Background: Accurate glucose measurement is central to effective glycaemic control in type 2 diabetes mellitus (T2DM). While central laboratory plasma glucose measurement remains the reference standard, point-of-care testing (POCT) glucometers are widely used in clinical practice because of their convenience and rapid turnaround time. Objective:This study compared the analytical performance of POCT glucose measurement with central laboratory glucose measurement among patients with T2DM. Method:A cross-sectional study was conducted among 100 confirmed T2DM patients attending the diabetes clinic of Jos University Teaching Hospital, North-Central Nigeria. Fasting venous plasma glucose was measured using the hexokinase method on a Cobas c111 analyzer, while capillary glucose was simultaneously measured using a standardized On-Call Plus glucometer. Data were analyzed using Pearson correlation and Bland–Altman agreement analysis. Result: The mean glucose values were 9.24 ± 4.98 mmol/L for POCT and 7.40 ± 4.13 mmol/L for laboratory measurement (p < 0.0001). A strong positive correlation was observed (r = 0.91, p < 0.0001). Bland–Altman analysis showed a mean bias of 1.9 mmol/L, with limits of agreement from −2.3 to +6.1 mmol/L, indicating a tendency for POCT values to be higher. Conclusion:POCT glucose measurement demonstrates good correlation with laboratory glucose but shows a positive bias. Regular quality assurance and periodic comparison with laboratory methods are essential to ensure safe clinical use.
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited.
Point-of-Care Testing, Glucose Monitoring, Type 2 Diabetes Mellitus, Method Evaluation
1. Introduction
Diabetes Mellitus (DM) is a metabolic disorder characterized by chronic hyperglycaemia and confers a huge financial burden for health systems globally.There has been tremendous increase in it’s prevalence with a demographic transition in its epidemiology in recent years such that populations previously unaffected or minimally affected by DM are now reporting increasing prevalence figures, making DM a major public health problem worldwide
[1]
Uloko A, Musa BM, Ramalan MA, Gezawa ID, Puepet FH, Uloko AT, et al. Prevalence and risk factors for diabetes mellitus in Nigeria: a systematic review and meta-analysis. Diabetes Therapy. 2018; 9(3): 1307-1316.
. Projections by the International Diabetes Federation (IDF) states that approximately 589 million adults (aged 20-79 years) are now living with DM worldwide with nearly 50% of these undiagnosed. These figures are expected to rise to about 853 million by 2050. A significant fraction of this figure is from developing countries of Africa and Asia. Factors that contribute to this soaring epidemic of DM are the aging population, increasing urbanization, sedentary lifestyle and obesity. The prevalence of DM in Nigeria is about 5.77%
[1]
Uloko A, Musa BM, Ramalan MA, Gezawa ID, Puepet FH, Uloko AT, et al. Prevalence and risk factors for diabetes mellitus in Nigeria: a systematic review and meta-analysis. Diabetes Therapy. 2018; 9(3): 1307-1316.
DM is associated with complications that have a linear relationship with the average plasma glucose and the management of diabetes relies on adequate long-term monitoring of glycaemic control. The result of the Diabetes Control and Complications Trial (DCCT) demonstrated the importance of tight glucose control for the prevention of complications of diabetes mellitus. Glycaemic control monitoring in DM has been based on glucose criteria and glycated haemoglobin criteria. The use of point-of-care glucose measurment is convenient for a number of reasons; it provides rapid results, is convenient for both the patient and healthcare provider and gets the patient more involved in their care
[2]
International Diabetes Federation (IDF) (2025) IDF Diabetes Atlas. 11th Edition, International Diabetes Federation.URL:
Central laboratory glucose measurements are considered the gold standard for glucose measurements because they employ methods that are more accurate and less susceptible to interferences. It is therefore pertinent that point of care glucose measurements are close as possible to those obtained by the central laboratory. This study therefore aims to compare the accuracy and practicability of Point-of care (POC) and Central Laboratory (CL) glucose measurements in monitoring glycaemic control in a cohort of T2DM patients accessing care at a tertiary hospital in North central Nigeria
[3]
Ogunbosi BO, Jarrett OO, Orimadegun AE, Ayoola OO, Osinusi K. Comparison of point-of-care glucometers and laboratory-based glucose oxidase test in determining blood glucose levels. Niger J Paediatr. 2022; 49(3): 266-271.
Aliyu RM, Zainab M, Sani M, Gezawa I, Uloko A. Should we assume accuracy of point-of-care glucose meters? Precision and accuracy of four glucose meters compared to laboratory method. Niger J Med. 2019; 28(2): 133-137.
[5]
Choukem SP, Sih C, Nebongo D, Keunmoe P, Kengne AP. Accuracy and precision of four main glucometers used in a sub-Saharan African country: a cross-sectional study. Pan Afr Med J. 2019; 32: 118.
This cross-sectional study was conducted among a total of 100 confirmed T2DM patients attending the diabetes clinic of Jos University Teaching Hospital. Written informed consent was obtained from all participants who met the inclusion criteria i.e confirmed T2DM patients who are on regular follow up at the diabetic clinic. 5 mL of venous blood was collected from the cubital fossa in the morning hours between 8-10 am after an overnight fast of 8-12 hours; a wide bore needle and dry clean vacutainers containing fluoride oxalate was used for each participant to prevent haemolysis. Sample was centrifuged at 3000 rmp for 3 mins and plasma obtained was used for glucose analysis on cobas c111 using the hexokinase method. Blood glucose was also assessed simultaneously using a standardised On-Call-Plus glucometer (a pilot study showed that upto 60% of patients who own a glucometer and monitor their glucose at home utilise this brand, making it the most popular), using capillary blood gotten from a finger prick.
The data collected from the study was analyzed using SSPS version 23. Descriptive statistics of mean, standard deviation, percentages were determined. Association between results obtained from the various methods were evaluated using Pearson's correlation coefficient while Bland-Altman analysis was used to determine agreement between the methods. A value of p<0.05 was considered statistically significant for this study.
3. Results
A total of one hundred (100) pre-diagnosed T2DM patients participated in the study (Table 1), which included 37 males (37%) and 63 females (63%). Their age range varied from 22-68 years, with a mean age of 57.29±10.35 years. The age range of the volunteered participants in this study accentuates the fact that type 2 diabetes mellitus is common among adult Nigerians. According to reports by the International Diabetes Federation (IDF), diabetes affects both children and adults with the adult age range being between 20-79 years. Reports by IDF also stated that the prevalence by age and sex appeared more between ages 40-79 years with peak age of 50-59 years and that males have higher prevalence of diabetes compared to females within the age group of 40-79 years whereas, between ages 20-39 years, the prevalence of diabetes among female appears higher than that of the males
[3]
Ogunbosi BO, Jarrett OO, Orimadegun AE, Ayoola OO, Osinusi K. Comparison of point-of-care glucometers and laboratory-based glucose oxidase test in determining blood glucose levels. Niger J Paediatr. 2022; 49(3): 266-271.
Aliyu RM, Zainab M, Sani M, Gezawa I, Uloko A. Should we assume accuracy of point-of-care glucose meters? Precision and accuracy of four glucose meters compared to laboratory method. Niger J Med. 2019; 28(2): 133-137.
[5]
Choukem SP, Sih C, Nebongo D, Keunmoe P, Kengne AP. Accuracy and precision of four main glucometers used in a sub-Saharan African country: a cross-sectional study. Pan Afr Med J. 2019; 32: 118.
Pleus S, Schmid C, Link M, Zschornack E, Klötzer HM, Haug C, et al. Accuracy evaluation of 18 blood glucose monitoring systems according to ISO 15197:2015. Diabetes Technol Ther. 2020; 22(6): 412-418.
Table 1. Socio-demographic Characteristics of the Diabetic Patients (N=100).Socio-demographic Characteristics of the Diabetic Patients (N=100).Socio-demographic Characteristics of the Diabetic Patients (N=100).
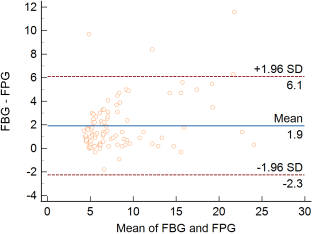
Figure 1. Bland-Altman plot for POCT and Central Laboratory glucose values.Bland-Altman plot for POCT and Central Laboratory glucose values.
Table 2. Comparative analysis of glucose determination using POCT and Central Laboratory Assay.Comparative analysis of glucose determination using POCT and Central Laboratory Assay.Comparative analysis of glucose determination using POCT and Central Laboratory Assay.
Method
Number of participants’
mean±S.D (mmol/L)
p Value
On Call Plus
100
9.24 ±4.98
<0.0001
Hexokinase
100
7.40±4.13
<0.0001
Significant level: p<0.05
The correlation coefficient (r) between POCT glucose values and central laboratory glucose values was 0.91;P<0.0001, indicating a strong positive correlation. A Bland-Altman analysis showed a mean bias of 1.9 mmol/L, indicating a tendency for point-of-care glucose values to be higher than laboratory glucose values. The limits of agreement were calculated as -2.3 to +6.1 mmol/L, within which 95% of the differences between the two methods were contained. The findings highlight both the reliability and limitations of POC glucose monitoring in clinical practice.
4. Discussion
The first commercially available glucose POCT was produced in 1970, which measured blood glucose levels using the glucose oxidase (GO) method. Over time, glucose POCT has evolved, securing a foothold in everyday clinical practice and into patients’ homes as a critical tool in diabetes management. The accuracy of results obtained from a glucose POCT depends on a lot of factors, ranging from manufacturing technique to operator training and patient factors. Errors arising from any of these areas can compound, leading to worsening inaccuracy. While no true gold standard exists for glucose testing, POCT results are compared to laboratory plasma glucose levels when results are suspicious or inconsistent
[7]
Luppa PB, Schlebusch H, Klostermann R, Huber S, Schleichert J, Neumann F, et al. Quality assessment of glucose measurement with regard to epidemiology and clinical management of diabetes mellitus in Germany. Front Mol Biosci. 2024; 11: 1371426.
Tonyushkina K, Nichols JH. Glucose Meters:AReview of Technical Challenges to Obtaining Accurate Results. J Diabetes Sci Technol. 2009: 3(5): 1462-70.
[7, 10]
.
POCT glucometers utilize GO or glucose-1-dehydrogenase (GDH) reactions and conveniently use whole blood measurements at the patient’s bedside, then convert the results to plasma glucose concentrations, the standardized form used in clinical practice. While the International Federation of Clinical Chemistry and Laboratory Medicine (IFCC) recommends a conversion factor of 1.11, the equation assumes standardized parameters for hematocrit, plasma, and red blood cell water concentrations that may not be accurate in individual patients
[6]
Pleus S, Schmid C, Link M, Zschornack E, Klötzer HM, Haug C, et al. Accuracy evaluation of 18 blood glucose monitoring systems according to ISO 15197:2015. Diabetes Technol Ther. 2020; 22(6): 412-418.
Luppa PB, Schlebusch H, Klostermann R, Huber S, Schleichert J, Neumann F, et al. Quality assessment of glucose measurement with regard to epidemiology and clinical management of diabetes mellitus in Germany. Front Mol Biosci. 2024; 11: 1371426.
Ukpe MP, Okafor IM, Bello SO, Adebayo AO, Lawal TO, Musa BM, et al. Accuracy of point-of-care devices for blood glucose estimation: a systematic review and meta-analysis. Afr J Lab Med. 2024; 13(1): a2451.
Both the International Organization for Standardization (ISO) and Clinical and Laboratory Standards Institute (CLSI) have published guidelines regarding accuracy in glucose POCT, with CLSI being the more stringent for hospital POCT use. According to ISO, 95% of individual glucose results should fall within ±15 mg/dL (± 0.83 mmol/L) of the reference method for glucose concentrations <100 mg/dL (<5.55 mmol/L), and within ±15% of the reference for concentrations ≥100 mg/dL (≥5.55 mmol/L). By contrast CLSI requires that ≥95% of results should be within ±12 mg/dL (±0.67 mmol/L) for glucose values <100 mg/dL, and within ±12.5% when concentartions are ≥100 mg/dL. In addition, when the cutoff level is <75 mg/dL (4.17 mmol/L), 98% of values should be within ±15 mg/dL and ±20% for those ≥75 mg/dL (4.17 mmol/L [6.9]).
In this study, the glucose values obtained from the standardized On-Call Plus glucometer (glucose oxidase method) and that obtained from the central laboratory (Hexokinase method) showed good agreement as evidenced by the strong positive correlation between the set of values obtained, but with a tendency for the POC glucose values to give higher values as the mean bias from the Bland-Altman analysis is 1.9 mmol/L and limits of agreement of -2.3 and +6.1 mmol/L respectively. This finding therefoere contributes to the accumulating evidence that point-of-care (POC) blood glucose monitoring systems (BGMS) demonstrate variable analytical agreement with central laboratory glucose measurement procedures, with performance strongly influenced by device characteristics, patient population, and clinical context. Similar Nigerian and international studies carried out with Bland–Altman analyses consistently reveal wide limits of agreement despite modest mean bias in some devices
[3]
Ogunbosi BO, Jarrett OO, Orimadegun AE, Ayoola OO, Osinusi K. Comparison of point-of-care glucometers and laboratory-based glucose oxidase test in determining blood glucose levels. Niger J Paediatr. 2022; 49(3): 266-271.
Aliyu RM, Zainab M, Sani M, Gezawa I, Uloko A. Should we assume accuracy of point-of-care glucose meters? Precision and accuracy of four glucose meters compared to laboratory method. Niger J Med. 2019; 28(2): 133-137.
[8]
Ukpe MP, Okafor IM, Bello SO, Adebayo AO, Lawal TO, Musa BM, et al. Accuracy of point-of-care devices for blood glucose estimation: a systematic review and meta-analysis. Afr J Lab Med. 2024; 13(1): a2451.
Dahman LSB, Daakeek AM, Alghazali HS, Kaity AM, Obbed MS, Al-Shameri EE. Evaluation of three glucometer devices in comparison with Cobas Integra 400 Plus autoanalyzer in measuring blood glucose levels. Int J Diabetes Mellit. 2021; 11(4): 132-142.
[3, 4, 8, 9]
. According to ISO-15197:2013/2015, analytical acceptability is not determined by correlation or mean bias alone but by the proportion of individual results falling within predefined accuracy limits, highlighting the importance of method-comparison statistics in evaluating BGMS performance
[11]
Dickson R, Buchmann EJ, Norris SA. Accuracy of point-of-care testing glucometers for the diagnosis of gestational diabetes mellitus. BMC Pregnancy Childbirth. 2019; 19: 203.
Khambule L, Norris SA, Crowther NJ, Madhi SA, Naidoo P, Venter C, et al. Diagnostic accuracy of point-of-care glucometers for gestational diabetes mellitus in South Africa. PLoS One. 2024; 19(1): e0298476.
Studies from several other settings have reported comparable results, though with variability between devices and patient groups. A study from Cameroon assessing four commonly used glucometers against laboratory method showed most devices achieved accceptable clinical accuracy, with at least 95% (96% from our study) values falling within consensus error grid zones and also demonstrated a positive bias, with POC glucometers tending to read higher than laboratory values
[5]
Choukem SP, Sih C, Nebongo D, Keunmoe P, Kengne AP. Accuracy and precision of four main glucometers used in a sub-Saharan African country: a cross-sectional study. Pan Afr Med J. 2019; 32: 118.
Dahman LSB, Daakeek AM, Alghazali HS, Kaity AM, Obbed MS, Al-Shameri EE. Evaluation of three glucometer devices in comparison with Cobas Integra 400 Plus autoanalyzer in measuring blood glucose levels. Int J Diabetes Mellit. 2021; 11(4): 132-142.
[11]
Dickson R, Buchmann EJ, Norris SA. Accuracy of point-of-care testing glucometers for the diagnosis of gestational diabetes mellitus. BMC Pregnancy Childbirth. 2019; 19: 203.
Other regional comparative studies that used Bland–Altman plots to asses agreement between POC glucometers and laboratory glucose have similarly reported narrow limits of agreement and high proportions of readings within ±20% of reference values, supporting the clinical reliability of POC testing while emphasizing the need for device-specific calibration and quality control. Internationally, work from South Asia and the Middle East in type 2 diabetes cohorts has shown strong correlations between capillary glucometer readings and venous laboratory glucose, with Bland–Altman analysis revealing small mean bias and limits of agreement that meet ISO 15197 criteria, although some devices perform better in the mid‑glycaemic range than at very low or very high glucose concentrations
[6]
Pleus S, Schmid C, Link M, Zschornack E, Klötzer HM, Haug C, et al. Accuracy evaluation of 18 blood glucose monitoring systems according to ISO 15197:2015. Diabetes Technol Ther. 2020; 22(6): 412-418.
Ukpe MP, Okafor IM, Bello SO, Adebayo AO, Lawal TO, Musa BM, et al. Accuracy of point-of-care devices for blood glucose estimation: a systematic review and meta-analysis. Afr J Lab Med. 2024; 13(1): a2451.
Khambule L, Norris SA, Crowther NJ, Madhi SA, Naidoo P, Venter C, et al. Diagnostic accuracy of point-of-care glucometers for gestational diabetes mellitus in South Africa. PLoS One. 2024; 19(1): e0298476.
By demonstrating good correlation and acceptable Bland–Altman agreement between POC and central laboratory glucose in local patients with type 2 diabetes, our study provides context-specific evidence to support structured use of POC glucose meters for both outpatient and inpatient management, especially where rapid decisions on dose adjustment or hypoglycaemia management are needed. At the same time, the presence of measurable bias and error margins, even if within acceptable limits, reinforces the need for regular internal quality control, periodic comparison with laboratory reference methods, staff training on proper sampling technique, and adherence to device maintenance and calibration protocols to ensure sustained accuracy.
In a resource-limited setting like most parts of Ngeria where reliance on POC testing is often driven by accessibility and cost, these results have important implications. Strengthening laboratory–POC integration, implementing routine glucometer performance verification against reference methods, and educating clinicians on the limitations of POC glucose testing are essential steps toward improving patient safety and diagnostic accuracy.
Abbreviation
BGMS
Blood Glucose Monitoring Systems
CL
Central Laboratory
CLSI
Clinical and Laboratory Standards Institute
DCCT
Diabetes Control and Complications Trial
DM
Diabetes Mellitus
GDH
Glucose-1-Dehydrogenase
GO
Glucose Oxidase
HbA1c
Glycated Haemoglobin
IDF
International Diabetes Federation
IFCC
International Federation of Clinical Chemistry and Laboratory Medicine
ISO
International Organization for Standardization
POCT
Point-of-Care Testing
SD
Standard Deviation
SPSS
Statistical Package for the Social Sciences
T2DM
Type 2 Diabetes Mellitus
Conflicts of Interest
The authors declare no conflicts of interest.
References
[1]
Uloko A, Musa BM, Ramalan MA, Gezawa ID, Puepet FH, Uloko AT, et al. Prevalence and risk factors for diabetes mellitus in Nigeria: a systematic review and meta-analysis. Diabetes Therapy. 2018; 9(3): 1307-1316.
Aliyu RM, Zainab M, Sani M, Gezawa I, Uloko A. Should we assume accuracy of point-of-care glucose meters? Precision and accuracy of four glucose meters compared to laboratory method. Niger J Med. 2019; 28(2): 133-137.
[5]
Choukem SP, Sih C, Nebongo D, Keunmoe P, Kengne AP. Accuracy and precision of four main glucometers used in a sub-Saharan African country: a cross-sectional study. Pan Afr Med J. 2019; 32: 118.
Pleus S, Schmid C, Link M, Zschornack E, Klötzer HM, Haug C, et al. Accuracy evaluation of 18 blood glucose monitoring systems according to ISO 15197:2015. Diabetes Technol Ther. 2020; 22(6): 412-418.
Luppa PB, Schlebusch H, Klostermann R, Huber S, Schleichert J, Neumann F, et al. Quality assessment of glucose measurement with regard to epidemiology and clinical management of diabetes mellitus in Germany. Front Mol Biosci. 2024; 11: 1371426.
Ukpe MP, Okafor IM, Bello SO, Adebayo AO, Lawal TO, Musa BM, et al. Accuracy of point-of-care devices for blood glucose estimation: a systematic review and meta-analysis. Afr J Lab Med. 2024; 13(1): a2451.
Dahman LSB, Daakeek AM, Alghazali HS, Kaity AM, Obbed MS, Al-Shameri EE. Evaluation of three glucometer devices in comparison with Cobas Integra 400 Plus autoanalyzer in measuring blood glucose levels. Int J Diabetes Mellit. 2021; 11(4): 132-142.
[10]
Tonyushkina K, Nichols JH. Glucose Meters:AReview of Technical Challenges to Obtaining Accurate Results. J Diabetes Sci Technol. 2009: 3(5): 1462-70.
[11]
Dickson R, Buchmann EJ, Norris SA. Accuracy of point-of-care testing glucometers for the diagnosis of gestational diabetes mellitus. BMC Pregnancy Childbirth. 2019; 19: 203.
Khambule L, Norris SA, Crowther NJ, Madhi SA, Naidoo P, Venter C, et al. Diagnostic accuracy of point-of-care glucometers for gestational diabetes mellitus in South Africa. PLoS One. 2024; 19(1): e0298476.
Luka, S. M., Ishaku, A. A., Stephen, L. M., Ogoegbunem, I. C. (2026). Performance Evaluation of Point-of-Care Glucose Meter in Adults with Type 2 Diabetes Mellitus: Evidence from North-central Nigeria. American Journal of Laboratory Medicine, 11(1), 24-28. https://doi.org/10.11648/j.ajlm.20261101.14
Luka, S. M.; Ishaku, A. A.; Stephen, L. M.; Ogoegbunem, I. C. Performance Evaluation of Point-of-Care Glucose Meter in Adults with Type 2 Diabetes Mellitus: Evidence from North-central Nigeria. Am. J. Lab. Med.2026, 11(1), 24-28. doi: 10.11648/j.ajlm.20261101.14
Luka SM, Ishaku AA, Stephen LM, Ogoegbunem IC. Performance Evaluation of Point-of-Care Glucose Meter in Adults with Type 2 Diabetes Mellitus: Evidence from North-central Nigeria. Am J Lab Med. 2026;11(1):24-28. doi: 10.11648/j.ajlm.20261101.14
@article{10.11648/j.ajlm.20261101.14,
author = {Solomon Mercy Luka and Ayuba Affi Ishaku and Lukden Mawun Stephen and Isichei Christain Ogoegbunem},
title = {Performance Evaluation of Point-of-Care Glucose Meter in Adults with Type 2 Diabetes Mellitus: Evidence from North-central Nigeria},
journal = {American Journal of Laboratory Medicine},
volume = {11},
number = {1},
pages = {24-28},
doi = {10.11648/j.ajlm.20261101.14},
url = {https://doi.org/10.11648/j.ajlm.20261101.14},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ajlm.20261101.14},
abstract = {Background: Accurate glucose measurement is central to effective glycaemic control in type 2 diabetes mellitus (T2DM). While central laboratory plasma glucose measurement remains the reference standard, point-of-care testing (POCT) glucometers are widely used in clinical practice because of their convenience and rapid turnaround time. Objective:This study compared the analytical performance of POCT glucose measurement with central laboratory glucose measurement among patients with T2DM. Method: A cross-sectional study was conducted among 100 confirmed T2DM patients attending the diabetes clinic of Jos University Teaching Hospital, North-Central Nigeria. Fasting venous plasma glucose was measured using the hexokinase method on a Cobas c111 analyzer, while capillary glucose was simultaneously measured using a standardized On-Call Plus glucometer. Data were analyzed using Pearson correlation and Bland–Altman agreement analysis. Result: The mean glucose values were 9.24 ± 4.98 mmol/L for POCT and 7.40 ± 4.13 mmol/L for laboratory measurement (p Conclusion: POCT glucose measurement demonstrates good correlation with laboratory glucose but shows a positive bias. Regular quality assurance and periodic comparison with laboratory methods are essential to ensure safe clinical use.},
year = {2026}
}
TY - JOUR
T1 - Performance Evaluation of Point-of-Care Glucose Meter in Adults with Type 2 Diabetes Mellitus: Evidence from North-central Nigeria
AU - Solomon Mercy Luka
AU - Ayuba Affi Ishaku
AU - Lukden Mawun Stephen
AU - Isichei Christain Ogoegbunem
Y1 - 2026/01/27
PY - 2026
N1 - https://doi.org/10.11648/j.ajlm.20261101.14
DO - 10.11648/j.ajlm.20261101.14
T2 - American Journal of Laboratory Medicine
JF - American Journal of Laboratory Medicine
JO - American Journal of Laboratory Medicine
SP - 24
EP - 28
PB - Science Publishing Group
SN - 2575-386X
UR - https://doi.org/10.11648/j.ajlm.20261101.14
AB - Background: Accurate glucose measurement is central to effective glycaemic control in type 2 diabetes mellitus (T2DM). While central laboratory plasma glucose measurement remains the reference standard, point-of-care testing (POCT) glucometers are widely used in clinical practice because of their convenience and rapid turnaround time. Objective:This study compared the analytical performance of POCT glucose measurement with central laboratory glucose measurement among patients with T2DM. Method: A cross-sectional study was conducted among 100 confirmed T2DM patients attending the diabetes clinic of Jos University Teaching Hospital, North-Central Nigeria. Fasting venous plasma glucose was measured using the hexokinase method on a Cobas c111 analyzer, while capillary glucose was simultaneously measured using a standardized On-Call Plus glucometer. Data were analyzed using Pearson correlation and Bland–Altman agreement analysis. Result: The mean glucose values were 9.24 ± 4.98 mmol/L for POCT and 7.40 ± 4.13 mmol/L for laboratory measurement (p Conclusion: POCT glucose measurement demonstrates good correlation with laboratory glucose but shows a positive bias. Regular quality assurance and periodic comparison with laboratory methods are essential to ensure safe clinical use.
VL - 11
IS - 1
ER -
Luka, S. M., Ishaku, A. A., Stephen, L. M., Ogoegbunem, I. C. (2026). Performance Evaluation of Point-of-Care Glucose Meter in Adults with Type 2 Diabetes Mellitus: Evidence from North-central Nigeria. American Journal of Laboratory Medicine, 11(1), 24-28. https://doi.org/10.11648/j.ajlm.20261101.14
Luka, S. M.; Ishaku, A. A.; Stephen, L. M.; Ogoegbunem, I. C. Performance Evaluation of Point-of-Care Glucose Meter in Adults with Type 2 Diabetes Mellitus: Evidence from North-central Nigeria. Am. J. Lab. Med.2026, 11(1), 24-28. doi: 10.11648/j.ajlm.20261101.14
Luka SM, Ishaku AA, Stephen LM, Ogoegbunem IC. Performance Evaluation of Point-of-Care Glucose Meter in Adults with Type 2 Diabetes Mellitus: Evidence from North-central Nigeria. Am J Lab Med. 2026;11(1):24-28. doi: 10.11648/j.ajlm.20261101.14
@article{10.11648/j.ajlm.20261101.14,
author = {Solomon Mercy Luka and Ayuba Affi Ishaku and Lukden Mawun Stephen and Isichei Christain Ogoegbunem},
title = {Performance Evaluation of Point-of-Care Glucose Meter in Adults with Type 2 Diabetes Mellitus: Evidence from North-central Nigeria},
journal = {American Journal of Laboratory Medicine},
volume = {11},
number = {1},
pages = {24-28},
doi = {10.11648/j.ajlm.20261101.14},
url = {https://doi.org/10.11648/j.ajlm.20261101.14},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ajlm.20261101.14},
abstract = {Background: Accurate glucose measurement is central to effective glycaemic control in type 2 diabetes mellitus (T2DM). While central laboratory plasma glucose measurement remains the reference standard, point-of-care testing (POCT) glucometers are widely used in clinical practice because of their convenience and rapid turnaround time. Objective:This study compared the analytical performance of POCT glucose measurement with central laboratory glucose measurement among patients with T2DM. Method: A cross-sectional study was conducted among 100 confirmed T2DM patients attending the diabetes clinic of Jos University Teaching Hospital, North-Central Nigeria. Fasting venous plasma glucose was measured using the hexokinase method on a Cobas c111 analyzer, while capillary glucose was simultaneously measured using a standardized On-Call Plus glucometer. Data were analyzed using Pearson correlation and Bland–Altman agreement analysis. Result: The mean glucose values were 9.24 ± 4.98 mmol/L for POCT and 7.40 ± 4.13 mmol/L for laboratory measurement (p Conclusion: POCT glucose measurement demonstrates good correlation with laboratory glucose but shows a positive bias. Regular quality assurance and periodic comparison with laboratory methods are essential to ensure safe clinical use.},
year = {2026}
}
TY - JOUR
T1 - Performance Evaluation of Point-of-Care Glucose Meter in Adults with Type 2 Diabetes Mellitus: Evidence from North-central Nigeria
AU - Solomon Mercy Luka
AU - Ayuba Affi Ishaku
AU - Lukden Mawun Stephen
AU - Isichei Christain Ogoegbunem
Y1 - 2026/01/27
PY - 2026
N1 - https://doi.org/10.11648/j.ajlm.20261101.14
DO - 10.11648/j.ajlm.20261101.14
T2 - American Journal of Laboratory Medicine
JF - American Journal of Laboratory Medicine
JO - American Journal of Laboratory Medicine
SP - 24
EP - 28
PB - Science Publishing Group
SN - 2575-386X
UR - https://doi.org/10.11648/j.ajlm.20261101.14
AB - Background: Accurate glucose measurement is central to effective glycaemic control in type 2 diabetes mellitus (T2DM). While central laboratory plasma glucose measurement remains the reference standard, point-of-care testing (POCT) glucometers are widely used in clinical practice because of their convenience and rapid turnaround time. Objective:This study compared the analytical performance of POCT glucose measurement with central laboratory glucose measurement among patients with T2DM. Method: A cross-sectional study was conducted among 100 confirmed T2DM patients attending the diabetes clinic of Jos University Teaching Hospital, North-Central Nigeria. Fasting venous plasma glucose was measured using the hexokinase method on a Cobas c111 analyzer, while capillary glucose was simultaneously measured using a standardized On-Call Plus glucometer. Data were analyzed using Pearson correlation and Bland–Altman agreement analysis. Result: The mean glucose values were 9.24 ± 4.98 mmol/L for POCT and 7.40 ± 4.13 mmol/L for laboratory measurement (p Conclusion: POCT glucose measurement demonstrates good correlation with laboratory glucose but shows a positive bias. Regular quality assurance and periodic comparison with laboratory methods are essential to ensure safe clinical use.
VL - 11
IS - 1
ER -