Introduction: Infertility is defined as the inability of a couple to achieve a clinical pregnancy after at least twelve months of regular, unprotected sexual intercourse. It is a major reproductive health problem worldwide, affecting approximately 80 million people. In Senegal, infertility represents a significant health and social concern due to its prevalence, its psychosocial repercussions, and the burden of suffering it inflicts on affected couples. The objective of the study was to evaluate the psychological experience of infertility among women in couples. Materials and Methods: This is a prospective, cross-sectional and descriptive study carried out over the period from October 11, 2021 to October 17, 2022 at the maternity ward of the National Hospital Center “Dalal Jamm” in Dakar. This included women in a relationship for one year who were consulted for pregnancy and those followed for infertility. Data was collected by direct interview, entered into the KOBO application, processed and analyzed using Excel and SPSS software. Results: Out of a total of 100 women surveyed, the average age was 34 years. The age group of [30-37 years] was the most represented. The secondary education level was the most represented 31%. The liberal profession was 37%, Muslim women 95% and those in their first marriage 85%. Women had been cohabiting with their partner for more than 5 years in 54% of cases. Primary infertility was 61%. The spouse participated in the explorations in 68.8% of cases. Infertility was of female origin in 51% of cases. When the diagnosis was announced, women felt hopeless in 29.6% of cases. Chronic psychological manifestations such as anxiety (82%), depression (73%), self-defense mechanisms such as isolation (62%), affiliation (20%) and intellectualization (13%) were not noted in the patients. The types of help expressed by patients were medical (68%), financial (37%), spiritual (23%), and psychological (20%). Conclusion: Infertility is not only a reproductive health issue, but also a mental health problem due to the psychological suffering it causes. Psychological and medical care (PMA) would allow women to reduce psychological suffering and increase the chances of pregnancy.
| Published in | American Journal of Psychiatry and Neuroscience (Volume 14, Issue 2) |
| DOI | 10.11648/j.ajpn.20261402.11 |
| Page(s) | 30-40 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2026. Published by Science Publishing Group |
Infertility of the Couple, Woman, Psychological Experience, Senegal
Age (year) | Workforce | Percentage (%) |
|---|---|---|
≤ 30 | 34 | 34 |
[30- 37] | 37 | 37 |
[37 - 40] | 14 | 14 |
> 40 | 15 | 15 |
Total | 100 | 100 |
Educational level | Workforce | Percentage (%) |
|---|---|---|
Unschooled | 13 | 13 |
Primary | 28 | 28 |
Secondary | 31 | 31 |
High | 28 | 28 |
Total | 100 | 100 |
Profession | Workforce | Percentage (%) |
|---|---|---|
Private employee | 7 | 7 |
Public employee | 13 | 13 |
Without profession | 31 | 31 |
Liberal profession | 37 | 37 |
Others | 12 | 12 |
Total | 100 | 100 |
Consultation deadline | Workforce | Percentage (%) |
|---|---|---|
One years | 36 | 36 |
Two years | 25 | 25 |
Three years | 11 | 11 |
Four years | 2 | 2 |
Five years | 8 | 8 |
Five years and over | 18 | 18 |
Total | 100 | 100 |
Raisons | Workforce | Percentage (%) |
|---|---|---|
No prescribed assessment | 13 | 45 |
Already a father | 7 | 24,1 |
Unknown reason | 6 | 20,7 |
Pregnant second wife | 1 | 3,4 |
No belief in modern medicine | 1 | 3,4 |
Lack of resources | 1 | 3,4 |
Total | 29 | 100 |
Reasons | Workforce | Percentage (%) |
|---|---|---|
Lack of expected results | 22 | 48,9 |
Discouragement | 7 | 15,6 |
Changing gynecologist | 6 | 13,6 |
Difficulty getting an appointment with the gynecologist | 4 | 8,9 |
Lack of resources | 2 | 4,4 |
Fear of surgery | 2 | 4,4 |
Spouse’s non-participation | 2 | 4,4 |
The husband's discomfort | 1 | 2,2 |
Covid 19wsz »a | 1 | 2,2 |
Travel | 1 | 2,2 |
Procedures | Workforce | Percentage (%) |
|---|---|---|
Continuity of care | 96 | 96 |
Medical Assistance for Reproduction | 9 | 9 |
Adoption of a child | 2 | 2 |
Consultation with other specialists | 2 | 2 |
Renunciation of the child project | 2 | 2 |
Low-calorie diet | 1 | 1 |
Reaction to the announcement of infertility | Workforce | Percentage (%) |
|---|---|---|
Despair | 21 | 29,6 |
The frustration | 17 | 23,9 |
The feeling of helplessness | 17 | 23,9 |
The pain | 15 | 21,1 |
Sadness | 10 | 14,1 |
Anger | 5 | 7 |
Denial | 4 | 5,6 |
Jealousy | 3 | 4,2 |
Guilt | 3 | 4,2 |
The injustice | 3 | 4,2 |
Loss of confidence | 3 | 4,2 |
Violation of his rights | 1 | 1,4 |
Demonstrations | Workforce | Percentage (%) |
|---|---|---|
Anxiety | 82 | 82 |
Depression | 73 | 73 |
Insomnia | 52 | 52 |
Bipolar disorder | 32 | 32 |
Lower self-esteem | 22 | 22 |
Presence of perverse desires | 18 | 18 |
Decreased libido | 15 | 15 |
No demonstration | 8 | 8 |
Self-defense reactions | Workforce | Percentage (%) |
|---|---|---|
Insulation or isolation | 62 | 62 |
Affiliation | 20 | 20 |
Intellectualization | 13 | 13 |
Sublimation | 12 | 12 |
Repression | 8 | 8 |
Altruism | 8 | 8 |
Denial | 6 | 6 |
Medication | 1 | 1 |
Help desired | Workforce | Percentage (%) |
|---|---|---|
Medical help | 68 | 68 |
Financial aid | 37 | 37 |
Spiritual help | 23 | 23 |
Psychological help | 20 | 20 |
Others | 2 | 2 |
PMA | Psychological and Medical Care |
CHNDJ | Dalal Jamm National Hospital Center |
CHNP | Pikine National Hospital Center |
IVF | In Vitro Fertilization |
WHO | World Health Organization |
DRC | Democratic Republic of the Congo |
HIV | Human Immunodeficiency Virus |
ART | Assisted Reproductive Technology |
| [1] | Girard DE, Galani DV, Toma S. « Détresse psychologique des couples infertiles : une approche globale ». ["Psychological distress in infertile couples: a comprehensive approach."] Rev Med Suisse 2017; 13(549): 371-374. |
| [2] | Brzakowski M, Lourdel E, Cabry R, Olieric MF, Claeys C, Devaux A, et al. « Epidémiologie du couple infertile ». [Epidemiology of infertile couples.] J Gynécol Obstet Biol Reprod 2009; 38: F3-F7. |
| [3] | Brochard M. Reproductive norms, infertility and new technologies of reproduction in Senegal. Université Paris Descartes, Thèse Méd., Paris, 2014. |
| [4] | Diop A. « Profil hystérosalpingographique de l’infertilité féminine au centre hospitalier national de pikine » [Hysterosalpingographic profile of female infertility at the Pikine National Hospital Center] Ucad, Thèse Méd., Dakar, 2013, n°772, 104p. |
| [5] | Dia F. « Assistance médicale à la procréation : bilan d’activités de FIV-Sénégal de 2007-2017 » [Assisted reproductive technology: activity report of IVF-Senegal from 2007-2017]. Ucad, Thèse Méd., Dakar, 2018, n°192, 116p. |
| [6] | Dieng ML. « Évaluation psychométrique du stress lie à l’infertilité dans un échantillon de patients au Sénégal » [Psychometric assessment of infertility-related stress in a sample of patients in Senegal]. Ucad, Thèse Méd., Dakar, 2019; n° 266, 96 p. |
| [7] | Faye AB. « Apport de l’échographie 2D dans l’exploration de l’infertilité féminine au CHN de Pikine ». [The contribution of 2D ultrasound in the investigation of female infertility at the Pikine National Hospital Center. Psychometric evaluation of stress related to infertility in a sample of patients in Senegal.] Ucad, Thèse Méd., Dakar, 2019, n°96, 149p. |
| [8] | Priso EB, Nguefack CT, Nguemgne C, Njamen TN, Taila W, Banag E. « L’infertilité féminine a l’Hôpital Général de Douala : aspects épidémiologiques et radiologiques (à propos de 658 cas) ». [Female infertility at Douala General Hospital: epidemiological and radiological aspects (based on 658 cases)] J Afr Imag Méd. 2015; 7. |
| [9] | Wembulua Shinga B. « Infertilité du couple. Étude épidémio-clinique et évaluation de la prise en charge à Kisangani, RDC ». [Couple infertility. Epidemiological and clinical study and evaluation of management in Kisangani, DRC] Thèse De Bachelor, 2012, 66 p. |
| [10] | Alhassan A, Ziblim AR, Muntaka S. A survey on depression among infertile women in Ghana. BMC Womens Health 2014; 14: 42. |
| [11] | Nana PN, Wandji JC, Fomulu JN, Mbu RE, Leke RJI, Woubinwou MJ. Aspects Psycho-Sociaux chez Patients Infertiles à la Maternite Principale de l’Hôpital Central de Yaoundé, Cameroun. [Psycho-Social Aspects in Infertile Patients at the Main Maternity Ward of the Central Hospital of Yaoundé, Cameroon.] Clin Mother Child Health 2011; 8. |
| [12] | Ella SB. « Aspects épidémiologiques des lésions pelviennes et concordance hystérosalpingongraphie-cœlioscopie dans l’exploration de l’infertilité féminine 2017 » [Epidemiological aspects of pelvic lesions and concordance between hysterosalpingography and laparoscopy in the investigation of female infertility 2017] [Internet]. [Consulté le 14 février 2020]. Disponible sur: |
| [13] | Frydman R. Reproduction humaine et hormones. [Human reproduction and hormones] Rev Form Méd Continue. 2012; XXV (3-4): 1-9. |
| [14] | Rowe T. Fertility and a woman’s age. J Reprod Med 2006; 51: 157-63. |
| [15] | Bernard V, Bouvattier C, Christin-Maitre S. « Enjeux thérapeutiques en fertilité masculine ». [Therapeutic challenges in male fertility] Ann Endocrinol. 2015; 39: 39. |
| [16] | Frydman R, Eibschitz I, Papiernik E. « Les indications médicales de la fécondation ». [Medical indications for fertilization] Méd Sci 1985; 1: 122-128. |
| [17] | Wischmann T, Stammer H, Scherg H, Gerhard I, Verres R. Psychosocial characteristics of infertile couples: a study by the "Heidelberg Fertility Consultation Service". Hum Reprod 2001; 16: 1753-61. |
| [18] | Meka ENU, Foumane P, Essi MJ, Kamta AL, Essiben F, Mboudou ET. « Connaissances, attitudes et pratiques des femmes en désir d’enfant vis-à-vis de l’infertilité à l’hôpital gynéco-obstétrique et pédiatrique de Yaoundé ». [Knowledge, attitudes and practices of women desiring a child regarding infertility at the Yaoundé Gynecology, Obstetrics and Pediatrics Hospital] Health Sci Dis 2016; 17(4): 41-46. |
| [19] | La Croix Africa. « Données géographiques et identité religieuse au Sénégal » [Geographic data and religious identity in Senegal] Internet]. Croix Afr n.d. [Consulté le 3 février 2023]. Disponible sur: |
| [20] | Kougbeagbede Kuassigan IT. « Vécu psychologique de l’infertilité féminine au sein du couple à l’hôpital Saint-Luc de Cotonou ». [The psychological experience of female infertility within couples at Saint-Luc Hospital in Cotonou] Revue Ivoirienne de Sociologie et de Sciences Sociales, p. 314-327. |
| [21] | Seck S. « Vécu psychologique de l’infertilité du couple au Sénégal ». [The psychological experience of infertility in couples in Senegal] Ucad, Thèse Méd., Dakar, 2010; n°16, 128 p. |
| [22] | Mbow F, Toure ID. « Développer des approches pour comprendre, caractériser et adresser l’infertilité et ses conséquences pour les individus et les familles en Afrique subsaharienne: le cas du Sénégal. [Population Council ». Developing approaches to understand, characterize, and address infertility and its consequences for individuals and families in sub-Saharan Africa: the case of Senegal. Population Council] 2019; 21 p. |
| [23] | Adjamagbo K. « Aspects radiologiques de la pathologie utero-tubaire dans la stérilité féminine à propos de 1314 hystérosalpingographies au CHU de Lomé ». [Radiological aspects of utero-tubal pathology in female infertility: a study of 1314 hysterosalpingographies at the University Hospital of Lomé] Médecine d'Afrique Noire. 1993, 40 (10): 581-582. |
| [24] | Hind I. « Apport de l’hystérosalpingographie dans le bilan d’infertilité féminine : étude multicentrique à propos de 155 cas ». [The role of hysterosalpingography in the assessment of female infertility: a multicenter study of 155 cases] Ucad, Thèse Méd., Dakar, 2017; n°42, 131p. |
| [25] | Afoutou JM, Diallo AS, D’Almeida C, Faye O, Diallo D, Silou J, et al. « Place du test post-coïtal direct de Hühner dans le bilan de la stérilité conjugale en milieu africain au Sénégal. (À propos de 2593 tests post-coïtaux réalisés par le laboratoire de cytologie clinique, cyto-génétique et biologie de la reproduction du CHU de Dakar, Sénégal) 1983-1993 ». [The role of the direct post-coital Hühner test in the assessment of marital infertility in an African setting in Senegal. (A study of 2593 post-coital tests performed by the clinical cytology, cytogenetics and reproductive biology laboratory of the University Hospital of Dakar, Senegal) 1983-1993] Santé Publique. 1997; n°1612: 1-4. |
| [26] | Sundby J. Infertility in the Gambia: traditional and modern health care. Patient Educ Couns 1997; 31: 29-37. |
| [27] | Traoré M, Touré A, Sissoko S, Samaké NF. « Profil spermiologique des hommes infertiles au Mali ». [Sperm profile of infertile men in Mali] Andrologie 2008; 18: 253-7. |
| [28] | Pirrello-Parnot LP. « Étude de l’insatisfaction corporelle et du projet d’enfant chez les couples infertiles consultant en centre de procréation médicalement assistée ». [A study of body dissatisfaction and the desire to have children among infertile couples consulting at a medically assisted reproduction center] Université de Grenoble, Thèse Méd., Grenoble, 2006; 219 p. |
| [29] | Barillier H. « La stérilité féminine Prise en charge actuelle en France ». [Female infertility: Current management in France] Université de Caen, Thèse Méd., Caen, 2007; 213 p. |
| [30] | Goëb JL, Férel S, Guetta J, Dutilh P, Dulioust E, Guibert J, et al. « Vécus psychologiques des démarches d’Assistance médicale à la procréation ». [Psychological experiences of medically assisted reproduction procedures] Ann Méd-Psychol Rev Psychiatr 2006; 164: 781-8. |
| [31] | Papreen N, Sharma A, Sabin K, Begum L, Ahsan SK, Baqui AH. Living with infertility: experiences among Urban slum populations in Bangladesh. Reprod Health Matters 2000; 8: 33-44. |
| [32] | El Kissi Y, Amamou B, Hidar S, Ayoubi Idrissi K, Khairi H, Ali BBH. Quality of life of infertile Tunisian couples and differences according to gender. Int J Gynecol Obstet 2014; 125: 134-7. |
| [33] | Hassanin IMA, Abd-El-Raheem T, Shahin AY. Primary infertility and health-related quality of life in Upper Egypt. Int J Gynecol Obstet 2010; 110: 118-21. |
| [34] | Xiaoli S, Mei L, Junjun B, Shu D, Zhaolian W, Jin W, et al. Assessing the quality of life of infertile Chinese women: a cross-sectional study. Taiwan J Obstet Gynecol 2016; 55: 244-50. |
| [35] | Oddens BJ, den Tonkelaar I, Nieuwenhuyse H. Psychosocial experiences in women facing fertility problems--a comparative survey. Hum Reprod Oxf Engl 1999; 14: 255-61. |
| [36] | Peterson BD, Newton CR, Rosen KH, Schulman RS. Coping Processes of Couples Experiencing Infertility. Fam Relat 2006; 55: 227-39. |
| [37] | Gamet ML. « À propos d’une étude sur la sexualité des femmes et des hommes pendant la grossesse issue d’une Assistance médicale à la procréation (AMP) ». [Regarding a study on the sexuality of women and men during pregnancy resulting from Assisted Reproductive Technology (ART)] EMC Sexologies 2008; 17: 102-12. |
| [38] | Rossin B. « En quoi l’infertilité peut être source d’un sentiment d’agression ». [How infertility can be a source of feelings of aggression] EMC Sexologies. 2019; 28(2): 49-53. |
| [39] | Bourdet-Loubère S, Pirlot G. « Le vécu psychologique d’hommes infertiles ». [The psychological experience of infertile men] Inf Psychiatr 2012; 88: 721-6. |
| [40] | Bessoles P. « Infécondité féminine : un malaise dans la filiation ». [Female infertility: a problem in lineage] Clin Mediterr 2001; 63: 103-15. |
| [41] | Adam M. « La prise en charge du couple infertile en soins primaires: enquête auprès de médecins généralistes de Seine-Maritime et de l’Eure ». [Primary care management of infertile couples: a survey of general practitioners in Seine-Maritime and Eure] Université de Rouen, Thèse Méd., Rouen, 2018; 102 p. |
| [42] | Edelmann RJ, Connolly KJ. Psychological aspects of infertility. Br J Med Psychol 1986; 59(Pt 3): 209-19. |
| [43] | Ramezanzadeh F, Aghssa MM, Abedinia N, Zayeri F, Khanafshar N, Shariat M, et al. A survey of relationship between anxiety, depression and duration of infertility. BMC Womens Health 2004; 4: 9. |
| [44] |
Camborieux L. « L’infertilité, c’est dans la tête ? Non mais oui ». [Is infertility all in your head? No, but yes.] Disponible sur:
https://www.aftcc.org/sites/default/files/documents/camborieux_prise_en_charge_infertilite_aftcc.pdf 64 p. |
| [45] | Dunnigan L. « La naissance tardive d’une intervention psychosociale en infertilité ». [The late emergence of psychosocial intervention in infertility] Serv Soc 1988; 37: 120-36. |
APA Style
Koundoul, A., Diehiou, M., Gueye, A. K., Ndiaye, M. D., Dieng, A. K., et al. (2026). Psychological Experience of Couple Infertility Among Women in Senegal. American Journal of Psychiatry and Neuroscience, 14(2), 30-40. https://doi.org/10.11648/j.ajpn.20261402.11
ACS Style
Koundoul, A.; Diehiou, M.; Gueye, A. K.; Ndiaye, M. D.; Dieng, A. K., et al. Psychological Experience of Couple Infertility Among Women in Senegal. Am. J. Psychiatry Neurosci. 2026, 14(2), 30-40. doi: 10.11648/j.ajpn.20261402.11
@article{10.11648/j.ajpn.20261402.11,
author = {Adama Koundoul and Mansata Diehiou and Amadou Kane Gueye and Mame Diarra Ndiaye and Abdou Khadre Dieng and Diariatou Seck and Sokhna Seck and El Hadji Matar Ba and Philippe Marc Moreira},
title = {Psychological Experience of Couple Infertility Among Women in Senegal},
journal = {American Journal of Psychiatry and Neuroscience},
volume = {14},
number = {2},
pages = {30-40},
doi = {10.11648/j.ajpn.20261402.11},
url = {https://doi.org/10.11648/j.ajpn.20261402.11},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ajpn.20261402.11},
abstract = {Introduction: Infertility is defined as the inability of a couple to achieve a clinical pregnancy after at least twelve months of regular, unprotected sexual intercourse. It is a major reproductive health problem worldwide, affecting approximately 80 million people. In Senegal, infertility represents a significant health and social concern due to its prevalence, its psychosocial repercussions, and the burden of suffering it inflicts on affected couples. The objective of the study was to evaluate the psychological experience of infertility among women in couples. Materials and Methods: This is a prospective, cross-sectional and descriptive study carried out over the period from October 11, 2021 to October 17, 2022 at the maternity ward of the National Hospital Center “Dalal Jamm” in Dakar. This included women in a relationship for one year who were consulted for pregnancy and those followed for infertility. Data was collected by direct interview, entered into the KOBO application, processed and analyzed using Excel and SPSS software. Results: Out of a total of 100 women surveyed, the average age was 34 years. The age group of [30-37 years] was the most represented. The secondary education level was the most represented 31%. The liberal profession was 37%, Muslim women 95% and those in their first marriage 85%. Women had been cohabiting with their partner for more than 5 years in 54% of cases. Primary infertility was 61%. The spouse participated in the explorations in 68.8% of cases. Infertility was of female origin in 51% of cases. When the diagnosis was announced, women felt hopeless in 29.6% of cases. Chronic psychological manifestations such as anxiety (82%), depression (73%), self-defense mechanisms such as isolation (62%), affiliation (20%) and intellectualization (13%) were not noted in the patients. The types of help expressed by patients were medical (68%), financial (37%), spiritual (23%), and psychological (20%). Conclusion: Infertility is not only a reproductive health issue, but also a mental health problem due to the psychological suffering it causes. Psychological and medical care (PMA) would allow women to reduce psychological suffering and increase the chances of pregnancy.},
year = {2026}
}
TY - JOUR T1 - Psychological Experience of Couple Infertility Among Women in Senegal AU - Adama Koundoul AU - Mansata Diehiou AU - Amadou Kane Gueye AU - Mame Diarra Ndiaye AU - Abdou Khadre Dieng AU - Diariatou Seck AU - Sokhna Seck AU - El Hadji Matar Ba AU - Philippe Marc Moreira Y1 - 2026/04/10 PY - 2026 N1 - https://doi.org/10.11648/j.ajpn.20261402.11 DO - 10.11648/j.ajpn.20261402.11 T2 - American Journal of Psychiatry and Neuroscience JF - American Journal of Psychiatry and Neuroscience JO - American Journal of Psychiatry and Neuroscience SP - 30 EP - 40 PB - Science Publishing Group SN - 2330-426X UR - https://doi.org/10.11648/j.ajpn.20261402.11 AB - Introduction: Infertility is defined as the inability of a couple to achieve a clinical pregnancy after at least twelve months of regular, unprotected sexual intercourse. It is a major reproductive health problem worldwide, affecting approximately 80 million people. In Senegal, infertility represents a significant health and social concern due to its prevalence, its psychosocial repercussions, and the burden of suffering it inflicts on affected couples. The objective of the study was to evaluate the psychological experience of infertility among women in couples. Materials and Methods: This is a prospective, cross-sectional and descriptive study carried out over the period from October 11, 2021 to October 17, 2022 at the maternity ward of the National Hospital Center “Dalal Jamm” in Dakar. This included women in a relationship for one year who were consulted for pregnancy and those followed for infertility. Data was collected by direct interview, entered into the KOBO application, processed and analyzed using Excel and SPSS software. Results: Out of a total of 100 women surveyed, the average age was 34 years. The age group of [30-37 years] was the most represented. The secondary education level was the most represented 31%. The liberal profession was 37%, Muslim women 95% and those in their first marriage 85%. Women had been cohabiting with their partner for more than 5 years in 54% of cases. Primary infertility was 61%. The spouse participated in the explorations in 68.8% of cases. Infertility was of female origin in 51% of cases. When the diagnosis was announced, women felt hopeless in 29.6% of cases. Chronic psychological manifestations such as anxiety (82%), depression (73%), self-defense mechanisms such as isolation (62%), affiliation (20%) and intellectualization (13%) were not noted in the patients. The types of help expressed by patients were medical (68%), financial (37%), spiritual (23%), and psychological (20%). Conclusion: Infertility is not only a reproductive health issue, but also a mental health problem due to the psychological suffering it causes. Psychological and medical care (PMA) would allow women to reduce psychological suffering and increase the chances of pregnancy. VL - 14 IS - 2 ER -
Emile Badiane Psychiatric Center, Ziguinchor, Senegal
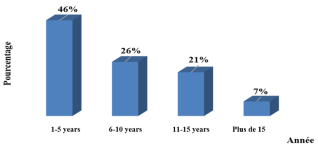
Figure 1. Distribution of patients according to the number of years of cohabitation with the spouse (N=100).
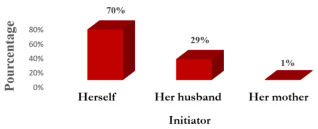
Figure 2. Distribution of patients according to the initiator of the decision to consult (N= 100).
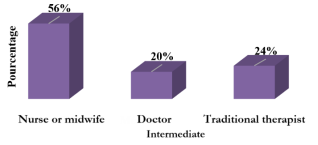
Figure 3. Distribution of patients according to type of intermediary (N=45).
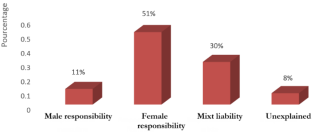
Figure 4. Distribution of responsibility for infertility (N=71).

Figure 5. Relationship with medical staff (N=100).
Information

