Background: Subtrochanteric femoral fractures are unstable injuries characterized by high mechanical stress, cortical bone predominance and an increased risk of fixation failure. Optimal implant selection remains controversial, particularly for unstable fracture patterns. This study aimed to compare the outcomes of proximal femoral nailing and locking plate fixation in the management of closed subtrochanteric femoral fractures. Methods: This comparative study was conducted at the Department of Orthopaedics, President Abdul Hamid Medical College Hospital, Kishoreganj, Bangladesh, from January to December 2025. Fifty adult patients with closed subtrochanteric femoral fractures were divided into two groups: proximal femoral nailing (PFN, n=25) and proximal femoral locking plate fixation (PFLP, n=25). Intraoperative parameters, postoperative recovery, radiological union, functional outcomes using the Harris Hip Score and complications were evaluated. Statistical analysis was performed using SPSS version 25.0, with significance set at p<0.05. Results: The mean operative time was significantly shorter in the proximal femoral nailing group (85.4 ± 12.5 min) than in the locking plate group (110.6 ± 15.3 min). Intraoperative blood loss was lower with nailing (180 ± 40 mL vs. 270 ± 60 mL). Time to partial weight bearing (4.8 ± 1.2 vs. 6.2 ± 1.6 weeks) and radiological union (17.6 ± 3.1 vs. 20.8 ± 3.7 weeks) were significantly earlier with nailing. Mean Harris Hip Score was higher following nailing (83.5 ± 6.4 vs 77.2 ± 7.8). Conclusion: Proximal femoral nailing provides superior operative efficiency, faster recovery and improved functional outcomes compared with proximal femoral locking plate fixation.
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited.
Subtrochanteric femoral fractures constitute a complex group of proximal femoral injuries characterized by high biomechanical stress and a strong tendency toward instability
[1]
Panteli M, Giannoudi MP, Lodge CJ, West RM, Pountos I, Giannoudis PV. Mortality and medical complications of subtrochanteric fracture fixation. Journal of Clinical Medicine. 2021 Feb 2; 10(3): 540.
[1]
. These fractures typically occur within 5 cm distal to the lesser trochanter and are associated with substantial deforming forces from surrounding musculature, leading to difficulties in achieving and maintaining reduction
[2]
Bhandari M, Swiontkowski M. Management of acute hip fracture. New England Journal of Medicine. 2017 Nov 23; 377(21): 2053-62.
[2]
. They commonly result from high-energy trauma in younger individuals and low-energy falls in elderly patients with osteoporotic bone, contributing to significant morbidity and prolonged functional impairment
[3]
Attum B, Pilson H. Intertrochanteric Femur Fracture. [Updated 2023 Aug 8]. In: StatPearls. Treasure Island (FL): StatPearls Publishing; 2025 Jan-. Available from:
The management of subtrochanteric fractures is primarily surgical, with the objectives of restoring anatomical alignment, achieving stable fixation and facilitating early mobilization
[4]
Chang SM, Hou ZY, Hu SJ, Du SC. Intertrochanteric femur fracture treatment in Asia: what we know and what the world can learn. Orthopedic Clinics. 2020 Apr 1; 51(2): 189-205.
[4]
. However, the unique anatomical and biomechanical characteristics of this region, including dense cortical bone and limited vascular supply, predispose these fractures to delayed union, non-union and implant-related complications
[5]
Meinberg EG, Agel J, Roberts CS, Karam MD, Kellam JF. Fracture and dislocation classification compendium—2018. Journal of orthopaedic trauma. 2018 Jan 1; 32: S1-0.
[5]
. Consequently, the choice of fixation device remains a subject of ongoing debate.
Intramedullary devices, particularly proximal femoral nails, have gained widespread acceptance due to their load-sharing properties, reduced bending moments and minimally invasive insertion technique
[6]
Yu X, Wang H, Duan X, Liu M, Xiang Z. Intramedullary versus extramedullary internal fixation for unstable intertrochanteric fracture, a meta-analysis. Acta orthopaedica et traumatologica turcica. 2018 Jul 1; 52(4): 299-307.
[6]
. Several studies have reported shorter operative time, reduced blood loss and earlier weight bearing with proximal femoral nailing, especially in unstable fracture patterns
[7]
Pradhan V, Jain S, Agrawal S, Sharma SL. Comparative prospective study of proximal femoral nail and locking compression plate in subtrochanteric fractures of femur. Natl J Clin Orthop. 2018; 2(4): 188-94.
[8]
Roy S, Banik R. A comparative study between proximal femoral nail and proximal femoral locking plate in subtrochanteric femoral fractures: A prospective analysis of 36 cases. International Journal of Orthopaedics. 2019; 5(3): 815-21.
[7, 8]
. These advantages are attributed to the biomechanical superiority of intramedullary fixation, which aligns closer to the mechanical axis of the femur
[9]
Zeelenberg ML, Plaisier AC, Nugteren LH, Loggers SA, Joosse P, Verhofstad MH, Den Hartog D, Van Lieshout EM, STABLE-HIP Study Group Gosens Taco Hegeman Johannes H. Polinder Suzanne Poolman Rudolf W. Willems Hanna C. Zuurmond Rutger G. Extramedullary versus intramedullary fixation of unstable trochanteric femoral fractures (AO type 31-A2): a systematic review and meta-analysis. Archives of orthopaedic and trauma surgery. 2024 Mar; 144(3): 1189-209.
[9]
.
In contrast, proximal femoral locking plates represent an extramedullary fixation option that provides angular stability and allows controlled fracture reduction under direct visualization
[10]
Vinay N, Sain A. Comparative evaluation of clinico-radiological and functional outcome of proximal femoral locking compression plate and proximal femoral nail in unstable proximal femoral fractures. Int J Orthop Sci. 2016; 2: 103-7.
[10]
. Locking plate constructs have been advocated in fractures with complex morphology, narrow medullary canals, or when intramedullary fixation is technically challenging
[11]
Kumar DY, Harshwardhan DH. Comparison of proximal femur locking compression plate and proximal femur nail in treatment of complex proximal femoral fractures. Int J Orthop Sci. 2018; 4(2c): 164-8.
[11]
. Despite these theoretical advantages, multiple studies have reported higher rates of implant failure, delayed union and reoperation with locking plates, particularly in osteoporotic bone and unstable fracture configurations
[12]
He S, Yan B, Zhu J, Huang X, Zhao J. High failure rate of proximal femoral locking plates in fixation of trochanteric fractures. Journal of Orthopaedic Surgery and Research. 2018 Oct 5; 13(1): 248.
[12]
.
Previous comparative studies evaluating proximal femoral nailing and proximal femoral locking plate fixation have demonstrated inconsistent results. While some authors have shown superior functional outcomes and faster fracture union with intramedullary nails, others have reported comparable clinical and radiological outcomes between the two methods
[13]
Mirbolook A, Siavashi B, Jafarinezhad AE, Khajeh Jahromi S, Farahmand M, Roohi Rad M, Kahe MA. Subtrochanteric fractures: comparison of proximal femur locking plate and intramedullary locking nail fixation outcome. Indian Journal of Surgery. 2015 Dec; 77(Suppl 3): 795-8.
[14]
Nirup NC, Reddy VN. A prospective comparative study of subtrochanteric fractures treated with long proximal femur nail and proximal femur locking plate. Int J Sci Res. 2019; 8(9): 62-5.
[13, 14]
. Variations in patient demographics, fracture patterns, surgical technique and follow-up duration contribute to these discrepancies.
Furthermore, data from low- and middle-income countries remain limited, particularly from secondary-level teaching hospitals where resource availability, implant cost and surgical expertise may influence outcomes. There is a need for region-specific evidence to guide implant selection and optimize patient care.
Therefore, the present study aimed to compare proximal femoral nailing and proximal femoral locking plate fixation in the treatment of closed subtrochanteric femoral fractures, focusing on intraoperative parameters, postoperative recovery, functional outcomes and complication profiles.
2. Materials & Methods
2.1. Methodology
This comparative observational study was conducted in the Department of Orthopaedics, President Abdul Hamid Medical College Hospital, Kishoreganj, Dhaka, Bangladesh, from January to December 2025. A total of 50 adult patients with closed subtrochanteric femoral fractures were included. Patients were equally allocated into two groups: proximal femoral nailing (PFN, n=25) and proximal femoral locking plate fixation (PFLP, n=25).
All eligible patients were evaluated at admission using a standardized proforma. Baseline demographic data, injury mechanism, fracture side and fracture classification were recorded. Radiological assessment included anteroposterior and lateral radiographs of the affected femur. Surgical fixation was performed by experienced orthopedic surgeons using either PFN or PFLP based on preoperative planning and implant availability. Intraoperative parameters such as operative time, blood loss, fluoroscopy exposure and need for open reduction were documented. Postoperatively, patients followed a standardized rehabilitation protocol. Clinical and radiological follow-up was conducted at regular intervals to assess fracture healing, time to weight bearing, complications and functional outcomes. Functional assessment was performed using the Harris Hip Score at six months. Informed consent was secured from all participants and patient confidentiality was strictly maintained throughout the study.
2.4. Statistical Analysis
Data were analyzed using SPSS version 25.0. Continuous variables were expressed as mean ± standard deviation and compared using independent sample t-tests. Categorical variables were analyzed using chi-square or Fisher’s exact test. A p-value less than 0.05 was considered statistically significant.
3. Results
Table 1 shows baseline characteristics of 50 patients. Mean age was similar in the PFN and PFLP groups (54.6 ± 10.2 vs 55.8 ± 9.6 years). Males constituted the majority in both groups (64% vs 60%). Right-sided fractures were more common (54%). Road traffic accidents were the main cause of injury (58%). AO Type C fractures were most frequent (40%), followed by Type B (38%) and Type A (22%), with comparable distribution between groups.
Table 1. Baseline Demographic and Clinical Characteristics of Patients (n = 50).
Characteristics
PFN Group (n=25)
PFLP Group (n=25)
Total (n=50)
Age (years)
54.6 ± 10.2
55.8 ± 9.6
55.2 ± 9.9
Gender
Male
16 (64%)
15 (60%)
31 (62%)
Female
9 (36%)
10 (40%)
19 (38%)
Side of Fracture
Right
13 (52%)
14 (56%)
27 (54%)
Left
12 (48%)
11 (44%)
23 (46%)
Mode of Injury
Road Traffic Accident
15 (60%)
14 (56%)
29 (58%)
Fall from Height
8 (32%)
9 (36%)
17 (34%)
Others (e.g., slip)
2 (8%)
2 (8%)
4 (8%)
Fracture Pattern (AO Classification)
Type A
6 (24%)
5 (20%)
11 (22%)
Type B
10 (40%)
9 (36%)
19 (38%)
Type C
9 (36%)
11 (44%)
20 (40%)
Table 2. Intraoperative Characteristics of PFN and PFLP Fixation.
Parameter
PFN Group (Mean ± SD)
PFLP Group (Mean ± SD)
p-value
Duration of Surgery (minutes)
85.4 ± 12.5
110.6 ± 15.3
<0.001
Intraoperative Blood Loss (mL)
180 ± 40
270 ± 60
<0.001
Fluoroscopy Exposure (seconds)
58 ± 10
42 ± 8
<0.001
Need for Open Reduction
5 (20%)
13 (52%)
0.019
Mean Hospital Stay (days)
7.2 ± 2.1
9.4 ± 2.8
0.002
Table 2 presents intraoperative parameters. Mean operative time was shorter in the PFN group (85.4 ± 12.5 vs 110.6 ± 15.3 minutes). Blood loss was lower with PFN (180 ± 40 vs 270 ± 60 mL). Fluoroscopy time was higher in the PFN group (58 ± 10 vs 42 ± 8 seconds). Open reduction was required in 20% of PFN cases and 52% of PFLP cases. Hospital stay was shorter following PFN (7.2 ± 2.1 vs 9.4 ± 2.8 days).
Table 3. Postoperative and Functional Outcomes Following PFN and PFLP Fixation.
Outcome Parameter
PFN Group (n=25)
PFLP Group (n=25)
p-value
Time to Partial Weight Bearing (weeks)
4.8 ± 1.2
6.2 ± 1.6
0.001
Time to Radiological Union (weeks)
17.6 ± 3.1
20.8 ± 3.7
0.001
Varus Collapse (>5°)
2 (8%)
5 (20%)
0.226
Limb Length Discrepancy (>1 cm)
1 (4%)
3 (12%)
0.3
Mean Harris Hip Score at 6 Months
83.5 ± 6.4
77.2 ± 7.8
0.003
Excellent/Good Results (HHS ≥ 80)
19 (76%)
13 (52%)
0.08
Table 3 describes postoperative outcomes. Time to partial weight bearing was earlier in the PFN group (4.8 ± 1.2 vs 6.2 ± 1.6 weeks). Radiological union occurred sooner with PFN (17.6 ± 3.1 vs 20.8 ± 3.7 weeks). Mean Harris Hip Score at six months was higher in the PFN group (83.5 ± 6.4 vs 77.2 ± 7.8). Excellent or good outcomes were achieved in 76% of PFN patients and 52% of PFLP patients.
Table 4. Comparison of Postoperative Complications Between PFN and PFLP Groups.
Complication
PFN Group (n=25)
PFLP Group (n=25)
Total (%)
Superficial Infection
1 (4%)
3 (12%)
4 (8%)
Deep Infection
0 (0%)
1 (4%)
1 (2%)
Implant Failure
1 (4%)
3 (12%)
4 (8%)
Delayed Union
2 (8%)
4 (16%)
6 (12%)
Non-union
0 (0%)
2 (8%)
2 (4%)
Reoperation
1 (4%)
2 (8%)
3 (6%)
Table 4 summarizes complications. Superficial infection occurred in 4% of PFN and 12% of PFLP patients. Implant failure was seen in 4% and 12%, respectively. Delayed union occurred in 8% of PFN and 16% of PFLP patients. Non-union and reoperation were more frequent in the PFLP group. Overall, complications were fewer in the PFN group.
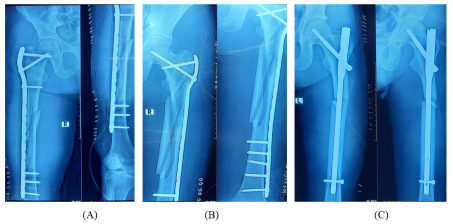
Figure 3. post-operative radiographs showing internal fixation of subtrochanteric fractures using a Proximal Femoral Locking Plate (PFLP) and Proximal Femoral Nailing (PFN).
4. Discussion
Subtrochanteric femoral fractures remain one of the most demanding injuries in orthopedic trauma due to high biomechanical stresses, unstable fracture patterns and a tendency toward fixation failure. The present comparative observational study evaluated proximal femoral nailing and proximal femoral locking plate fixation for closed subtrochanteric fractures and demonstrated meaningful differences in intraoperative parameters, postoperative recovery and functional outcomes, thereby contributing clinically relevant evidence to an ongoing debate.
In this study, proximal femoral nailing was associated with significantly shorter operative time and reduced intraoperative blood loss compared with proximal femoral locking plate fixation. These findings are consistent with those reported by Pradhan et al., who observed that intramedullary fixation minimizes surgical exposure and preserves soft tissue integrity, leading to improved operative efficiency
[7]
Pradhan V, Jain S, Agrawal S, Sharma SL. Comparative prospective study of proximal femoral nail and locking compression plate in subtrochanteric fractures of femur. Natl J Clin Orthop. 2018; 2(4): 188-94.
[7]
. Roy et al. similarly reported shorter surgical duration with proximal femoral nailing, attributing this to the percutaneous technique and reduced need for fracture manipulation
[8]
Roy S, Banik R. A comparative study between proximal femoral nail and proximal femoral locking plate in subtrochanteric femoral fractures: A prospective analysis of 36 cases. International Journal of Orthopaedics. 2019; 5(3): 815-21.
[8]
. In contrast, locking plate fixation often requires extensive dissection and precise plate contouring, which may prolong operative time.
The need for open reduction was significantly higher in the locking plate group, a finding also reported by He et al., who noted that indirect reduction is frequently insufficient when using extramedullary implants in unstable fracture configurations
[12]
He S, Yan B, Zhu J, Huang X, Zhao J. High failure rate of proximal femoral locking plates in fixation of trochanteric fractures. Journal of Orthopaedic Surgery and Research. 2018 Oct 5; 13(1): 248.
[12]
. Increased surgical exposure may partly explain the significantly longer hospital stay observed among patients treated with proximal femoral locking plates. Mirbolook et al. demonstrated that prolonged operative time and soft tissue disruption were associated with delayed postoperative recovery and extended hospitalization
[13]
Mirbolook A, Siavashi B, Jafarinezhad AE, Khajeh Jahromi S, Farahmand M, Roohi Rad M, Kahe MA. Subtrochanteric fractures: comparison of proximal femur locking plate and intramedullary locking nail fixation outcome. Indian Journal of Surgery. 2015 Dec; 77(Suppl 3): 795-8.
[13]
.
Postoperative recovery parameters favored proximal femoral nailing in the present study. Time to partial weight bearing was significantly shorter in the nailing group, reflecting the biomechanical stability of intramedullary fixation. Nirup and Reddy reported similar findings, emphasizing that load-sharing implants facilitate earlier mobilization and reduce complications related to prolonged immobilization
[14]
Nirup NC, Reddy VN. A prospective comparative study of subtrochanteric fractures treated with long proximal femur nail and proximal femur locking plate. Int J Sci Res. 2019; 8(9): 62-5.
[14]
. Early weight bearing is particularly important in elderly patients to prevent deconditioning and systemic complications.
Radiological union occurred significantly earlier in the proximal femoral nailing group. Yu et al. explained that intramedullary devices align closer to the mechanical axis of the femur, reducing bending moments at the fracture site and promoting callus formation
[6]
Yu X, Wang H, Duan X, Liu M, Xiang Z. Intramedullary versus extramedullary internal fixation for unstable intertrochanteric fracture, a meta-analysis. Acta orthopaedica et traumatologica turcica. 2018 Jul 1; 52(4): 299-307.
[6]
. In contrast, extramedullary fixation creates a longer lever arm, increasing mechanical strain and potentially delaying fracture healing. These biomechanical principles are particularly relevant in subtrochanteric fractures, where cortical bone predominates.
Functional outcomes assessed using the Harris Hip Score at six months were significantly better in the proximal femoral nailing group. Singh et al. reported superior functional recovery following intramedullary fixation, attributing improved outcomes to early mobilization and stable fixation
[15]
Singh AK, Narsaria N, G RA SV. Treatment of unstable trochanteric femur fractures: proximal femur nail versus proximal femur locking compression plate. Am J Orthop (Belle Mead NJ). 2017 Mar 1; 46(2): E116-23.
[15]
. Although the proportion of excellent or good results was higher with proximal femoral nailing, this difference did not reach statistical significance, suggesting that both implants can achieve acceptable long-term function when union is achieved.
Complication analysis revealed numerically higher rates of implant failure, delayed union and non-union in the locking plate group. He et al. reported a high failure rate of proximal femoral locking plates, particularly in osteoporotic bone, due to stress concentration at the plate–bone interface
[12]
He S, Yan B, Zhu J, Huang X, Zhao J. High failure rate of proximal femoral locking plates in fixation of trochanteric fractures. Journal of Orthopaedic Surgery and Research. 2018 Oct 5; 13(1): 248.
[12]
. Yu et al. further highlighted that extramedullary implants are more susceptible to mechanical failure under cyclical loading
[6]
Yu X, Wang H, Duan X, Liu M, Xiang Z. Intramedullary versus extramedullary internal fixation for unstable intertrochanteric fracture, a meta-analysis. Acta orthopaedica et traumatologica turcica. 2018 Jul 1; 52(4): 299-307.
[6]
. Although statistical significance was not observed in the present study, the trend is clinically important and aligns with previously published literature.
Recent systematic reviews and meta-analyses further support the preferential use of intramedullary fixation. Zeelenberg et al. demonstrated lower rates of mechanical failure and improved functional outcomes with intramedullary devices compared with extramedullary fixation for unstable proximal femoral fractures
[9]
Zeelenberg ML, Plaisier AC, Nugteren LH, Loggers SA, Joosse P, Verhofstad MH, Den Hartog D, Van Lieshout EM, STABLE-HIP Study Group Gosens Taco Hegeman Johannes H. Polinder Suzanne Poolman Rudolf W. Willems Hanna C. Zuurmond Rutger G. Extramedullary versus intramedullary fixation of unstable trochanteric femoral fractures (AO type 31-A2): a systematic review and meta-analysis. Archives of orthopaedic and trauma surgery. 2024 Mar; 144(3): 1189-209.
[9]
. Similarly, the Cochrane review by Lewis et al. concluded that cephalomedullary nails offer biomechanical advantages and facilitate earlier mobilization
[16]
Lewis SR, Macey R, Gill JR, Parker MJ, Griffin XL. Cephalomedullary nails versus extramedullary implants for extracapsular hip fractures in older adults. Cochrane Database of Systematic Reviews. 2022(1).
[16]
.
In resource-limited healthcare settings, the reduced operative time, shorter hospital stays and faster rehabilitation associated with proximal femoral nailing may translate into significant clinical and economic benefits. Overall, the findings of this study reinforce existing evidence that proximal femoral nailing provides superior outcomes compared with proximal femoral locking plate fixation in the management of closed subtrochanteric femoral fractures.
5. Limitations and Recommendations
The study was limited by a modest sample size and short follow-up duration. Future multicenter randomized studies with longer follow-up are recommended to validate these findings and assess long-term functional and implant-related outcomes.
6. Conclusion
Proximal femoral nailing demonstrated superior intraoperative efficiency, earlier mobilization, faster fracture union and better functional outcomes compared with proximal femoral locking plate fixation. These findings support the preferential use of intramedullary fixation for closed subtrochanteric femoral fractures, particularly in unstable patterns, to optimize clinical recovery and reduce complication risk.
Abbreviations
PFN
Proximal Femoral Nailing
PFLP
Proximal Femoral Locking Plate Fixation
SPSS
Statistical Package for the Social Sciences
Author Contributions
Avishek Bhadra: Conceptualization, Supervision, Resources, Writing – original draft.
Gulam Mustofa: Methodology, Data curation, Investigation.
Zahid Hasan Hemal: Formal analysis, Software, Validation.
Sabbir Ahmed: Data curation, Visualization, Writing – review & editing.
Panteli M, Giannoudi MP, Lodge CJ, West RM, Pountos I, Giannoudis PV. Mortality and medical complications of subtrochanteric fracture fixation. Journal of Clinical Medicine. 2021 Feb 2; 10(3): 540.
[2]
Bhandari M, Swiontkowski M. Management of acute hip fracture. New England Journal of Medicine. 2017 Nov 23; 377(21): 2053-62.
[3]
Attum B, Pilson H. Intertrochanteric Femur Fracture. [Updated 2023 Aug 8]. In: StatPearls. Treasure Island (FL): StatPearls Publishing; 2025 Jan-. Available from:
Chang SM, Hou ZY, Hu SJ, Du SC. Intertrochanteric femur fracture treatment in Asia: what we know and what the world can learn. Orthopedic Clinics. 2020 Apr 1; 51(2): 189-205.
[5]
Meinberg EG, Agel J, Roberts CS, Karam MD, Kellam JF. Fracture and dislocation classification compendium—2018. Journal of orthopaedic trauma. 2018 Jan 1; 32: S1-0.
[6]
Yu X, Wang H, Duan X, Liu M, Xiang Z. Intramedullary versus extramedullary internal fixation for unstable intertrochanteric fracture, a meta-analysis. Acta orthopaedica et traumatologica turcica. 2018 Jul 1; 52(4): 299-307.
[7]
Pradhan V, Jain S, Agrawal S, Sharma SL. Comparative prospective study of proximal femoral nail and locking compression plate in subtrochanteric fractures of femur. Natl J Clin Orthop. 2018; 2(4): 188-94.
[8]
Roy S, Banik R. A comparative study between proximal femoral nail and proximal femoral locking plate in subtrochanteric femoral fractures: A prospective analysis of 36 cases. International Journal of Orthopaedics. 2019; 5(3): 815-21.
[9]
Zeelenberg ML, Plaisier AC, Nugteren LH, Loggers SA, Joosse P, Verhofstad MH, Den Hartog D, Van Lieshout EM, STABLE-HIP Study Group Gosens Taco Hegeman Johannes H. Polinder Suzanne Poolman Rudolf W. Willems Hanna C. Zuurmond Rutger G. Extramedullary versus intramedullary fixation of unstable trochanteric femoral fractures (AO type 31-A2): a systematic review and meta-analysis. Archives of orthopaedic and trauma surgery. 2024 Mar; 144(3): 1189-209.
[10]
Vinay N, Sain A. Comparative evaluation of clinico-radiological and functional outcome of proximal femoral locking compression plate and proximal femoral nail in unstable proximal femoral fractures. Int J Orthop Sci. 2016; 2: 103-7.
[11]
Kumar DY, Harshwardhan DH. Comparison of proximal femur locking compression plate and proximal femur nail in treatment of complex proximal femoral fractures. Int J Orthop Sci. 2018; 4(2c): 164-8.
[12]
He S, Yan B, Zhu J, Huang X, Zhao J. High failure rate of proximal femoral locking plates in fixation of trochanteric fractures. Journal of Orthopaedic Surgery and Research. 2018 Oct 5; 13(1): 248.
[13]
Mirbolook A, Siavashi B, Jafarinezhad AE, Khajeh Jahromi S, Farahmand M, Roohi Rad M, Kahe MA. Subtrochanteric fractures: comparison of proximal femur locking plate and intramedullary locking nail fixation outcome. Indian Journal of Surgery. 2015 Dec; 77(Suppl 3): 795-8.
[14]
Nirup NC, Reddy VN. A prospective comparative study of subtrochanteric fractures treated with long proximal femur nail and proximal femur locking plate. Int J Sci Res. 2019; 8(9): 62-5.
[15]
Singh AK, Narsaria N, G RA SV. Treatment of unstable trochanteric femur fractures: proximal femur nail versus proximal femur locking compression plate. Am J Orthop (Belle Mead NJ). 2017 Mar 1; 46(2): E116-23.
[16]
Lewis SR, Macey R, Gill JR, Parker MJ, Griffin XL. Cephalomedullary nails versus extramedullary implants for extracapsular hip fractures in older adults. Cochrane Database of Systematic Reviews. 2022(1).
Bhadra, A., Mustofa, G., Hemal, Z. H., Ahmed, S., Rahman, A. (2026). Comparison Between Proximal Femoral Nailing and Proximal Femoral Locking Plate in Closed Subtrochanteric Fracture. American Journal of Orthopaedics and Traumatology, 1(1), 20-26. https://doi.org/10.11648/j.ajot.20260101.14
Bhadra A, Mustofa G, Hemal ZH, Ahmed S, Rahman A. Comparison Between Proximal Femoral Nailing and Proximal Femoral Locking Plate in Closed Subtrochanteric Fracture. Am J Orthop Traumatol. 2026;1(1):20-26. doi: 10.11648/j.ajot.20260101.14
@article{10.11648/j.ajot.20260101.14,
author = {Avishek Bhadra and Gulam Mustofa and Zahid Hasan Hemal and Sabbir Ahmed and Ashikur Rahman},
title = {Comparison Between Proximal Femoral Nailing and Proximal Femoral Locking Plate in Closed Subtrochanteric Fracture},
journal = {American Journal of Orthopaedics and Traumatology},
volume = {1},
number = {1},
pages = {20-26},
doi = {10.11648/j.ajot.20260101.14},
url = {https://doi.org/10.11648/j.ajot.20260101.14},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ajot.20260101.14},
abstract = {Background: Subtrochanteric femoral fractures are unstable injuries characterized by high mechanical stress, cortical bone predominance and an increased risk of fixation failure. Optimal implant selection remains controversial, particularly for unstable fracture patterns. This study aimed to compare the outcomes of proximal femoral nailing and locking plate fixation in the management of closed subtrochanteric femoral fractures. Methods: This comparative study was conducted at the Department of Orthopaedics, President Abdul Hamid Medical College Hospital, Kishoreganj, Bangladesh, from January to December 2025. Fifty adult patients with closed subtrochanteric femoral fractures were divided into two groups: proximal femoral nailing (PFN, n=25) and proximal femoral locking plate fixation (PFLP, n=25). Intraoperative parameters, postoperative recovery, radiological union, functional outcomes using the Harris Hip Score and complications were evaluated. Statistical analysis was performed using SPSS version 25.0, with significance set at pResults: The mean operative time was significantly shorter in the proximal femoral nailing group (85.4 ± 12.5 min) than in the locking plate group (110.6 ± 15.3 min). Intraoperative blood loss was lower with nailing (180 ± 40 mL vs. 270 ± 60 mL). Time to partial weight bearing (4.8 ± 1.2 vs. 6.2 ± 1.6 weeks) and radiological union (17.6 ± 3.1 vs. 20.8 ± 3.7 weeks) were significantly earlier with nailing. Mean Harris Hip Score was higher following nailing (83.5 ± 6.4 vs 77.2 ± 7.8). Conclusion: Proximal femoral nailing provides superior operative efficiency, faster recovery and improved functional outcomes compared with proximal femoral locking plate fixation.},
year = {2026}
}
TY - JOUR
T1 - Comparison Between Proximal Femoral Nailing and Proximal Femoral Locking Plate in Closed Subtrochanteric Fracture
AU - Avishek Bhadra
AU - Gulam Mustofa
AU - Zahid Hasan Hemal
AU - Sabbir Ahmed
AU - Ashikur Rahman
Y1 - 2026/02/14
PY - 2026
N1 - https://doi.org/10.11648/j.ajot.20260101.14
DO - 10.11648/j.ajot.20260101.14
T2 - American Journal of Orthopaedics and Traumatology
JF - American Journal of Orthopaedics and Traumatology
JO - American Journal of Orthopaedics and Traumatology
SP - 20
EP - 26
PB - Science Publishing Group
UR - https://doi.org/10.11648/j.ajot.20260101.14
AB - Background: Subtrochanteric femoral fractures are unstable injuries characterized by high mechanical stress, cortical bone predominance and an increased risk of fixation failure. Optimal implant selection remains controversial, particularly for unstable fracture patterns. This study aimed to compare the outcomes of proximal femoral nailing and locking plate fixation in the management of closed subtrochanteric femoral fractures. Methods: This comparative study was conducted at the Department of Orthopaedics, President Abdul Hamid Medical College Hospital, Kishoreganj, Bangladesh, from January to December 2025. Fifty adult patients with closed subtrochanteric femoral fractures were divided into two groups: proximal femoral nailing (PFN, n=25) and proximal femoral locking plate fixation (PFLP, n=25). Intraoperative parameters, postoperative recovery, radiological union, functional outcomes using the Harris Hip Score and complications were evaluated. Statistical analysis was performed using SPSS version 25.0, with significance set at pResults: The mean operative time was significantly shorter in the proximal femoral nailing group (85.4 ± 12.5 min) than in the locking plate group (110.6 ± 15.3 min). Intraoperative blood loss was lower with nailing (180 ± 40 mL vs. 270 ± 60 mL). Time to partial weight bearing (4.8 ± 1.2 vs. 6.2 ± 1.6 weeks) and radiological union (17.6 ± 3.1 vs. 20.8 ± 3.7 weeks) were significantly earlier with nailing. Mean Harris Hip Score was higher following nailing (83.5 ± 6.4 vs 77.2 ± 7.8). Conclusion: Proximal femoral nailing provides superior operative efficiency, faster recovery and improved functional outcomes compared with proximal femoral locking plate fixation.
VL - 1
IS - 1
ER -
Bhadra, A., Mustofa, G., Hemal, Z. H., Ahmed, S., Rahman, A. (2026). Comparison Between Proximal Femoral Nailing and Proximal Femoral Locking Plate in Closed Subtrochanteric Fracture. American Journal of Orthopaedics and Traumatology, 1(1), 20-26. https://doi.org/10.11648/j.ajot.20260101.14
Bhadra A, Mustofa G, Hemal ZH, Ahmed S, Rahman A. Comparison Between Proximal Femoral Nailing and Proximal Femoral Locking Plate in Closed Subtrochanteric Fracture. Am J Orthop Traumatol. 2026;1(1):20-26. doi: 10.11648/j.ajot.20260101.14
@article{10.11648/j.ajot.20260101.14,
author = {Avishek Bhadra and Gulam Mustofa and Zahid Hasan Hemal and Sabbir Ahmed and Ashikur Rahman},
title = {Comparison Between Proximal Femoral Nailing and Proximal Femoral Locking Plate in Closed Subtrochanteric Fracture},
journal = {American Journal of Orthopaedics and Traumatology},
volume = {1},
number = {1},
pages = {20-26},
doi = {10.11648/j.ajot.20260101.14},
url = {https://doi.org/10.11648/j.ajot.20260101.14},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ajot.20260101.14},
abstract = {Background: Subtrochanteric femoral fractures are unstable injuries characterized by high mechanical stress, cortical bone predominance and an increased risk of fixation failure. Optimal implant selection remains controversial, particularly for unstable fracture patterns. This study aimed to compare the outcomes of proximal femoral nailing and locking plate fixation in the management of closed subtrochanteric femoral fractures. Methods: This comparative study was conducted at the Department of Orthopaedics, President Abdul Hamid Medical College Hospital, Kishoreganj, Bangladesh, from January to December 2025. Fifty adult patients with closed subtrochanteric femoral fractures were divided into two groups: proximal femoral nailing (PFN, n=25) and proximal femoral locking plate fixation (PFLP, n=25). Intraoperative parameters, postoperative recovery, radiological union, functional outcomes using the Harris Hip Score and complications were evaluated. Statistical analysis was performed using SPSS version 25.0, with significance set at pResults: The mean operative time was significantly shorter in the proximal femoral nailing group (85.4 ± 12.5 min) than in the locking plate group (110.6 ± 15.3 min). Intraoperative blood loss was lower with nailing (180 ± 40 mL vs. 270 ± 60 mL). Time to partial weight bearing (4.8 ± 1.2 vs. 6.2 ± 1.6 weeks) and radiological union (17.6 ± 3.1 vs. 20.8 ± 3.7 weeks) were significantly earlier with nailing. Mean Harris Hip Score was higher following nailing (83.5 ± 6.4 vs 77.2 ± 7.8). Conclusion: Proximal femoral nailing provides superior operative efficiency, faster recovery and improved functional outcomes compared with proximal femoral locking plate fixation.},
year = {2026}
}
TY - JOUR
T1 - Comparison Between Proximal Femoral Nailing and Proximal Femoral Locking Plate in Closed Subtrochanteric Fracture
AU - Avishek Bhadra
AU - Gulam Mustofa
AU - Zahid Hasan Hemal
AU - Sabbir Ahmed
AU - Ashikur Rahman
Y1 - 2026/02/14
PY - 2026
N1 - https://doi.org/10.11648/j.ajot.20260101.14
DO - 10.11648/j.ajot.20260101.14
T2 - American Journal of Orthopaedics and Traumatology
JF - American Journal of Orthopaedics and Traumatology
JO - American Journal of Orthopaedics and Traumatology
SP - 20
EP - 26
PB - Science Publishing Group
UR - https://doi.org/10.11648/j.ajot.20260101.14
AB - Background: Subtrochanteric femoral fractures are unstable injuries characterized by high mechanical stress, cortical bone predominance and an increased risk of fixation failure. Optimal implant selection remains controversial, particularly for unstable fracture patterns. This study aimed to compare the outcomes of proximal femoral nailing and locking plate fixation in the management of closed subtrochanteric femoral fractures. Methods: This comparative study was conducted at the Department of Orthopaedics, President Abdul Hamid Medical College Hospital, Kishoreganj, Bangladesh, from January to December 2025. Fifty adult patients with closed subtrochanteric femoral fractures were divided into two groups: proximal femoral nailing (PFN, n=25) and proximal femoral locking plate fixation (PFLP, n=25). Intraoperative parameters, postoperative recovery, radiological union, functional outcomes using the Harris Hip Score and complications were evaluated. Statistical analysis was performed using SPSS version 25.0, with significance set at pResults: The mean operative time was significantly shorter in the proximal femoral nailing group (85.4 ± 12.5 min) than in the locking plate group (110.6 ± 15.3 min). Intraoperative blood loss was lower with nailing (180 ± 40 mL vs. 270 ± 60 mL). Time to partial weight bearing (4.8 ± 1.2 vs. 6.2 ± 1.6 weeks) and radiological union (17.6 ± 3.1 vs. 20.8 ± 3.7 weeks) were significantly earlier with nailing. Mean Harris Hip Score was higher following nailing (83.5 ± 6.4 vs 77.2 ± 7.8). Conclusion: Proximal femoral nailing provides superior operative efficiency, faster recovery and improved functional outcomes compared with proximal femoral locking plate fixation.
VL - 1
IS - 1
ER -