Previous studies on the correlation between serum apolipoprotein A-I (apoA-I) and the severity of heart failure (HF) as well as short-term clinical outcomes in patients with heart failure due to non-ischemic cardiomyopathy (NICM) have been inconclusive. To address this, we aimed to determine the impact of apoA-I on the severity of heart failure and short-term clinical outcomes in patients with HF due to NICM. In this single-center, observational study, we recruited 154 patients with NICM heart failure (NYHA functional class II-IV) and 80 control patients with normal cardiac function. Baseline characteristics were collected during hospitalization, and follow-up records were obtained 6 months after discharge. Statistical analyses included Pearson’s chi-squared test and Spearman's correlation analysis, while the receiver operating characteristic (ROC) curve was used to discriminate patients with severe heart failure. Results showed that serum apoA-I levels were significantly lower in the heart failure group compared to controls and decreased with increasing cardiac function class. Additionally, serum apoA-I was positively correlated with left ventricular ejection fraction (LVEF) and negatively correlated with B-type natriuretic peptide (BNP) and cardiac function class. Patients who experienced clinical events within 6 months of discharge had significantly lower apoA-I concentrations compared to those without events. In conclusion, low serum apoA-I concentrations in patients with NICM and heart failure may be associated with more severe heart failure and a higher probability of recurrent clinical events in the short term.
| Published in | Cardiology and Cardiovascular Research (Volume 9, Issue 1) |
| DOI | 10.11648/j.ccr.20250901.12 |
| Page(s) | 25-31 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2025. Published by Science Publishing Group |
Heart Failure, Apolipoprotein A-I, Heart Rate, Cardiac Function, Clinical Outcome
Cardiac Function Classification (NYHA) | |||||
|---|---|---|---|---|---|
control (N=80) | Grade II (N=18) | Grade III (N=49) | Grade IV (N=87) | P value | |
Age | 60.31±8.75 | 63.67±12.12 | 64.33±9.96 | 63.52±11.86 | >0.05 |
Male (%) | 41(51.25%) | 10(55.56%) | 34(69.39%) | 64(73.56%) | >0.05 |
BMI | 23.79±2.51 | 23.95±3.09 | 24.36±3.36 | 23.82±4.35 | >0.05 |
Diabetes (%) | 7(8.75%) | 2(11.11%) | 9(18.37%) | 14(16.09%) | >0.05 |
AF (%) | 3(3.75%) | 2(11.11%) | 18(36.73%) | 28(32.18%) | >0.05 |
Smoking (%) | 18(22.50%) | 8(44.44%) | 14(28.57%) | 29(33.33%) | >0.05 |
SP (mmHg) | 124.89±14.81 | 138.72±32.16 | 125.76±24.12 | 118.48±21.52 | >0.05 |
DP (mmHg) | 77.75±8.47 | 83.72±20.55 | 76.00±14.73 | 74.66±13.95 | >0.05 |
HR (bpm) | 73.63±10.67 | 76.56±13.29 | 79.61±24.48 | 85.45±19.67 | <0.05 |
Etiology | |||||
Dilated cardiomyopathy (%) | 11 (61.11%) | 22 (44.90%) | 58 (66.67%) | ||
Hypertension (%) | 4 (22.22%) | 22 (44.90%) | 17 (19.54%) | >0.05 | |
Heart Valve (%) | 3 (16.67%) | 5 (10.20%) | 12 (13.79%) | ||
TC (mmol/L) | 4.42±0.73 | 4.23±0.75 | 3.85±1.22 | 3.72±1.03 | >0.05 |
TG (mmol/L) | 1.59±0.88 | 1.40±0.69 | 1.32±0.95 | 1.08±0.58 | >0.05 |
LDL-C (mmol/L) | 2.63±0.64 | 2.59±0.61 | 2.28±0.84 | 2.33±0.84 | >0.05 |
HDL-C (mmol/L) | 1.17±0.27 | 1.05±0.20 | 1.03±0.37 | 0.95±0.30 | >0.05 |
ApoAI (g/L) | 1.32±0.27 | 1.21±0.15 | 1.15±0.23 | 1.02±0.19 | <0.05 |
ApoB (g/L) | 0.89±0.19 | 0.88±0.17 | 0.85±0.22 | 0.84±0.28 | >0.05 |
LP(a) (mg/L) | 171.51±196.79 | 149.19±123.91 | 107.52±82.11 | 155.56±228.75 | >0.05 |
ApoAI/ApoB | 1.56±0.39 | 1.44±0.41 | 1.43±0.38 | 1.35±0.38 | >0.05 |
Cr (umol/L) | 63.38±13.25 | 81.35±17.35 | 85.55±28.32 | 96.22±39.43 | >0.05 |
CrCl (ml/min) | 97.26±22.58 | 75.75±23.98 | 71.57±30.58 | 69.74±31.15 | >0.05 |
BNP (pg/ml) | 50.12±30.99 | 1741.37±1509.41 | 3079.44±2626.87 | 7401.92±7671.88 | <0.05 |
LVEF (%) | 66.39±51.21 | 43.22±15.20 | 39.33±17.95 | 31.94±12.10 | <0.05 |
HsCRP (mg/L) | 1.78±2.07 | 4.73±3.92 | 4.93±4.90 | 6.19±5.15 | >0.05 |
Grade II (N=18) | Grade III (N=49) | Grade IV (N=87) | |
|---|---|---|---|
Re-hospitalization due to worsening heart failure symptoms | 1 (5.56%) | 4 (8.16%) | 12 (13.79%) |
Death | |||
pump Failure | 0 (0.00%) | 0 (0.00%) | 2 (2.30%) |
sudden death | 0 (0.00%) | 0 (0.00%) | 1 (1.15%) |
other causes | 0 (0.00%) | 0 (0.00%) | 1 (1.15%) |
HF | Heart Failure |
NICM | Non-ischemic Cardiomyopathy |
NYHA | New York Heart Association |
LVEF | Left Ventricular Ejection Fraction |
BNP | B-type Natriuretic Peptide |
HDL-C | High-Density Lipoprotein Cholesterol |
apoA-I | Apolipoprotein A-I |
apoB | Apolipoprotein B |
LP(a) | Lipoprotein A |
Cr | Creatinine |
CrCl | Creatinine Clearance |
Hs-CRP | Hypersensitive C-Reactive Protein |
TC | Total Cholesterol |
TG | Triglyceride |
LDL-C | Low-Density Lipoprotein Cholesterol |
ROC | Receiver Operating Characteristic |
AUC | Area Under the Curve |
ESC | European Society of Cardiology |
LCAT | Lecithin-Cholesterol Acyltransferase |
AF | Atrial Fibrillation |
SP | Systolic Pressure |
DP | Diastolic Pressure |
HR | Heart Rate |
| [1] | Petrie MC, Verma S, Docherty KF, Inzucchi SE, Anand I, Belohlavek J, Bohm M, Chiang CE, Chopra VK, de Boer RA et al: Effect of Dapagliflozin on Worsening Heart Failure and Cardiovascular Death in Patients With Heart Failure With and Without Diabetes. JAMA 2020, 323(14): 1353-1368. |
| [2] |
Yin J, Lu X, Qian Z, Xu W, Zhou X: New insights into the pathogenesis and treatment of sarcopenia in chronic heart failure. Theranostics 2019, 9(14): 4019-4029.
https://doi.org/10.7150/thno.33000 eCollection 2019. |
| [3] | Pinsky MR: The right ventricle: interaction with the pulmonary circulation. Crit Care 2016, 20: 266. |
| [4] | Kraigher-Krainer E, Shah AM, Gupta DK, Santos A, Claggett B, Pieske B, Zile MR, Voors AA, Lefkowitz MP, Packer M et al: Impaired systolic function by strain imaging in heart failure with preserved ejection fraction. J Am Coll Cardiol 2014, 63(5): 447-456. |
| [5] |
Aaron CP, Hoffman EA, Lima JAC, Kawut SM, Bertoni AG, Vogel-Claussen J, Habibi M, Hueper K, Jacobs DR, Jr., Kalhan R et al: Pulmonary vascular volume, impaired left ventricular filling and dyspnea: The MESA Lung Study. PLoS One 2017, 12(4): e0176180.
https://doi.org/10.1371/journal.pone.0176180 eCollection 2017. |
| [6] | Liu L, Eisen HJ: Epidemiology of heart failure and scope of the problem. Cardiol Clin 2014, 32(1): 1-8, vii. |
| [7] | Wong CM, Hawkins NM, Petrie MC, Jhund PS, Gardner RS, Ariti CA, Poppe KK, Earle N, Whalley GA, Squire IB et al: Heart failure in younger patients: the Meta-analysis Global Group in Chronic Heart Failure (MAGGIC). Eur Heart J 2014, 35(39): 2714-2721. |
| [8] | Segrest JP, Li L, Anantharamaiah GM, Harvey SC, Liadaki KN, Zannis V: Structure and function of apolipoprotein A-I and high-density lipoprotein. Curr Opin Lipidol 2000, 11(2): 105-115. |
| [9] | Melchior JT, Street SE, Vaisar T, Hart R, Jerome J, Kuklenyik Z, Clouet-Foraison N, Thornock C, Bedi S, Shah AS et al: Apolipoprotein A-I modulates HDL particle size in the absence of apolipoprotein A-II. J Lipid Res 2021, 62: 100099. |
| [10] | De Oliveira e Silva ER, Kong M, Han Z, Starr C, Kass EM, Juo SH, Foster D, Dansky HM, Merkel M, Cundey K et al: Metabolic and genetic determinants of HDL metabolism and hepatic lipase activity in normolipidemic females. J Lipid Res 1999, 40(7): 1211-1221. |
| [11] | Pussinen PJ, Jauhiainen M, Ehnholm C: ApoA-II/apoA-I molar ratio in the HDL particle influences phospholipid transfer protein-mediated HDL interconversion. J Lipid Res 1997, 38(1): 12-21. |
| [12] | Millar JS, Cuchel M: ApoA-I-Directed Therapies for the Management of Atherosclerosis. Curr Atheroscler Rep 2015, 17(10): 60. |
| [13] | Walldius G, Jungner I, Aastveit AH, Holme I, Furberg CD, Sniderman AD: The apoB/apoA-I ratio is better than the cholesterol ratios to estimate the balance between plasma proatherogenic and antiatherogenic lipoproteins and to predict coronary risk. Clin Chem Lab Med 2004, 42(12): 1355-1363. |
| [14] | Fernandez ML, Webb D: The LDL to HDL cholesterol ratio as a valuable tool to evaluate coronary heart disease risk. J Am Coll Nutr 2008, 27(1): 1-5. |
| [15] | Srinivasan SR, Berenson GS: Serum apolipoproteins A-I and B as markers of coronary artery disease risk in early life: the Bogalusa Heart Study. Clin Chem 1995, 41(1): 159-164. |
| [16] | Rubenfire M, Brook RD: HDL cholesterol and cardiovascular outcomes: what is the evidence? Curr Cardiol Rep 2013, 15(4): 349. |
| [17] | Barter P: HDL-C: role as a risk modifier. Atheroscler Suppl 2011, 12(3): 267-270. |
| [18] | Van Lenten BJ, Hama SY, de Beer FC, Stafforini DM, McIntyre TM, Prescott SM, La Du BN, Fogelman AM, Navab M: Anti-inflammatory HDL becomes pro-inflammatory during the acute phase response. Loss of protective effect of HDL against LDL oxidation in aortic wall cell cocultures. J Clin Invest 1995, 96(6): 2758-2767. |
| [19] | Zhang Y, Zanotti I, Reilly MP, Glick JM, Rothblat GH, Rader DJ: Overexpression of apolipoprotein A-I promotes reverse transport of cholesterol from macrophages to feces in vivo. Circulation 2003, 108(6): 661-663. |
| [20] | Georgila K, Vyrla D, Drakos E: Apolipoprotein A-I (ApoA-I), Immunity, Inflammation and Cancer. Cancers (Basel) 2019, 11(8). |
| [21] | Chiesa G, Sirtori CR: Recombinant apolipoprotein A-I (Milano): a novel agent for the induction of regression of atherosclerotic plaques. Ann Med 2003, 35(4): 267-273. |
| [22] | Karjalainen MK, Holmes MV, Wang Q, Anufrieva O, Kahonen M, Lehtimaki T, Havulinna AS, Kristiansson K, Salomaa V, Perola M et al: Apolipoprotein A-I concentrations and risk of coronary artery disease: A Mendelian randomization study. Atherosclerosis 2020, 299: 56-63. |
| [23] | Banos-Gonzalez MA, Pena-Duque MA, Angles-Cano E, Martinez-Rios MA, Bahena A, Valente-Acosta B, Cardoso-Saldana G, Angulo-Ortiz J, de la Pena-Diaz A: Apo(a) phenotyping and long-term prognosis for coronary artery disease. Clin Biochem 2010, 43(7-8): 640-644. |
| [24] |
Sun L, Guo M, Xu C, Qiao X, Hua Y, Tuerhongjiang G, Lou B, Li R, Bai X, Zhou J et al: HDL-C/apoA-I Ratio Is Associated with the Severity of Coronary Artery Stenosis in Diabetic Patients with Acute Coronary Syndrome. Dis Markers 2021, 2021: 6689056.
https://doi.org/10.1155/2021/6689056 eCollection 2021. |
| [25] |
Voigt A, Rahnefeld A, Kloetzel PM, Kruger E: Cytokine-induced oxidative stress in cardiac inflammation and heart failure-how the ubiquitin proteasome system targets this vicious cycle. Front Physiol 2013, 4: 42.
https://doi.org/10.3389/fphys.2013.00042 . eCollection 2013. |
| [26] | Ayoub KF, Pothineni NVK, Rutland J, Ding Z, Mehta JL: Immunity, Inflammation, and Oxidative Stress in Heart Failure: Emerging Molecular Targets. Cardiovasc Drugs Ther 2017, 31(5-6): 593-608. |
APA Style
Ma, C., Chen, L., Sun, S., Qian, X., Qin, Y. (2025). Correlation Between Serum Apolipoprotein A and Clinical Outcome in Patients with Non-ischemic Heart Failure. Cardiology and Cardiovascular Research, 9(1), 25-31. https://doi.org/10.11648/j.ccr.20250901.12
ACS Style
Ma, C.; Chen, L.; Sun, S.; Qian, X.; Qin, Y. Correlation Between Serum Apolipoprotein A and Clinical Outcome in Patients with Non-ischemic Heart Failure. Cardiol. Cardiovasc. Res. 2025, 9(1), 25-31. doi: 10.11648/j.ccr.20250901.12
@article{10.11648/j.ccr.20250901.12,
author = {Chiqian Ma and Licong Chen and Shikun Sun and Xiaodong Qian and Yiren Qin},
title = {Correlation Between Serum Apolipoprotein A and Clinical Outcome in Patients with Non-ischemic Heart Failure},
journal = {Cardiology and Cardiovascular Research},
volume = {9},
number = {1},
pages = {25-31},
doi = {10.11648/j.ccr.20250901.12},
url = {https://doi.org/10.11648/j.ccr.20250901.12},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ccr.20250901.12},
abstract = {Previous studies on the correlation between serum apolipoprotein A-I (apoA-I) and the severity of heart failure (HF) as well as short-term clinical outcomes in patients with heart failure due to non-ischemic cardiomyopathy (NICM) have been inconclusive. To address this, we aimed to determine the impact of apoA-I on the severity of heart failure and short-term clinical outcomes in patients with HF due to NICM. In this single-center, observational study, we recruited 154 patients with NICM heart failure (NYHA functional class II-IV) and 80 control patients with normal cardiac function. Baseline characteristics were collected during hospitalization, and follow-up records were obtained 6 months after discharge. Statistical analyses included Pearson’s chi-squared test and Spearman's correlation analysis, while the receiver operating characteristic (ROC) curve was used to discriminate patients with severe heart failure. Results showed that serum apoA-I levels were significantly lower in the heart failure group compared to controls and decreased with increasing cardiac function class. Additionally, serum apoA-I was positively correlated with left ventricular ejection fraction (LVEF) and negatively correlated with B-type natriuretic peptide (BNP) and cardiac function class. Patients who experienced clinical events within 6 months of discharge had significantly lower apoA-I concentrations compared to those without events. In conclusion, low serum apoA-I concentrations in patients with NICM and heart failure may be associated with more severe heart failure and a higher probability of recurrent clinical events in the short term.},
year = {2025}
}
TY - JOUR T1 - Correlation Between Serum Apolipoprotein A and Clinical Outcome in Patients with Non-ischemic Heart Failure AU - Chiqian Ma AU - Licong Chen AU - Shikun Sun AU - Xiaodong Qian AU - Yiren Qin Y1 - 2025/02/10 PY - 2025 N1 - https://doi.org/10.11648/j.ccr.20250901.12 DO - 10.11648/j.ccr.20250901.12 T2 - Cardiology and Cardiovascular Research JF - Cardiology and Cardiovascular Research JO - Cardiology and Cardiovascular Research SP - 25 EP - 31 PB - Science Publishing Group SN - 2578-8914 UR - https://doi.org/10.11648/j.ccr.20250901.12 AB - Previous studies on the correlation between serum apolipoprotein A-I (apoA-I) and the severity of heart failure (HF) as well as short-term clinical outcomes in patients with heart failure due to non-ischemic cardiomyopathy (NICM) have been inconclusive. To address this, we aimed to determine the impact of apoA-I on the severity of heart failure and short-term clinical outcomes in patients with HF due to NICM. In this single-center, observational study, we recruited 154 patients with NICM heart failure (NYHA functional class II-IV) and 80 control patients with normal cardiac function. Baseline characteristics were collected during hospitalization, and follow-up records were obtained 6 months after discharge. Statistical analyses included Pearson’s chi-squared test and Spearman's correlation analysis, while the receiver operating characteristic (ROC) curve was used to discriminate patients with severe heart failure. Results showed that serum apoA-I levels were significantly lower in the heart failure group compared to controls and decreased with increasing cardiac function class. Additionally, serum apoA-I was positively correlated with left ventricular ejection fraction (LVEF) and negatively correlated with B-type natriuretic peptide (BNP) and cardiac function class. Patients who experienced clinical events within 6 months of discharge had significantly lower apoA-I concentrations compared to those without events. In conclusion, low serum apoA-I concentrations in patients with NICM and heart failure may be associated with more severe heart failure and a higher probability of recurrent clinical events in the short term. VL - 9 IS - 1 ER -
The Department of Cardiology, The First Affiliated Hospital of Soochow University, Soochow University, Suzhou, China
The Department of Neurology, The First Affiliated Hospital of Soochow University, Soochow University, Suzhou, China
The Department of Cardiology, The First Affiliated Hospital of Soochow University, Soochow University, Suzhou, China
The Department of Cardiology, The First Affiliated Hospital of Soochow University, Soochow University, Suzhou, China
The Department of Neurology, The First Affiliated Hospital of Soochow University, Soochow University, Suzhou, China
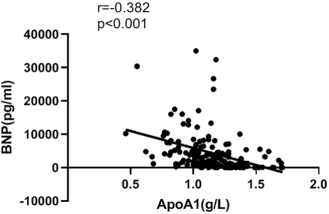
Figure 1. Correlation analysis of serum apoA-I concentration with BNP.
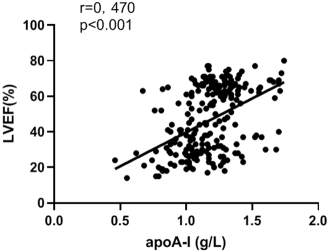
Figure 2. Correlation analysis of serum apoA-I concentration with LVEF value.
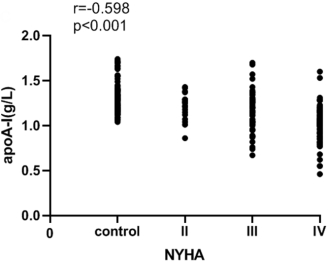
Figure 3. Correlation analysis of serum apoA-I concentration with cardiac function classification.
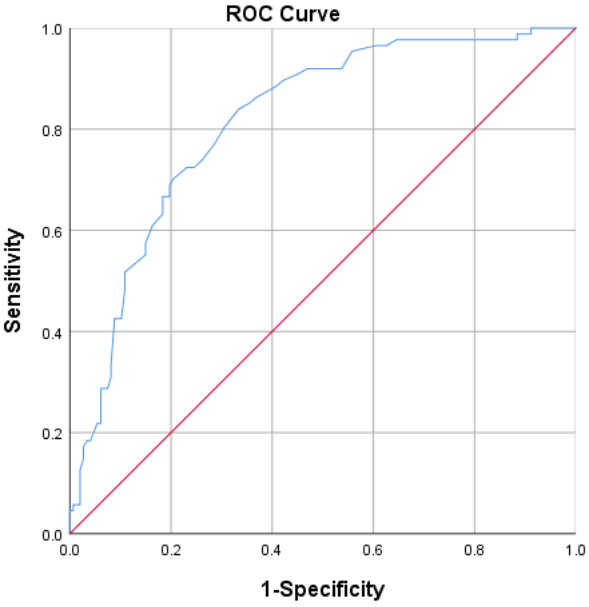
Figure 4. ROC curve of serum apoA-I concentration to evaluate the severity of heart failure.
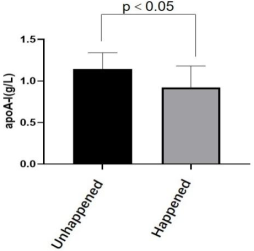
Figure 5. Comparison of apoA-I levels in patients without and with clinical events.
Information

