management of Hypertension in Indian Settings: A Nationwide Survey. Cardiology and Cardiovascular Research, 10(2), 20-27. https://doi.org/10.11648/j.ccr.20261002.12
Suresh, M.; Manjunath, K. K. Expert Perspectives and Preferences in the Management of Hypertension in Indian Settings: A Nationwide Survey. Cardiol. Cardiovasc. Res.2026, 10(2), 20-27. doi: 10.11648/j.ccr.20261002.12
Suresh M, Manjunath KK. Expert Perspectives and Preferences in the Management of Hypertension in Indian Settings: A Nationwide Survey. Cardiol Cardiovasc Res. 2026;10(2):20-27. doi: 10.11648/j.ccr.20261002.12
@article{10.11648/j.ccr.20261002.12,
author = {Manjula Suresh and Krishna Kumar Manjunath},
title = {Expert Perspectives and Preferences in the Management of Hypertension in Indian Settings: A Nationwide Survey},
journal = {Cardiology and Cardiovascular Research},
volume = {10},
number = {2},
pages = {20-27},
doi = {10.11648/j.ccr.20261002.12},
url = {https://doi.org/10.11648/j.ccr.20261002.12},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ccr.20261002.12},
abstract = {Objective: To assess clinicians’ perspectives and preferences in hypertension management, with a focus on telmisartan-based therapies in Indian settings. Methodology: The cross-sectional study was conducted among 973 clinicians across India using a 23-item structured questionnaire, which collected information on treatment approaches, the use of fixed-dose combinations (FDCs), and treatment preferences. Additionally, an extended analysis comprising 15 supplementary questions was conducted with a subset of clinicians (n = 93) to further explore clinical practices in specific scenarios. The data were analyzed using descriptive statistics and presented as frequencies and percentages. Results: A large proportion of clinicians (76.67%) preferred FDCs when two or more drugs are required for hypertension management. Telmisartan was the most commonly preferred angiotensin receptor blocker (ARB), as reported by the majority (96.92%) of clinicians, with approximately 52% reporting its frequent use in combination with calcium channel blockers (CCBs). Among these, amlodipine is the most commonly preferred agent in young patients with uncontrolled hypertension, as reported by 67% of participants. Nearly half (50.15%) of respondents reported that chlorthalidone is the preferred diuretic in combination with telmisartan. About 57% of participants reported that metoprolol is the most commonly used beta-blocker in patients with hypertension and coronary artery disease. Telmisartan + CCB + beta-blocker is the most commonly preferred triple-drug combination, as indicated by 49% of participants, and 64% reported preferring this combination, particularly in young patients with uncontrolled hypertension. Conclusion: The survey findings highlight a strong preference for telmisartan-based therapies and FDCs among Indian clinicians, reflecting current clinical practices in hypertension management. The widespread use of ARBs, particularly in younger patients, underscores their perceived efficacy and tolerability.},
year = {2026}
}
TY - JOUR
T1 - Expert Perspectives and Preferences in the Management of Hypertension in Indian Settings: A Nationwide Survey
AU - Manjula Suresh
AU - Krishna Kumar Manjunath
Y1 - 2026/06/30
PY - 2026
N1 - https://doi.org/10.11648/j.ccr.20261002.12
DO - 10.11648/j.ccr.20261002.12
T2 - Cardiology and Cardiovascular Research
JF - Cardiology and Cardiovascular Research
JO - Cardiology and Cardiovascular Research
SP - 20
EP - 27
PB - Science Publishing Group
SN - 2578-8914
UR - https://doi.org/10.11648/j.ccr.20261002.12
AB - Objective: To assess clinicians’ perspectives and preferences in hypertension management, with a focus on telmisartan-based therapies in Indian settings. Methodology: The cross-sectional study was conducted among 973 clinicians across India using a 23-item structured questionnaire, which collected information on treatment approaches, the use of fixed-dose combinations (FDCs), and treatment preferences. Additionally, an extended analysis comprising 15 supplementary questions was conducted with a subset of clinicians (n = 93) to further explore clinical practices in specific scenarios. The data were analyzed using descriptive statistics and presented as frequencies and percentages. Results: A large proportion of clinicians (76.67%) preferred FDCs when two or more drugs are required for hypertension management. Telmisartan was the most commonly preferred angiotensin receptor blocker (ARB), as reported by the majority (96.92%) of clinicians, with approximately 52% reporting its frequent use in combination with calcium channel blockers (CCBs). Among these, amlodipine is the most commonly preferred agent in young patients with uncontrolled hypertension, as reported by 67% of participants. Nearly half (50.15%) of respondents reported that chlorthalidone is the preferred diuretic in combination with telmisartan. About 57% of participants reported that metoprolol is the most commonly used beta-blocker in patients with hypertension and coronary artery disease. Telmisartan + CCB + beta-blocker is the most commonly preferred triple-drug combination, as indicated by 49% of participants, and 64% reported preferring this combination, particularly in young patients with uncontrolled hypertension. Conclusion: The survey findings highlight a strong preference for telmisartan-based therapies and FDCs among Indian clinicians, reflecting current clinical practices in hypertension management. The widespread use of ARBs, particularly in younger patients, underscores their perceived efficacy and tolerability.
VL - 10
IS - 2
ER -
Suresh, M., Manjunath, K. K. (2026). Expert Perspectives and Preferences in the Management of Hypertension in Indian Settings: A Nationwide Survey. Cardiology and Cardiovascular Research, 10(2), 20-27. https://doi.org/10.11648/j.ccr.20261002.12
Suresh, M.; Manjunath, K. K. Expert Perspectives and Preferences in the Management of Hypertension in Indian Settings: A Nationwide Survey. Cardiol. Cardiovasc. Res.2026, 10(2), 20-27. doi: 10.11648/j.ccr.20261002.12
Suresh M, Manjunath KK. Expert Perspectives and Preferences in the Management of Hypertension in Indian Settings: A Nationwide Survey. Cardiol Cardiovasc Res. 2026;10(2):20-27. doi: 10.11648/j.ccr.20261002.12
@article{10.11648/j.ccr.20261002.12,
author = {Manjula Suresh and Krishna Kumar Manjunath},
title = {Expert Perspectives and Preferences in the Management of Hypertension in Indian Settings: A Nationwide Survey},
journal = {Cardiology and Cardiovascular Research},
volume = {10},
number = {2},
pages = {20-27},
doi = {10.11648/j.ccr.20261002.12},
url = {https://doi.org/10.11648/j.ccr.20261002.12},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ccr.20261002.12},
abstract = {Objective: To assess clinicians’ perspectives and preferences in hypertension management, with a focus on telmisartan-based therapies in Indian settings. Methodology: The cross-sectional study was conducted among 973 clinicians across India using a 23-item structured questionnaire, which collected information on treatment approaches, the use of fixed-dose combinations (FDCs), and treatment preferences. Additionally, an extended analysis comprising 15 supplementary questions was conducted with a subset of clinicians (n = 93) to further explore clinical practices in specific scenarios. The data were analyzed using descriptive statistics and presented as frequencies and percentages. Results: A large proportion of clinicians (76.67%) preferred FDCs when two or more drugs are required for hypertension management. Telmisartan was the most commonly preferred angiotensin receptor blocker (ARB), as reported by the majority (96.92%) of clinicians, with approximately 52% reporting its frequent use in combination with calcium channel blockers (CCBs). Among these, amlodipine is the most commonly preferred agent in young patients with uncontrolled hypertension, as reported by 67% of participants. Nearly half (50.15%) of respondents reported that chlorthalidone is the preferred diuretic in combination with telmisartan. About 57% of participants reported that metoprolol is the most commonly used beta-blocker in patients with hypertension and coronary artery disease. Telmisartan + CCB + beta-blocker is the most commonly preferred triple-drug combination, as indicated by 49% of participants, and 64% reported preferring this combination, particularly in young patients with uncontrolled hypertension. Conclusion: The survey findings highlight a strong preference for telmisartan-based therapies and FDCs among Indian clinicians, reflecting current clinical practices in hypertension management. The widespread use of ARBs, particularly in younger patients, underscores their perceived efficacy and tolerability.},
year = {2026}
}
TY - JOUR
T1 - Expert Perspectives and Preferences in the Management of Hypertension in Indian Settings: A Nationwide Survey
AU - Manjula Suresh
AU - Krishna Kumar Manjunath
Y1 - 2026/06/30
PY - 2026
N1 - https://doi.org/10.11648/j.ccr.20261002.12
DO - 10.11648/j.ccr.20261002.12
T2 - Cardiology and Cardiovascular Research
JF - Cardiology and Cardiovascular Research
JO - Cardiology and Cardiovascular Research
SP - 20
EP - 27
PB - Science Publishing Group
SN - 2578-8914
UR - https://doi.org/10.11648/j.ccr.20261002.12
AB - Objective: To assess clinicians’ perspectives and preferences in hypertension management, with a focus on telmisartan-based therapies in Indian settings. Methodology: The cross-sectional study was conducted among 973 clinicians across India using a 23-item structured questionnaire, which collected information on treatment approaches, the use of fixed-dose combinations (FDCs), and treatment preferences. Additionally, an extended analysis comprising 15 supplementary questions was conducted with a subset of clinicians (n = 93) to further explore clinical practices in specific scenarios. The data were analyzed using descriptive statistics and presented as frequencies and percentages. Results: A large proportion of clinicians (76.67%) preferred FDCs when two or more drugs are required for hypertension management. Telmisartan was the most commonly preferred angiotensin receptor blocker (ARB), as reported by the majority (96.92%) of clinicians, with approximately 52% reporting its frequent use in combination with calcium channel blockers (CCBs). Among these, amlodipine is the most commonly preferred agent in young patients with uncontrolled hypertension, as reported by 67% of participants. Nearly half (50.15%) of respondents reported that chlorthalidone is the preferred diuretic in combination with telmisartan. About 57% of participants reported that metoprolol is the most commonly used beta-blocker in patients with hypertension and coronary artery disease. Telmisartan + CCB + beta-blocker is the most commonly preferred triple-drug combination, as indicated by 49% of participants, and 64% reported preferring this combination, particularly in young patients with uncontrolled hypertension. Conclusion: The survey findings highlight a strong preference for telmisartan-based therapies and FDCs among Indian clinicians, reflecting current clinical practices in hypertension management. The widespread use of ARBs, particularly in younger patients, underscores their perceived efficacy and tolerability.
VL - 10
IS - 2
ER -