Abstract
Background: High-flow oxygen therapy is an ideal treatment for managing respiratory failure. It avoids orotracheal intubation; however, some patients are refractory to this treatment. The ROX Index aims to detect early failure in high-flow oxygen therapy; nevertheless, its use has been poorly studied in pediatrics. Objective: To evaluate the applicability of the ROX Index as a tool to determine the failure of high-flow oxygen therapy in pediatric patients admitted to the Roberto Gilbert Hospital. Methodology: Observational, prospective, longitudinal cohort study with a descriptive approach including 209 patients between 1 month and 17 years old who required high-flow oxygen therapy within the first 24 hours. ROX Index measurements were taken at 2, 4, 6, 12, and 24 hours with follow-up to determine the outcome. Result: A total of 209 patients meeting the inclusion criteria were obtained; 27 (12.9%) required endotracheal intubation (ETI), and 182 (87%) received high-flow oxygen therapy (HFNC). A higher frequency of younger infants was observed among patients who required ETI, with a median age of 12 months. A significant difference in the ROX index was found from two hours onwards with cutoff points on the AUROC curve above 0.5. Conclusion: It was determined that the ROX Index can be used as a complementary tool to strengthen decision-making in pediatrics.
Keywords
High-Flow Oxygen Therapy, Predictors, ROX Index, Tool, Achievable, Endotracheal Intubation
1. Introduction
High flow oxygen therapy has been established as a fundamental treatment in pediatric hospital settings for managing acute hypoxemic respiratory failure, avoiding the need for progressing to invasive mechanical ventilation. In other words; by serving as a bridge of respiratory support, high-flow oxygen therapy avoids immediate endotracheal intubation, thereby conserving resources in various pediatric intensive care units around the world
| [1] | Silva-Guayasamín LG, Callejas D, Silva-Sarabia CA, Silva-Orozco GS. EPIDEMIOLOGICAL PROFILE OF ACUTE RESPIRATORY INFECTIONS IN PEDIATRIC PATIENTS IN ECUADOR. Enferm Investiga Investig Link Teaching Gest [Internet]. 2022; 7(2): 87–92. Available in: http://dx.doi.org/10.31243/ei.uta.v7i2.1620.2022 |
| [2] | Dulcey-Sarmiento LA, Castillo-Blanco JF, Theran-Leon JS, Caltagirone-Miceli R, Aguas-Cantillo MJ. Utility of the ROX Index as a Predictor of Respiratory Failure, Mortality and Complications in Patients with COVID-19 Without Invasive Ventilator Support, Unicentric Study [Internet]. Zenodo; 2022. Available in: http://dx.doi.org/10.5281/ZENODO.6949776 |
[1, 2]
.
Although high-flow oxygen therapy is primarily used in pediatric emergency rooms to prevent orotracheal intubation, some patients exhibit refractory hypoxemia to this type of non-invasive ventilation. In fact, despite the use of high-flow oxygen therapy, certain respiratory pathologies can present severe gas exchange impairment in the first hours of treatment, increasing the predisposition to require intubation and, consequently, mortality if its use is delayed
| [3] | Villanueva M, Alapont M. High flow oxygen in bronchiolitis. What if in the end it turns out not? Evid Pediatr. 2023; 19. |
| [4] | Chung-Engracia S, Cornejo-Briones C, López-Toledo M, Moreno-Castro F. Acute respiratory failure in pediatrics. [Internet]. 2022; 6(3): 166–74. Available in: http://dx.doi.org/10.26820/recimundo/6.(3).junio.2022.166-174 |
[3, 4]
.
Various parameters such as respiratory rate, oxygen saturation, and inspired fraction of oxygen are routinely used to monitor patients in emergency rooms; similarly, the assessment of respiratory work is a subjective variable, as it depends on the examiner, in the absence of advanced monitoring. Therefore, having a tool that integrates these parameters will provide a comprehensive view of the clinical status of pediatric patients. The Respiratory Rate-Oxygenation Index (ROX Index) was created to early detect the failure in the use of high flow oxygen therapy
| [2] | Dulcey-Sarmiento LA, Castillo-Blanco JF, Theran-Leon JS, Caltagirone-Miceli R, Aguas-Cantillo MJ. Utility of the ROX Index as a Predictor of Respiratory Failure, Mortality and Complications in Patients with COVID-19 Without Invasive Ventilator Support, Unicentric Study [Internet]. Zenodo; 2022. Available in: http://dx.doi.org/10.5281/ZENODO.6949776 |
| [5] | Webb L, Chahine R, Aban I, Prabhakaran P, Loberger J. Predicting high-flow nasal cannula therapy outcomes using the ROX-HR index in the pediatric ICU. Respir Care [Internet]. 2022; respcare.09765. Available in: http://dx.doi.org/10.4187/respcare.09765 |
| [6] | Junhai Z, Jing Y, Beibei C, Li L. The value of ROX index in predicting the outcome of high flow nasal cannula: a systematic review and meta-analysis. Breathe Res [Internet]. 2022; 23(1). Available in: http://dx.doi.org/10.1186/s12931-022-01951-9 |
[2, 5, 6]
.
2. Methods
Observational, prospective, longitudinal cohort study with a descriptive approach in pediatric patients who required high-flow oxygen therapy and were treated in the emergency area of Roberto Gilbert Elizalde Hospital during the period from February to September 2023.
Within the study design, inclusion criteria included: patients admitted to the emergency department of Roberto Gilbert Elizalde Hospital, requiring high-flow oxygen therapy due to acute respiratory failure aged between 1 month to 17 years, and who required high-flow oxygen therapy within the first 24 hours of admission. Patients with a history of high-flow oxygen therapy use, caregiver refusal of endotracheal intubation, as well as patients with comorbidities such as neurodegenerative diseases, heart diseases, cerebral palsy, and genetic disorders were excluded from the study. Patients with moderate to severe acute respiratory distress syndrome were also excluded.
The evaluated variables were: sociodemographic data of each patient, admission diagnosis, length of hospital stay, duration of high-flow oxygen therapy, and assessment scales used within the hospital (Downes Score, Pulmonary Score, Wang Score). This data was obtained through the review of digital medical records from the SERVINTE system of Roberto Gilbert Elizalde Hospital. The ROX Index was calculated using the following formula: (Sat/Fio2)/RR. Measurements were made at 2, 4, 6, 12 and 24 hours, with subsequent follow-up of the patients to determine their outcome (need for invasive ventilation or not), and forms were used for the registration of this variable.
The information was initially tabulated in a database using the Excel program. IBM SPSS Statistics 28 program for Windows 10 was used for statistical analysis. Quantitative variables were presented as medians with interquartile range, and qualitative variables as frequencies and percentages. The Mann-Whitney U test was used for the contrast of continuous variables, and the chi-square test or Fisher's exact test for qualitative variables; as appropriate.
Finally, to evaluate the predictive capacity of the ROX Index on the success of high-flow oxygen therapy, an analysis with the ROC curve was performed to find the cut-off point associated with the success of the technique, as well as the calculation of the area under the ROC curve (AUROC) to determine the probability of association of the chosen cut-off point associated with the success of high-flow oxygen therapy.
3. Results
During the study period, a sample of 209 patients who met the inclusion criteria and received respective follow-up was obtained. Out of this total figure, 27 (12.9%) patients required endotracheal intubation and 182 (87%) received only high-flow oxygen therapy without the need for escalated interventions.
In the analysis of the variables presented in
Table 1; it is initially highlighted that the sample had a median age of 12 months (IQR 7 – 36). In those patients who were intubated, the median was 10 months (IQR 5-24), in contrast to a median age of 12 months (IQR 7-48) in those who remained only on HFNC. A higher frequency of younger infants was observed among patients who received ETI, corresponding to 66.6% (p=.023). Regarding gender, 107 (51.2%) patients were female, while 102 (48.8%) were male.
Pneumonia was identified as the main cause of respiratory failure, accounting for 155 (74.2%) cases, followed by bronchiolitis in 46 (22%) and asthma in 8 (3.8%). No significant differences were found between these groups (p=0.428). It was also identified that within the group of intubated patients, pneumonia diagnosis was more prevalent, representing 70.4% of the population.
Analyzing the median time under high-flow oxygen therapy, it was found to be significantly shorter in those who required ETI (14 vs. 65 hours; p<.001). Additionally, in this group, the median length of hospital stay was significantly longer (20 vs. 7 days; p<.001). Another important point to note is mortality.
Regarding this; only 3 (1.4%) patients died within the study period. All of them required endotracheal intubation, with a p-value corresponding to <0.05. As another important pillar of the study, the ROX Index was evaluated throughout the patient follow-up. This monitoring was carried out from their arrival in the emergency room until 24 hours or endotracheal intubation.
Table 1. Study population characteristics.
| Total (N=209) | ETI (N=27) | HFNC only (N=182) | p value |
Age (months), median (IQR) | 12 (7 – 36) | 10 (5 – 24) | 12 (7 – 48) | .023a |
Young infant (1-12 months) | 120 (53.6) | 18 (66.6) | 102 (56.0) | |
Older infant (13-24 months) | 21 (10.0) | 6 (22.2) | 15 (8.2) | |
Preschool (2 to 6 years) | 53 (25.4) | 3 (11.1) | 50 (27.5) | |
School-age (7 to 10 years) | 11 (5.3) | - | 11 (6.0) | |
Adolescent (11 to 17 years) | 4 (1.9) | - | 4 (2.2) | |
Gender, n (%) | | | | .894b |
Female | 107 (51.2) | 13 (48.1) | 94 (51.6) | |
Male | 102 (48.8) | 14 (51.9) | 88 (48.4) | |
Diagnosis, n (%) | | | | .428c |
| Bronchiolitis | 46 (22.0) | 8 (29.6) | 38 (20.9) | |
Asthma | 8 (3.8) | - | 8 (4.4) | |
Pneumonia | 155 (74.2) | 19 (70.4) | 136 (74.7) | |
Community-acquired pneumonia | 113/155 | 7/19 | 52/136 | |
Complicated pneumonia | 36/155 | 7/19 | 29/136 | |
Bronchial obstructive syndrome | 60/155 | 5/19 | 55/136 | |
Time under high-flow mask (hours), median (IQR) | 56 (36 – 84) | 14 (6 – 23.5) | 65 (42 – 87.8) | <.001a |
Hospitalization time (days), median (IQR) | 7 (6 – 12) | 20 (12.5 – 27) | 7 (5 – 10) | <.001a |
Discharge status, n (%) | | | | <.001c |
Dead | 3 (1.4) | 3 (11.1) | - | |
Alive | 206 (98.6) | 24 (88.9) | 182 (100.0) | |
Mann-Whitney U test. Pearson chi-square test. Fisher's exact test | | | | |
Additionally, the ROX Index was measured at 2-4-6, and 12 hours after starting high-flow oxygen therapy.
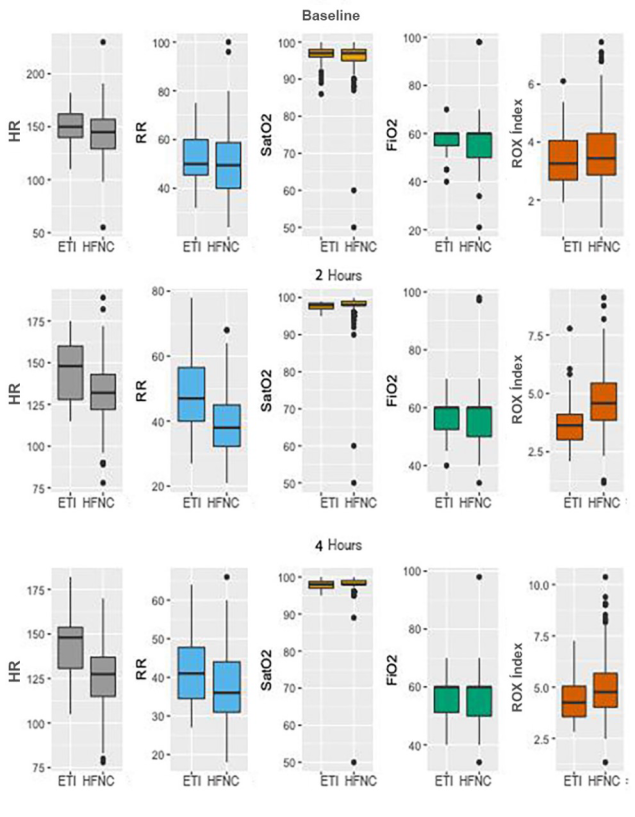
Figures 1 and 2 summarizes the results obtained in the different measurements. Firstly, it is observed that the initial value of the ROX Index upon arrival at the emergency department, also known as baseline value, did not show statistically significant differences between those who required ETI and those who only needed HFNC.
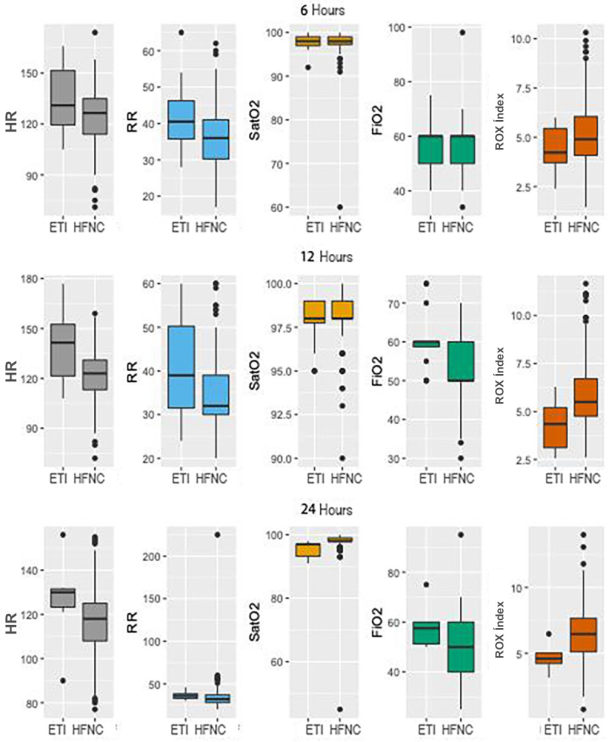
However, as time progressed, these results changed. Notice the significant difference in the ROX Index from two hours after their arrival in the emergency room (3.62 vs 4.58; p<.001), at the expense of respiratory rate (47 vs 38 RPM; p<.001).
From 12 hours onwards, this difference was also related to FiO2 (60 vs 50; p<.001). Furthermore, it was possible to evidence maximum statistical significance at 6 hours of measurement, as well as increased variability at the expense of heart rate.
Additionally; as part of the statistical analysis, a comparison was carried out between the various scales used in the emergency and the ROX Index. Downes, Wang and Pulmonary scales showed better observed agreement than the ROX Index, and this trend progressively increased throughout the baseline, 2, 4, 6, 12 and 24 hours measurements, with percentages of 72.73%, 88.52%, 90.2%, 91.09%, 91.41% and 95.53%, respectively (
table 2).
This observed agreement was higher than that observed when using the cut-off value of <4.88 of the ROX Index: 26.32% (p=.467), 44.5% (p=.004), 48.04% (p=.017), 52.97% (p=.016), 69.19% (p=.625) and 76.54% (p=.06), respectively. Using the cut-off value obtained from this research, the following observed agreement was obtained: 67.94% (p=.621), 68.9% (p=.025), 61.27% (p=.024), 32.67% (p =.028), 79.8% (p=.754), 74.86% (p=.021).
Figure 1. Vital signs and baseline ROX Index, at two, four, six, twelve and twenty-four hours after arrival at the Emergency Department; stratified according to the indication for endotracheal intubation.
Figure 2. Vital signs and baseline ROX Index, at two, four, six, twelve and twenty-four hours after arrival at the Emergency Department; stratified according to the indication for endotracheal intubation.
Likewise, it could be observed in
Table 2 that while the ROX Index has higher sensitivity than clinical scales (>60%) with a high negative predictive value, these are characterized by having higher specificity (>70%) with a higher positive predictive value.
Regarding the follow-up, the following was found: at 4 hours, 5 patients had exited the study due to endotracheal intubation; at 6 hours, 2 more also due to ETI. At 12 hours, 4 more patients for the same reason and, at 24 hours, 19 more. In the latter case, 10 patients due to ETI and 9 for remaining on high-flow oxygen therapy (
table 2).
Within the framework of this research, several cut-off points were obtained through the follow-up carried out on the patients. Having as a reference the cut-off value from the literature (<4.88), several aspects can be described.
Primarily, although the cut-off value of the ROX Index obtained in this study was superior during the baseline measurement (<2.97 vs <4.88 with an observed agreement of 67.94%); at 2, 4 and 12 hours, the progressive growth seen in the observed agreement of the clinical scales and the cut-off value from the literature of the ROX Index was not observed (
table 2).
Table 2. Prognostic sufficiency for the need of endotracheal intubation, using the clinical scales Downes, Wang and Pulmonary, ROX index according to the cut-off value from the literature (<4.88), and the one established from the data of this study.
| Sensitivity | Specificity | Positive Predictive Value | Negative Predictive Value | Observed Agreement | AUROC | P value |
Baseline |
Scale (Severe) | 11/27; 40.74 | 141/182; 77.47 | 11/52; 21.15 | 141/157; 89.81 | 152/209; 72.73 | 0.55 | ref |
(22.39-61.2) | (70.71-83.32) | (11.06-34.7) | (83.98-94.06) | (66.15-78.64) |
ROX (<4.88) | 24/27; 88.89 | 31/182; 17.03 | 24/175; 13.71 | 31/34; 91.18 | 55/209; 26.32 | 0.524 | .467* |
(70.84-97.65) | (11.88-23.3) | (8.99-19.72) | (76.32-98.14) | (20.48-32.84) |
ROX (>2.97) | 11/27; 40.74 | 131/182; 71.98 | 11/62; 17.74 | 131/147; 89.12 | 142/209; 67.94 | 0.534 | .621* |
(22.39-61.2) | (64.86-78.37) | (9.2-29.53) | (82.93-93.65) | (61.15-74.21) |
Two hours |
Scale (Severe) | 8/27; 29.63 | 177/182; 97.25 | 8/13; 61.54 | 177/196; 90.31 | 185/209; 88.52 | 0.759 | ref |
(13.75-50.18) | (93.71-99.1) | (31.58-86.14) | (85.28-94.06) | (83.4-92.5) |
ROX (<4.88) | 21/27; 77.78 | 72/182; 39.56 | 21/131; 16.03 | 72/78; 92.31 | 93/209; 44.5 | 0.542 | .004* |
(57.74-91.38) | (32.4-47.06) | (10.21-23.45) | (84.01-97.12) | (37.64-51.51) |
ROX (<4.04) | 18/27; 66.67 | 126/182; 69.23 | 18/74; 24.32 | 126/135; 93.33 | 144/209; 68.9 | 0.588 | .026* |
(46.04-83.48) | (61.98-75.85) | (15.1-35.69) | (87.72-96.91) | (62.15-75.11) |
Four hours |
Scale (Severe) | 4/22; 18.18 | 180/182; 98.9 | 4/6; 66.67 | 180/198; 90.91 | 184/204; 90.2 | 0.788 | ref |
(5.19-40.28) | (96.09-99.87) | (22.28-95.67) | (86.01-94.52) | (85.27-93.91) |
ROX (<4.88) | 15/22; 68.18 | 83/182; 45.6 | 15/114; 13.16 | 83/90; 92.22 | 98/204; 48.04 | 0.527 | .017* |
(45.13-86.14) | (38.22-53.14) | (7.56-20.77) | (84.63-96.82) | (41.01-55.13) |
ROX (<4.44) | 13/22; 59.09 | 112/182; 61.54 | 13/83; 15.66 | 112/121; 92.56 | 125/204; 61.27 | 0.541 | .024* |
(36.35-79.29) | (54.05-68.64) | (8.61-25.29) | (86.35-96.54) | (54.22-68) |
Six hours |
Scale (Severe) | 3/20; 15 | 181/182; 99.45 | 3/4; 75 | 181/198; 91.41 | 184/202; 91.09 | 0.832 | ref |
(3.21-37.89) | (96.98-99.99) | (19.41-99.37) | (86.61-94.92) | (86.28-94.63) |
ROX (<4.88) | 12/20; 60 | 95/182; 52.2 | 12/99; 12,12 | 95/103; 92.23 | 107/202; 52.97 | 0.522 | .016* |
(36.05-80.88) | (44.68-59.64) | (6.42-20.22) | (85.27-96.59) | (45.84-60.01) |
ROX (<6.00) | 19/20; 95 | 47/182; 25.82 | 19/154; 12.34 | 47/48; 97.92 | 66/202; 32.67 | 0.551 | .028* |
(75.13-99.87) | (19.63-32.82) | (7.59-18.59) | (88.93-99.95) | (26.26-39.61) |
Twelve hours |
Scale (Severe) | 1/16; 6.25 | 180/182; 98.9 | 1/3; 33.33 | 180/195; 92.31 | 181/198; 91.41 | 0.628 | ref |
(0.16-30.23) | (96.09-99.87) | (0.84-90.57) | (87.63-95.63) | (86.61-94.92) |
ROX (<4.88) | 9/16; 56.25 | 128/182; 70.33 | 9/63; 14.29 | 128/135; 94.81 | 137/198; 69.19 | 0.546 | .625* |
(29.88-80.25) | (63.12-76.86) | (6.75-25.39) | (89.61-97.89) | (62.26-75.54) |
ROX (<4.39) | 8/16; 50 | 150/182; 82.42 | 8/40; 20 | 150/158; 94.94 | 158/198; 79.8 | 0.575 | .754* |
(24.65-75.35) | (76.1-87.65) | (9.05-35.65) | (90.27-97.79) | (73.52-85.16) |
Twenty-four hours |
Scale (Severe) | 0/6; 0 | 171/173; 98.84 | 0/2; 0 | 171/177; 96.61 | 171/179; 95.53 | 0.483 | ref |
(0-45.93) | (95.89-99.86) | (0-84.19) | (92.77-98.75) | (91.38-98.05) |
ROX (<4.88) | 3/6; 50 | 134/173; 77.46 | 3/42; 7.14 | 134/137, 97.81 | 137/179; 76.54 | 0.525 | .060* |
(11.81-88.19) | (70.5-83.45) | (1.5-19.48) | (93.73-99.55) | (69.64-82.54) |
ROX (<5.05) | 4/6; 66.67 | 130/173; 75.14 | 4/47; 8.51 | 130/132; 98.48 | 134/179; 74.86 | 0.535 | .021* |
(22.28-95.67) | (68.02-81.39) | (2.37-20.38) | (94.63-99.82) | (67.84-81.03) |
*Delong test | | | | | |
Regarding the area under the curve shown in
Figure 3, it is illustrated that the AUROC of the clinical scales (red-colored line); at 2, 4 and 6 hours is significantly superior to the curves generated by the ROX Index, regardless of the cut-off value used. Finally; considering that a value close to 1 in terms of AUROC curve indicates better discriminatory ability, the values obtained for the different cut-off points of the ROX Index (both the one described in the literature and from this study) range above 0.5, being considered acceptable.
Figure 3. Area under the curve (AUROC), describing prognostic sufficiency for the requirement of endotracheal intubation (ETI), using the clinical scales Downes, Wang and Pulmonary (red line), ROX Index according to the cut-off value from the literature (<4.88, blue line), and the one established from the data of this study (dotted blue line).
4. Discussion
The research constitutes one of the few studies aiming to evaluate whether the ROX Index, previously validated in adults, has the capacity to predict the need to escalate to invasive mechanical ventilation in the pediatric population.
It has been widely reported in the literature that in pediatric patients with acute respiratory failure, the failure rate can reach up to 50%. This value can vary significantly depending on the particular characteristics of the studied population. Age, sex and cause of acute respiratory failure are the factors mostly involved in this fluctuation
| [7] | Yildizdas D, Yontem A, Iplik G, Horoz OO, Ekinci F. Predicting nasal high-flow therapy failure by pediatric respiratory rate-oxygenation index and pediatric respiratory rate-oxygenation index variation in children. Eur J Pediatr [Internet]. 2021; 180(4): 1099–106. Available in: http://dx.doi.org/10.1007/s00431-020-03847-6 |
| [8] | Vásquez-Hoyos P, Jiménez-Chaves A, Tovar-Velásquez M, Albor-Ortega R, Palencia M, Redondo-Pastrana D, et al. Factors associated with failure of high-flow nasal cannula therapy in pediatric patients with respiratory failure in two high-altitude pediatric critical care units. Med Intensiva (Engl Ed) [Internet]. 2021; 45(4): 195–204. Available in: http://dx.doi.org/10.1016/j.medin.2019.10.005 |
[7, 8]
.
The demographic distribution in terms of age and associated pathology in this study is similar to that of other cohorts where both the success and failure of HFNC have been analyzed. Consistent with our sample, both the study by Yildizdas et al. and Vásquez et al. identified a higher incidence in younger infants
| [7] | Yildizdas D, Yontem A, Iplik G, Horoz OO, Ekinci F. Predicting nasal high-flow therapy failure by pediatric respiratory rate-oxygenation index and pediatric respiratory rate-oxygenation index variation in children. Eur J Pediatr [Internet]. 2021; 180(4): 1099–106. Available in: http://dx.doi.org/10.1007/s00431-020-03847-6 |
| [8] | Vásquez-Hoyos P, Jiménez-Chaves A, Tovar-Velásquez M, Albor-Ortega R, Palencia M, Redondo-Pastrana D, et al. Factors associated with failure of high-flow nasal cannula therapy in pediatric patients with respiratory failure in two high-altitude pediatric critical care units. Med Intensiva (Engl Ed) [Internet]. 2021; 45(4): 195–204. Available in: http://dx.doi.org/10.1016/j.medin.2019.10.005 |
[7, 8]
. Additionally, it is highlighted that pneumonia is the main cause of high-flow oxygen therapy failure; although few studies indicate a higher number of patients with bronchiolitis.
| [6] | Junhai Z, Jing Y, Beibei C, Li L. The value of ROX index in predicting the outcome of high flow nasal cannula: a systematic review and meta-analysis. Breathe Res [Internet]. 2022; 23(1). Available in: http://dx.doi.org/10.1186/s12931-022-01951-9 |
| [9] | Roca O, Messika J, Caralt B, García-de-Acilu M, Sztrymf B, Ricard JD, et al. Predicting success of high-flow nasal cannula in pneumonia patients with hypoxemic respiratory failure: The utility of the ROX index. J Crit Care [Internet]. 2016; 35: 200–5. Available in: http://dx.doi.org/10.1016/j.jcrc.2016.05.022 |
| [10] | Goh K, Chai H, Ong T, Sewa D, Phua G, Tan Q. Early prediction of high flow nasal cannula therapy outcomes using a modified ROX index incorporating heart rate. J Intensive Care [Internet]. 2020; 8(1). Available in: http://dx.doi.org/10.1186/s40560-020-00458-z |
[6, 9, 10]
.
Taking gender as another important point; although the majority of participants in this study were females, it was males who required endotracheal intubation. This finding aligns with the report of 49.6% of males undergoing this procedure in the study published by Yildizdas et al
| [7] | Yildizdas D, Yontem A, Iplik G, Horoz OO, Ekinci F. Predicting nasal high-flow therapy failure by pediatric respiratory rate-oxygenation index and pediatric respiratory rate-oxygenation index variation in children. Eur J Pediatr [Internet]. 2021; 180(4): 1099–106. Available in: http://dx.doi.org/10.1007/s00431-020-03847-6 |
[7].
However, notable variability persists, reflecting the disparities found in different studies documented in the medical literature
.
Analyzing the median time on high-flow oxygen therapy, the findings obtained coincide with the reviewed literature. Several studies indicate that the duration of HFNC varies, with successful cases lasting around 3 days and approximately 1 day for failures, consistent with previously reported findings
| [8] | Vásquez-Hoyos P, Jiménez-Chaves A, Tovar-Velásquez M, Albor-Ortega R, Palencia M, Redondo-Pastrana D, et al. Factors associated with failure of high-flow nasal cannula therapy in pediatric patients with respiratory failure in two high-altitude pediatric critical care units. Med Intensiva (Engl Ed) [Internet]. 2021; 45(4): 195–204. Available in: http://dx.doi.org/10.1016/j.medin.2019.10.005 |
| [9] | Roca O, Messika J, Caralt B, García-de-Acilu M, Sztrymf B, Ricard JD, et al. Predicting success of high-flow nasal cannula in pneumonia patients with hypoxemic respiratory failure: The utility of the ROX index. J Crit Care [Internet]. 2016; 35: 200–5. Available in: http://dx.doi.org/10.1016/j.jcrc.2016.05.022 |
| [10] | Goh K, Chai H, Ong T, Sewa D, Phua G, Tan Q. Early prediction of high flow nasal cannula therapy outcomes using a modified ROX index incorporating heart rate. J Intensive Care [Internet]. 2020; 8(1). Available in: http://dx.doi.org/10.1186/s40560-020-00458-z |
[8-10]
. Regarding the hospitalization period; the stay was significantly shorter in patients whose treatment was successful, as described by Artacho et al
| [12] | Artacho-Ruiz R, Artacho-Jurado B, Caballero-Güeto F, Cano-Yuste A, Durbán-García I, García-Delgado F, et al. Predictors of success of high-flow nasal cannula treatment in hypoxemic acute respiratory failure. Med Intensiva [Internet]. 2021; 45(2): 80–7. Available in: http://dx.doi.org/10.1016/j.medin.2019.07.012 |
[12].
In this study, it was documented that a total of 3 patients, equivalent to 1.4%, died while on invasive mechanical ventilation. These figures resemble those reported by Vásquez et al, who registered a 3.9% mortality rate
| [8] | Vásquez-Hoyos P, Jiménez-Chaves A, Tovar-Velásquez M, Albor-Ortega R, Palencia M, Redondo-Pastrana D, et al. Factors associated with failure of high-flow nasal cannula therapy in pediatric patients with respiratory failure in two high-altitude pediatric critical care units. Med Intensiva (Engl Ed) [Internet]. 2021; 45(4): 195–204. Available in: http://dx.doi.org/10.1016/j.medin.2019.10.005 |
[8]
. Yildizdas et al also report a mortality rate of around 3.8% with no recorded deaths among patients who only needed HFNC
| [7] | Yildizdas D, Yontem A, Iplik G, Horoz OO, Ekinci F. Predicting nasal high-flow therapy failure by pediatric respiratory rate-oxygenation index and pediatric respiratory rate-oxygenation index variation in children. Eur J Pediatr [Internet]. 2021; 180(4): 1099–106. Available in: http://dx.doi.org/10.1007/s00431-020-03847-6 |
[7].
This clearly indicates that the risk of mortality is higher in those who do not respond to high-flow oxygen therapy.
Predicting the outcome regarding the management of patients with high-flow oxygen therapy ensures the rapid identification of those at higher risk of requiring endotracheal intubation. The ROX Index, first introduced by Roca et al and evaluated in an adult population diagnosed with pneumonia, was designed and validated for this purpose
| [9] | Roca O, Messika J, Caralt B, García-de-Acilu M, Sztrymf B, Ricard JD, et al. Predicting success of high-flow nasal cannula in pneumonia patients with hypoxemic respiratory failure: The utility of the ROX index. J Crit Care [Internet]. 2016; 35: 200–5. Available in: http://dx.doi.org/10.1016/j.jcrc.2016.05.022 |
| [13] | Salvatico E, Storaccio S, Ulloa A, Prado S, Diaz M. High flow oxygen therapy (HFO) in pediatrics. An innovative experience. Sick notes (Córdoba) [Internet]. 2017; 23–8. Available in: https://pesquisa.bvsalud.org/portal/resource/pt/biblio-907856 |
[9, 13].
Several analyzes can be performed in relation to this index. Firstly, the optimal follow-up time should be determined to carry out the evaluation. In this research, statistical significance was found from 2 hours of follow-up, reaching a peak at 6 hours, corroborating that accuracy improves over time. It should be noted that this varies considerably among studies, depending on the investigated population, mostly adults; However, most studies agree on considering 6 hours as the best time for index collection
| [3] | Villanueva M, Alapont M. High flow oxygen in bronchiolitis. What if in the end it turns out not? Evid Pediatr. 2023; 19. |
| [7] | Yildizdas D, Yontem A, Iplik G, Horoz OO, Ekinci F. Predicting nasal high-flow therapy failure by pediatric respiratory rate-oxygenation index and pediatric respiratory rate-oxygenation index variation in children. Eur J Pediatr [Internet]. 2021; 180(4): 1099–106. Available in: http://dx.doi.org/10.1007/s00431-020-03847-6 |
| [14] | Chang C, Lin Y, Chen T, Lin J, Hsia S, Chan O, et al. High-flow nasal cannula therapy in children with acute respiratory distress with hypoxia in A pediatric intensive care unit–A single center experience. Front Pediatr [Internet]. 2021; 9. Available in: http://dx.doi.org/10.3389/fped.2021.664180 |
[3, 7, 14]
.
In the study conducted by Roca et al, it was demonstrated that the best predictor of HFNC success is respiratory rate, with a significant reduction observed at 2 hours of management
| [9] | Roca O, Messika J, Caralt B, García-de-Acilu M, Sztrymf B, Ricard JD, et al. Predicting success of high-flow nasal cannula in pneumonia patients with hypoxemic respiratory failure: The utility of the ROX index. J Crit Care [Internet]. 2016; 35: 200–5. Available in: http://dx.doi.org/10.1016/j.jcrc.2016.05.022 |
[9]
. This trend was replicated in other studies carried out in adult population, as observed in the study by Artacho et al
| [12] | Artacho-Ruiz R, Artacho-Jurado B, Caballero-Güeto F, Cano-Yuste A, Durbán-García I, García-Delgado F, et al. Predictors of success of high-flow nasal cannula treatment in hypoxemic acute respiratory failure. Med Intensiva [Internet]. 2021; 45(2): 80–7. Available in: http://dx.doi.org/10.1016/j.medin.2019.07.012 |
[12]
. However, this research which included pediatric patients, a notable variability in respiratory rate at 2 hours (47 vs 38 RPM; p<.001) was observed.
Considering changes in respiratory rate according to age in pediatrics, a study published by Yildizdas et al used the SCORE-Z of respiratory rate instead of the RR alone in the calculation, referred to as p- ROXI. This analysis revealed that this index had a superior accuracy in predicting HFNC failure, with an area under the ROC curve (AUROC) of 0.79. It is relevant to mention that this study represents the first and only one to use the score-z of respiratory rate as a variable, implying that it has not yet been validated
| [7] | Yildizdas D, Yontem A, Iplik G, Horoz OO, Ekinci F. Predicting nasal high-flow therapy failure by pediatric respiratory rate-oxygenation index and pediatric respiratory rate-oxygenation index variation in children. Eur J Pediatr [Internet]. 2021; 180(4): 1099–106. Available in: http://dx.doi.org/10.1007/s00431-020-03847-6 |
[7].
In addition to respiratory rate, heart rate also shows greater variability throughout the index measurement, as evidenced in this study. It has been widely described in the literature that a gradual increase in HR is directly related to failure in HFNC use. Since heart rate is an easily obtainable vital sign at the patient's bedside, Goh et al published a study exploring the possibility of incorporating it into the ROX Index to improve its diagnostic accuracy
| [10] | Goh K, Chai H, Ong T, Sewa D, Phua G, Tan Q. Early prediction of high flow nasal cannula therapy outcomes using a modified ROX index incorporating heart rate. J Intensive Care [Internet]. 2020; 8(1). Available in: http://dx.doi.org/10.1186/s40560-020-00458-z |
[10]
. However, this study was the only one that evaluated this additional variable to predict HFNC failure in the context of an adult population
.
Due to the severity of respiratory pathology, there are various clinical scales in pediatrics that allow patients to be staged
. Based on the obtained sample, it was possible to compare these scales with the ROX Index. These scales show better observed agreement, while the ROX Index demonstrated a higher negative predictive value, suggesting that it is reliable in ruling out the possibility of HFNC failure. However, it is necessary to replicate this study in other investigations to determine if any of the clinical scales are superior to the ROX Index.
Another crucial aspect focuses on the cut-off point of the ROX Index. Compared to the study by Roca et al, the cut-off points identified in this study do not demonstrate superiority
| [9] | Roca O, Messika J, Caralt B, García-de-Acilu M, Sztrymf B, Ricard JD, et al. Predicting success of high-flow nasal cannula in pneumonia patients with hypoxemic respiratory failure: The utility of the ROX index. J Crit Care [Internet]. 2016; 35: 200–5. Available in: http://dx.doi.org/10.1016/j.jcrc.2016.05.022 |
| [17] | Roca O, Caralt B, Messika J, Samper M, Sztrymf B, Hernández G, et al. An index combining respiratory rate and oxygenation to predict outcome of nasal high-flow therapy. Am J Respir Crit Care Med [Internet]. 2019; 199(11): 1368–76. Available at: http://dx.doi.org/10.1164/rccm.201803-0589oc |
[9, 17]
. Additionally; the progressive growth observed in the analysis carried out in this study, around the cut-off point of <4.88 indicates that as the clinical case progresses, it approaches the requirement for ETI or not IOT, highlighting the importance of making more precise measurements at times close to this critical point.
It is important to note that this is not a diagnostic clinical trial. The decision regarding the need for ETI was made based on clinical individualization. The decision to discontinue HFNC and initiate intubation was made through the physician's clinical evaluation, supported by the application of clinical scales (Downes, Wang and Pulmonary) together with the deterioration of vital signs, evidence of respiratory acidosis in the arterial blood gas, significant hemodynamic instability (with or without the need for vasopressors), and deterioration of neurological status.
The cut-off points for the ROX Index show wide variation in the literature, with studies reporting ranges from 2.7 to 9.2. Although so far, the best cut-off point has been estimated to be 4.88, which constitutes a predictor of success, there is no universal consensus on the best cut-off point in the pediatric population
| [3] | Villanueva M, Alapont M. High flow oxygen in bronchiolitis. What if in the end it turns out not? Evid Pediatr. 2023; 19. |
| [7] | Yildizdas D, Yontem A, Iplik G, Horoz OO, Ekinci F. Predicting nasal high-flow therapy failure by pediatric respiratory rate-oxygenation index and pediatric respiratory rate-oxygenation index variation in children. Eur J Pediatr [Internet]. 2021; 180(4): 1099–106. Available in: http://dx.doi.org/10.1007/s00431-020-03847-6 |
| [18] | Quesada-Arguedas D, Lin-Wu E, Quesada-Salas A, Navarro-Alvarado M. Respiratory Failure: types, pathophysiology and treatment: Acute Respiratory Failure: causes, pathophysiology and treatment. LATAM Latin American Journal of Social Sciences and Humanities [Internet]. 2023; 4(2). Available in: http://dx.doi.org/10.56712/latam.v4i2.853 |
[3, 7, 18]
.
In a study conducted by Vásquez et al, it was observed that the cut-off value of 4.88 was present in 9.43% of all failed therapies and in 16.2% of the remaining ones
| [8] | Vásquez-Hoyos P, Jiménez-Chaves A, Tovar-Velásquez M, Albor-Ortega R, Palencia M, Redondo-Pastrana D, et al. Factors associated with failure of high-flow nasal cannula therapy in pediatric patients with respiratory failure in two high-altitude pediatric critical care units. Med Intensiva (Engl Ed) [Internet]. 2021; 45(4): 195–204. Available in: http://dx.doi.org/10.1016/j.medin.2019.10.005 |
[8]
. This suggests that the cut-off values used in the original study (Roca et al) were not suitable for this pediatric population, which presents higher respiratory rates. Therefore, further research is required to confirm the validity of these cut-off values in pediatric cohorts
.
Regarding the area under the ROC curve (AUROC), we can infer that the ROX Index could have a less prominent role, remaining secondarily in comparison to the clinical scales evaluated in this study. Although some studies suggest that the ROX Index adequately predicts the outcome of HFNC use, others indicate the opposite. Therefore, it is not possible to make generalizations, and this should be considered as a tool that complements others
| [12] | Artacho-Ruiz R, Artacho-Jurado B, Caballero-Güeto F, Cano-Yuste A, Durbán-García I, García-Delgado F, et al. Predictors of success of high-flow nasal cannula treatment in hypoxemic acute respiratory failure. Med Intensiva [Internet]. 2021; 45(2): 80–7. Available in: http://dx.doi.org/10.1016/j.medin.2019.07.012 |
[12]
.
The primary advantage of this study lies in its prospective approach, which enabled greater control of the variables under study and contributed to minimizing the possibility of bias. Another additional strength is that it represents the first research carried out in an Ecuadorian pediatric hospital aiming to systematically evaluate the value of the ROX Index in predicting the failure of high-flow oxygen therapy in different patients.
As for limitations, firstly, there is the heterogeneity of the sample. Most studies focused on the ROX Index evaluate only one type of patients, mainly those diagnosed of pneumonia. The different design of our study, which includes various types of pathologies, could explain the limited performance according to the AUROC curve. A second limitation is finding the optimal cutoff point, as this is considered a challenge. Since measurements were taken at different time intervals in the present study, several cut-off points were obtained, representing a statistical limitation. Therefore, it would be preferable to maintain the same cut-off point for this purpose.
5. Conclusions
A higher proportion of younger infants was observed, as well as a prolongation in hospitalization time and an increase in mortality within the group of intubated patients. Furthermore, among those who did not respond satisfactorily to high-flow oxygen therapy, pneumonia was the predominant diagnosis.
Failure in the use of high-flow oxygen therapy not only prolongs hospital stay but also increases the need for endotracheal intubation. Identifying patients at risk should be a primary goal. For this reason, it is suggested that the ROX Index should be measured at 2 – 4 – 6 and 12 hours, since most patients who fail are intubated within 24 hours.
There is a wide variation in the literature regarding the best cut-off point for the ROX Index. At the moment, there is no universal agreement regarding the optimal cut-off point within the pediatric population. However, based on the data from this study, it is estimated that the cut-off point of 4.88, widely accepted in the literature, constitutes a predictor of success.
By having scales that assess the severity of respiratory failure according to the type of pathology, already validated in pediatrics, we can use the ROX Index as a complementary tool that strengthens decision-making instead of depending solely on it.
Abbreviations
ETI | Endotracheal Intubation |
HFNC | High-Flow Oxygen Therapy |
ROX INDEX | Respiratory Rate-Oxygenation Index |
Author Contributions
All authors contributed to the study conception and design.
Karla Calderón-Salavarría: Conceptualization, Material preparation, Data collection and Analysis.
Jimmy Barreiro-Casanova: Conceptualization, Resources and Methodology.
The first draft of the manuscript was written by Karla Calderón and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Declarations
This research adheres to rigorous ethical standards, prioritizing the protection of participants right. Additionally, it ensures that appropriate consent for publication has been obtained, thereby upholding transparency and integrity in disseminating the findings.
Code Availability
Data were analyzed using IBM SPSS Statistics for Windows, Version 20.0.
Ethics Approval and Consent to Participate
The forms and methodology for this study was approved by the Internal Review Board (IRB) of the Roberto Gilbert Elizalde Hospital. Informed consent was obtained from legal guardians.
Funding
This work is not supported by any external funding.
Data Availability Statement
The data that support the findings of this study are available within the paper and from the authors in forms. Restrictions apply to the availability of these forms, which were used under license from the Hospital Roberto Gilbert Elizalde for the current study, and so are not publicly available. Data shall be shared upon request.
Conflicts of Interest
The authors declare no conflicts of interest.
References
| [1] |
Silva-Guayasamín LG, Callejas D, Silva-Sarabia CA, Silva-Orozco GS. EPIDEMIOLOGICAL PROFILE OF ACUTE RESPIRATORY INFECTIONS IN PEDIATRIC PATIENTS IN ECUADOR. Enferm Investiga Investig Link Teaching Gest [Internet]. 2022; 7(2): 87–92. Available in:
http://dx.doi.org/10.31243/ei.uta.v7i2.1620.2022
|
| [2] |
Dulcey-Sarmiento LA, Castillo-Blanco JF, Theran-Leon JS, Caltagirone-Miceli R, Aguas-Cantillo MJ. Utility of the ROX Index as a Predictor of Respiratory Failure, Mortality and Complications in Patients with COVID-19 Without Invasive Ventilator Support, Unicentric Study [Internet]. Zenodo; 2022. Available in:
http://dx.doi.org/10.5281/ZENODO.6949776
|
| [3] |
Villanueva M, Alapont M. High flow oxygen in bronchiolitis. What if in the end it turns out not? Evid Pediatr. 2023; 19.
|
| [4] |
Chung-Engracia S, Cornejo-Briones C, López-Toledo M, Moreno-Castro F. Acute respiratory failure in pediatrics. [Internet]. 2022; 6(3): 166–74. Available in:
http://dx.doi.org/10.26820/recimundo/6.(3).junio.2022.166-174
|
| [5] |
Webb L, Chahine R, Aban I, Prabhakaran P, Loberger J. Predicting high-flow nasal cannula therapy outcomes using the ROX-HR index in the pediatric ICU. Respir Care [Internet]. 2022; respcare.09765. Available in:
http://dx.doi.org/10.4187/respcare.09765
|
| [6] |
Junhai Z, Jing Y, Beibei C, Li L. The value of ROX index in predicting the outcome of high flow nasal cannula: a systematic review and meta-analysis. Breathe Res [Internet]. 2022; 23(1). Available in:
http://dx.doi.org/10.1186/s12931-022-01951-9
|
| [7] |
Yildizdas D, Yontem A, Iplik G, Horoz OO, Ekinci F. Predicting nasal high-flow therapy failure by pediatric respiratory rate-oxygenation index and pediatric respiratory rate-oxygenation index variation in children. Eur J Pediatr [Internet]. 2021; 180(4): 1099–106. Available in:
http://dx.doi.org/10.1007/s00431-020-03847-6
|
| [8] |
Vásquez-Hoyos P, Jiménez-Chaves A, Tovar-Velásquez M, Albor-Ortega R, Palencia M, Redondo-Pastrana D, et al. Factors associated with failure of high-flow nasal cannula therapy in pediatric patients with respiratory failure in two high-altitude pediatric critical care units. Med Intensiva (Engl Ed) [Internet]. 2021; 45(4): 195–204. Available in:
http://dx.doi.org/10.1016/j.medin.2019.10.005
|
| [9] |
Roca O, Messika J, Caralt B, García-de-Acilu M, Sztrymf B, Ricard JD, et al. Predicting success of high-flow nasal cannula in pneumonia patients with hypoxemic respiratory failure: The utility of the ROX index. J Crit Care [Internet]. 2016; 35: 200–5. Available in:
http://dx.doi.org/10.1016/j.jcrc.2016.05.022
|
| [10] |
Goh K, Chai H, Ong T, Sewa D, Phua G, Tan Q. Early prediction of high flow nasal cannula therapy outcomes using a modified ROX index incorporating heart rate. J Intensive Care [Internet]. 2020; 8(1). Available in:
http://dx.doi.org/10.1186/s40560-020-00458-z
|
| [11] |
Pastor D, Tarazona S, Rodríguez-Cimadevilla J. Acute and chronic respiratory failure. Oxygen therapy [Internet]. 2017; 1: 369-399. Aeped.es. Available at:
https://www.aeped.es/sites/default/files/documentos/23_fracaso_respiratorio.pdf
|
| [12] |
Artacho-Ruiz R, Artacho-Jurado B, Caballero-Güeto F, Cano-Yuste A, Durbán-García I, García-Delgado F, et al. Predictors of success of high-flow nasal cannula treatment in hypoxemic acute respiratory failure. Med Intensiva [Internet]. 2021; 45(2): 80–7. Available in:
http://dx.doi.org/10.1016/j.medin.2019.07.012
|
| [13] |
Salvatico E, Storaccio S, Ulloa A, Prado S, Diaz M. High flow oxygen therapy (HFO) in pediatrics. An innovative experience. Sick notes (Córdoba) [Internet]. 2017; 23–8. Available in:
https://pesquisa.bvsalud.org/portal/resource/pt/biblio-907856
|
| [14] |
Chang C, Lin Y, Chen T, Lin J, Hsia S, Chan O, et al. High-flow nasal cannula therapy in children with acute respiratory distress with hypoxia in A pediatric intensive care unit–A single center experience. Front Pediatr [Internet]. 2021; 9. Available in:
http://dx.doi.org/10.3389/fped.2021.664180
|
| [15] |
Mendoza B. Respiratory failure in pediatrics. Concepts of Pediatric Respiratory Care. Santiago de Cali University Editorial. [Internet]. 2021. Pp. 79-94. Edu.co. Available at:
https://libros.usc.edu.co/index.php/usc/catalog/download/279/394/5967?inline=1
|
| [16] |
Casares H. Respiratory distress in pediatrics in the emergency [Internet]. 2023. Vol VI. 79-109. Npunto.es. Available in:
https://www.npunto.es/content/src/pdf-articulo/63d9340a1883fart4.pdf
|
| [17] |
Roca O, Caralt B, Messika J, Samper M, Sztrymf B, Hernández G, et al. An index combining respiratory rate and oxygenation to predict outcome of nasal high-flow therapy. Am J Respir Crit Care Med [Internet]. 2019; 199(11): 1368–76. Available at:
http://dx.doi.org/10.1164/rccm.201803-0589oc
|
| [18] |
Quesada-Arguedas D, Lin-Wu E, Quesada-Salas A, Navarro-Alvarado M. Respiratory Failure: types, pathophysiology and treatment: Acute Respiratory Failure: causes, pathophysiology and treatment. LATAM Latin American Journal of Social Sciences and Humanities [Internet]. 2023; 4(2). Available in:
http://dx.doi.org/10.56712/latam.v4i2.853
|
| [19] |
Ricard J, Roca O, Lemiale V, Corley A, Braunlich J, Jones P, et al. Use of nasal high flow oxygen during acute respiratory failure. Intensive Care Med [Internet]. 2020; 46(12): 2238–47. Available in:
http://dx.doi.org/10.1007/s00134-020-06228-7
|
| [20] |
Pilar-Orive F, López-Fernández Y. High flow [Internet]. 2021; 1: 235-43. Aeped.es. Available in:
https://www.aeped.es/sites/default/files/documentos/18_alto_flujo
|
Cite This Article
-
APA Style
Calderón-Salavarría, K., Barreiro-Casanova, J. (2024). Application of the Rox Index as a Predictor of Respiratory Failure in Pediatric Patients Receiving High-Flow Oxygen Therapy Support at the Roberto Gilbert Elizalde Hospital. American Journal of Pediatrics, 10(2), 96-106. https://doi.org/10.11648/j.ajp.20241002.17
 Copy
|
Copy
|
 Download
Download
ACS Style
Calderón-Salavarría, K.; Barreiro-Casanova, J. Application of the Rox Index as a Predictor of Respiratory Failure in Pediatric Patients Receiving High-Flow Oxygen Therapy Support at the Roberto Gilbert Elizalde Hospital. Am. J. Pediatr. 2024, 10(2), 96-106. doi: 10.11648/j.ajp.20241002.17
Copy
|
Download
AMA Style
Calderón-Salavarría K, Barreiro-Casanova J. Application of the Rox Index as a Predictor of Respiratory Failure in Pediatric Patients Receiving High-Flow Oxygen Therapy Support at the Roberto Gilbert Elizalde Hospital. Am J Pediatr. 2024;10(2):96-106. doi: 10.11648/j.ajp.20241002.17
Copy
|
Download
-
@article{10.11648/j.ajp.20241002.17,
author = {Karla Calderón-Salavarría and Jimmy Barreiro-Casanova},
title = {Application of the Rox Index as a Predictor of Respiratory Failure in Pediatric Patients Receiving High-Flow Oxygen Therapy Support at the Roberto Gilbert Elizalde Hospital
},
journal = {American Journal of Pediatrics},
volume = {10},
number = {2},
pages = {96-106},
doi = {10.11648/j.ajp.20241002.17},
url = {https://doi.org/10.11648/j.ajp.20241002.17},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ajp.20241002.17},
abstract = {Background: High-flow oxygen therapy is an ideal treatment for managing respiratory failure. It avoids orotracheal intubation; however, some patients are refractory to this treatment. The ROX Index aims to detect early failure in high-flow oxygen therapy; nevertheless, its use has been poorly studied in pediatrics. Objective: To evaluate the applicability of the ROX Index as a tool to determine the failure of high-flow oxygen therapy in pediatric patients admitted to the Roberto Gilbert Hospital. Methodology: Observational, prospective, longitudinal cohort study with a descriptive approach including 209 patients between 1 month and 17 years old who required high-flow oxygen therapy within the first 24 hours. ROX Index measurements were taken at 2, 4, 6, 12, and 24 hours with follow-up to determine the outcome. Result: A total of 209 patients meeting the inclusion criteria were obtained; 27 (12.9%) required endotracheal intubation (ETI), and 182 (87%) received high-flow oxygen therapy (HFNC). A higher frequency of younger infants was observed among patients who required ETI, with a median age of 12 months. A significant difference in the ROX index was found from two hours onwards with cutoff points on the AUROC curve above 0.5. Conclusion: It was determined that the ROX Index can be used as a complementary tool to strengthen decision-making in pediatrics.
},
year = {2024}
}
Copy
|
Download
-
TY - JOUR
T1 - Application of the Rox Index as a Predictor of Respiratory Failure in Pediatric Patients Receiving High-Flow Oxygen Therapy Support at the Roberto Gilbert Elizalde Hospital
AU - Karla Calderón-Salavarría
AU - Jimmy Barreiro-Casanova
Y1 - 2024/05/30
PY - 2024
N1 - https://doi.org/10.11648/j.ajp.20241002.17
DO - 10.11648/j.ajp.20241002.17
T2 - American Journal of Pediatrics
JF - American Journal of Pediatrics
JO - American Journal of Pediatrics
SP - 96
EP - 106
PB - Science Publishing Group
SN - 2472-0909
UR - https://doi.org/10.11648/j.ajp.20241002.17
AB - Background: High-flow oxygen therapy is an ideal treatment for managing respiratory failure. It avoids orotracheal intubation; however, some patients are refractory to this treatment. The ROX Index aims to detect early failure in high-flow oxygen therapy; nevertheless, its use has been poorly studied in pediatrics. Objective: To evaluate the applicability of the ROX Index as a tool to determine the failure of high-flow oxygen therapy in pediatric patients admitted to the Roberto Gilbert Hospital. Methodology: Observational, prospective, longitudinal cohort study with a descriptive approach including 209 patients between 1 month and 17 years old who required high-flow oxygen therapy within the first 24 hours. ROX Index measurements were taken at 2, 4, 6, 12, and 24 hours with follow-up to determine the outcome. Result: A total of 209 patients meeting the inclusion criteria were obtained; 27 (12.9%) required endotracheal intubation (ETI), and 182 (87%) received high-flow oxygen therapy (HFNC). A higher frequency of younger infants was observed among patients who required ETI, with a median age of 12 months. A significant difference in the ROX index was found from two hours onwards with cutoff points on the AUROC curve above 0.5. Conclusion: It was determined that the ROX Index can be used as a complementary tool to strengthen decision-making in pediatrics.
VL - 10
IS - 2
ER -
Copy
|
Download