Abstract
This study aimed to examine the integration of Post-Traumatic Slave Syndrome (PTSS) into Social Determinants of Health (SDOH) trainings as a means to enhance the understanding and addressing of health disparities, particularly among Black populations. Given the growing emphasis on SDOH in health education, the study sought to explore how historical trauma, specifically PTSS, contributes to ongoing health inequities and to evaluate whether its inclusion in training could lead to more culturally informed approaches in health and human services (HHS). Through ethnographic interviews with six Black female professionals in Massachusetts and Rhode Island, who had participated in SDOH trainings organized by a medical-legal partnership (MLP), the research aimed to uncover the connections between historical trauma and health disparities in the context of contemporary healthcare. By highlighting the lived experiences of professionals and their perspectives on PTSS, the study also sought to propose methods for incorporating these historical dimensions into current SDOH frameworks to foster deeper, more systemic change. The findings suggest that integrating PTSS within SDOH education is essential for developing comprehensive strategies to promote health equity and advance social justice in medical-legal collaborations.
|
Published in
|
American Journal of Health Research (Volume 13, Issue 1)
|
|
DOI
|
10.11648/j.ajhr.20251301.14
|
|
Page(s)
|
47-56 |
|
Creative Commons
|

This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited.
|
|
Copyright
|
Copyright © The Author(s), 2025. Published by Science Publishing Group
|
Keywords
Race, History, Social Determinants of Health, Post Traumatic Slave Syndrome, Health Education, Right to Health
1. Introduction
In January 2023, Florida officials blocked the introduction of a new Advanced Placement (AP) African American studies course, dismissing its educational value and compliance with state law
. By summer, Florida’s approval of controversial Black history standards, suggesting enslaved people benefited personally from their oppression, underscored a broader societal problem: the erasure and distortion of Black history. This manipulation is not just an attack on historical truth; it sustains the structural inequities that manifest in present-day health disparities.
The SDOH discourse frequently isolates contemporary health outcomes from their historical roots, creating a fragmented understanding of systemic inequities. Without historical context, medical-legal institutions have framed health disparities as innate or incidental rather than as consequences of deliberate policy decisions and intergenerational trauma. This narrative absolves systems of accountability, reducing the role of health professionals to managing suffering rather than addressing root causes.
Health inequities in Black communities are neither incidental nor ahistorical; they are rooted in centuries of systemic oppression, enslavement, and colonial exploitation. However, current SDOH frameworks frequently neglect the historical foundations of these disparities, reducing them to contemporary socioeconomic or behavioral factors. This omission perpetuates a narrative that health inequities arise in isolation, obscuring the role of historical and structural determinants in shaping the lived experiences of marginalized populations.
Figure 1. Florida Approves New Black History Standards. (Courtesy of Garssandra Presumey-Leblanc).
PTSS, as conceptualized by Dr. Joy DeGruy, offers an essential framework for confronting this historical erasure. By linking the enduring psychological and social effects of slavery and colonialism to modern health inequities, PTSS compels us to confront how historical trauma shapes health outcomes in Black communities. Yet, PTSS remains absent from most SDOH trainings, leaving HHS professionals ill-equipped to address the legacy of these inequities.
Emerging literature highlights the critical need for historical contextualization in health education and training. Scholars such as DeGruy
| [2] | DeGruy, J. (2005). Post Traumatic Slave Syndrome: America’s Legacy of Enduring Injury and Healing (Newly Rev.). Joy DeGruy Publications Inc. |
[2]
and Hanks et al.
have argued that failing to address the intergenerational impacts of slavery and structural racism in SDOH frameworks limits our ability to achieve health equity. Historical erasure not only hinders understanding but also perpetuates harm by framing disparities as inevitable or inherent. Yet, while calls for integrating historical analysis into health policy and education are growing, actionable frameworks remain underdeveloped.
To counter this historical erasure, PTSS, as conceptualized by DeGruy, provides a critical framework for understanding how intergenerational trauma influenced health outcomes. PTSS highlights the enduring psychological and social effects of slavery and colonialism, offering a lens to analyze the systemic inequities entrenched within HHS systems. However, PTSS remains conspicuously absent from most SDOH frameworks, leaving HHS professionals ill-equipped to address the legacies of structural racism.
This study investigates whether integrating PTSS into SDOH trainings can improve the understanding of health inequities among HHS professionals. Specifically, it asks:
1) How does the inclusion of historical trauma in SDOH trainings affect the capacity of HHS professionals to recognize and address systemic health inequities?
2) To what extent do Black female HHS professionals perceive PTSS and historical contextualization as critical tools in addressing the unique challenges faced by marginalized populations?
The inclusion of a MLP, operating in Massachusetts and Rhode Island, a unique context to the study. Via a service-learning internship, looking to involve observational and community-based participatory research, the MLP aided in the development of the research scope, historical framework, interview guide, and analysis interpretation. The MLP’s interdisciplinary approach integrates legal advocacy into healthcare settings, addressing systemic barriers that disproportionately affect marginalized populations. This makes MLPs an ideal setting for examining how historical frameworks like PTSS can inform SDOH practices in ways that challenge existing structural inequities.
By grounding the analysis in their personal accounts of Black female HHS professionals, this study demonstrates how incorporating PTSS into SDOH trainings can ground health equity in historical accountability and foster systemic change.
This historical education gap has real-world consequences. Marginalized populations are left to navigate systems designed to help them survive rather than thrive, perpetuating a cycle of disadvantage. The urgency to integrate PTSS into SDOH education is clear: without it, we cannot fully understand or dismantle the structures that maintain health inequities. The findings contribute to a growing body of literature that underscores the necessity of a historically informed SDOH framework to dismantle the structural barriers that perpetuate health inequities. This paper builds on the personal accounts of Black female HHS professionals to demonstrate how incorporating PTSS into SDOH trainings can serve as a transformative tool, grounding health equity efforts in historical accountability and fostering systemic change.
2. Methods
The study utilized qualitative ethnographic methods to explore the role of historical trauma and PTSS in understanding and addressing health inequities within SDOH trainings. The research population consisted of six Black female HHS workforce members who had previously participated in SDOH trainings facilitated by a MLP in Massachusetts and Rhode Island.
Table 1. Participants — Deidentified Black Female HHS Workforce Members.
Pseudonym | State | HHS Position |
Alexa Canady | Rhode Island | Director, Community Health Institute |
Rebecca Davis Lee Crumpler | Rhode Island | Director, Community Health Integration |
Joycelyn Elders | Massachusetts | Senior Project Manager |
Paula A. Johnson | Rhode Island | Community Health Outreach Worker |
Sophia B. Jones | Massachusetts | Patient Resource Coordinator |
Claudia L. Thomas | Massachusetts | Patient Navigator |
The decision to focus exclusively on Black females was intentional and grounded in the understanding that racism and discrimination are profoundly gendered experiences. Research has consistently shown that Black women face a unique intersection of racial and gender-based oppression, often referred to as misogynoir
| [4] | Bailey, M. (2010). The Intersectional Invisibility of Black Women: Misogynoir and the Multiple Marginalization of African American women. Journal of Black Studies, 41(3), 327-353. https://doi.org/10/1177/0021934709357882 |
[4]
. This intersectionality results in compounded vulnerabilities and distinct health outcomes compared to their male counterparts or women from other racial or ethnic groups. For example, Black women are disproportionately affected by maternal mortality, chronic stress, and workplace discrimination, all of which are shaped by systemic inequities and historical trauma
| [5] | Crenshaw, K. (1991). Mapping the Margins: intersectionality, Identity Politics, and Violence Against Women of Color. Stanford Law Review (43(6), 1241-1299. https://doi.org/10.2307.1229039 |
| [6] | Rosenthal, L. & Lobel, M. (20110, Explaining Disparities in Adverse Birth Outcomes: The Contributions of Maternal Stress and Coping. In S. K. M. K. S. McNaughton, L. L. G. Engle, & P. W. G. Shaw (Eds.), Psychology of Stress and Coping in Health (pp. 125-147). Cambridge University Press. https://doi.org/10/1017/CBO9780511976763.010 |
[5, 6]
.
By centering the voices of Black women, this study sought to highlight their lived experiences and insights as both recipients of healthcare disparities and advocates for marginalized populations within the HHS workforce. Each participant was assigned a pseudonym to honor pioneering Black women in medicine and to protect their confidentiality.
Participants were recruited purposively through professional networks and outreach facilitated by the MLP affiliates. Inclusion criteria required participants to identify as Black, female, and employed in the HHS sector, with prior experience in SDOH training programs. These criteria were designed to ensure participants could speak directly to both systemic inequities and the practical implications of SDOH frameworks in their work. Exclusion criteria included individuals without prior SDOH training or those not actively engaged in HHS roles, as their experiences would not align with the study’s focus on systemic and professional contexts.
Semi-structured interviews were conducted in participant-chosen locations to foster a sense of safety and comfort. Interviews were held in locations selected by the participants to foster a sense of comfort and openness. Sessions were audio-recorded with consent and lasted approximately 90-120 minutes. The interview protocol encouraged participants to reflect on their experiences with SDOH training, their understanding of PTSS, and the ways historical trauma influenced their professional and personal perspectives. To deepen the analysis, participants completed a free-association exercise linking objects or images to their understanding of SDOH. This exercise was designed to uncover implicit associations and provide richer context to their narratives.
The interview guide consisted of open-ended questions designed to elicit detailed narratives and insights. Sample questions included:
1) “How has your understanding of historical trauma influenced your perspective on health disparities?”
2) “In what ways do you think SDOH trainings could better address systemic inequities?”
3) “Can you describe a moment when historical context was or could have been critical in your work?”
To enhance depth, participants were also asked to complete a free-association exercise by selecting an object or image they associated with SDOH and discussing its relevance.
As a framework, PTSS shaped both data collection and interpretation phases of the study. By linking the intergenerational impacts of slavery and structural racism to modern health inequities, PTSS provided a lens to examine the lived experiences of Black female HHS professionals. This framework guided the development of the interview guide, ensuring that questions captured both the systemic and individual dimensions of health inequities.
Interviews were transcribed verbatim and analyzed using open coding, as outlined by Charmaz
| [7] | Charmaz, Kathy. 2008. “Grounded Theory as an Emergent Method.” In Handbook of Emergent Methods, edited by S. N. Hesse-Biber and P. Leavy, 155–72. New York: The Guilford Press. https://doi.org/10.5172/conu.2010.37.1.092. |
[7]
. This grounded theory approach allowed emergent themes to surface organically from the data. Initial coding focused on identifying key phrases and concepts related to PTSS, historical trauma, and SDOH. Axial coding was then employed to identify relationships between these codes, leading to the development of higher-order themes.
Three primary these emerged from the data:
1) Historical Erasure in Health Education: Participants consistently emphasized the absence of historical context in SDOH trainings and its impact on perpetuating health disparities.
2) Embodiment of PTSS: Many participants described their lived experiences as encapsulating the intergenerational effects of trauma, which shaped their professional roles and personal health.
3) Resistance as Praxis: Participants reframed resilience as resistance, highlighting their efforts to challenge systemic barriers within their institutions and communities.
These themes were derived through iterative analysis, with recurring patterns validated across multiple participant narratives. The free-association exercise provided additional context, linking participants’ symbolic association to their lived experiences and professional insights. PTSS also informed the analysis, with coding strategies focusing on identifying instances of historical trauma, systemic inequities, and participant strategies for resistance. This approach ensures that PTSS was not merely a theoretical framework but a practical tool for interpreting participant experiences and deriving actional insights.
3. Results
3.1. The Invisible American History
In February 2020, Black British professor Dr. Kehinde Andrews sparked controversy when he argued that "whiteness is a psychosis" and compared the British Empire to Nazi Germany on Good Morning Britain. This remark enraged hosts Piers Morgan and Susanna Reid, who labeled Andrews a racist. Despite their criticism, Andrews stood firm, pointing out that the British Empire last longer, did more damage and paved the way for the Nazi’s genocidal ideology. He argued, “We do no favors to the victims of the Holocaust by pretending otherwise. If we forget the past, we are likely to repeat it”
Andrews’ stance was not a one-off. He had previously debated the legacy of Winston Churchill with Morgan and others, challenging the often-one-sided narrative of British heroism in World War II. Andrews emphasized the contributions of individuals from India, Africa, and the Caribbean, whose families had suffered due to Churchill’s rationing decisions. He highlighted that Britain’s history was deeply rooted in racism, a theme that Morgan and Reid could not fully grasp or accept. Andrews's response to their question of why he still lived in Britain, despite his critique, was pointed: “Where would I go?” He argued that there was no place on earth where Black people had not been devastated by British colonialism. While the conversation veered into a comparison of Britain and the United States, the underlying issue became clear: the erasure and distortion of history, particularly related to racism, colonialism, and slavery, was endemic to both countries.
3.2. America’s Real Problem
While Andrews’ critique focused on Britain, the U.S. faces its own version of historical amnesia. The extensive history of slavery, colonialism, and systemic racial injustice is often downplayed or framed as irrelevant to contemporary racial dynamics. Public discourse around racism typically centers on concepts like white privilege, implicit bias, and structural racism —important though they may be — but fails to acknowledge the persistent and explicit racial discrimination that continues to shape modern society. As historian Jamelle Bouie notes, “Racial inequality is about the structure of our society,” but it is also about how ordinary bias and discrimination play out in everyday life. This ongoing racial injustice is not a relic of the past; it is a live force that reproduces disadvantage
.
The 2023 Supreme Court ruling that ended race-conscious admissions in higher education is a striking example of this erasure. Justice Clarence Thomas’s concurring opinion, which argued that affirmative action policies contradicted the "colorblind" Constitution, overlooked the historical reality that the Constitution has never been colorblind. From the Three-Fifths Compromise to discriminatory policies like redlining, segregation, and mass incarceration, the U.S. Constitution was, and still is, deeply intertwined with racial injustice
.
The healthcare system is a perfect example of how these historical injustices continue to manifest in contemporary life. The concept of SDOH is frequently discussed as a way of addressing health inequities. However, this discourse often fails to account for the historical context that underpins current disparities. In an interview with Alexa Canady, she reflects on how challenging it is to address systemic issues within healthcare, which is itself deeply embedded in a history of racism and inequality
| [12] | Presumey-Leblanc, G. (2020, November 23). Rewriting the Present: Post Traumatic Slave Syndrome as a Foundation for Social Determinants of Health. OpenBU. https://open.bu.edu/handle/2144/41716 |
[12]
.
Canady: I think [the healthcare system] is a crazymaking industry. And there are so many competing priorities, so how do I make this top of mine? I don’t know that I’ve been successful, but that’s sort of like my thinking. Going through [MLP SDOH] trainings have helped me try to think that through.
GPL: Well, I think you mentioned something really interesting about risk-averse. It’s actually something that’s came up in my literature and in my past interviews is that when you think about how the SDOH discourse has kind of made the marriage between the medical and the legal almost necessary, this idea that they want to challenge...and correct the system that has foundations and not of the best intentions — you know, racism, sexism, ableism, and any — ism that you can think of — and yet, both institutions, the medical and the legal, are very risk-averse...So, how do you go about changing the system, when the actual institutions...do not lend themselves to allowing for change. I think some of the things that you mentioned in terms of responsibility and value, is it when an individual feels like the responsibility and the value is on me to help change the system or does it require a collective group? ‘Cause I think MLPs are trying to do that, but it’s so much harder when you have to operate within that system and change it from within.
Canady: And I think it’s both. I think you need enough people who feel like...this is my human and moral responsibility, but you do need a critical mass. So, one of the things that I have actively tried to do in my [time] here is identify who are the other champions doing this work for our system. And they are there...we support each other. It does require a critical mass, and it requires different disciplines. So, like I’m not an MD and there are usually some MDs and maybe some nurses in leadership that are running hospitals, and they want to hear from their clinical colleagues. So, I need MDs in my corner or in this choir. But also bringing the public health perspective. One thing I think I bring to this workplace is my history working in public health, the health department, and other agencies and entities...I’m almost like the public health whisperer — what it feels like sometimes. And building bridges, but also communicating that this, a public health strategy, that’s consistent with a healthcare strategy. Here’s the shared win...Doing this work because it’s the right thing to do won’t get it done, even if people think it’s the right thing to do, if they agree on that. That is not the motivation. I am clear on that now…What can I immediately do? And at least with the programs that are under my control, how do we make them safe spaces and communicate that?
Medical-legal institutions, like the healthcare system, often fail to connect current health disparities with their historical roots. Instead, SDOH are framed as "cultural problems" (e.g., poverty) rather than as the result of historical discrimination, such as slavery, colonialism, and segregation. This lack of historical contextualization in healthcare prevents effective solutions from being implemented.
3.3. Historical Foundations of Health Inequities
Any meaningful discussion about health inequities in populations affected by slavery and colonialism must include historical contextualization. Scholars like DeGruy
| [2] | DeGruy, J. (2005). Post Traumatic Slave Syndrome: America’s Legacy of Enduring Injury and Healing (Newly Rev.). Joy DeGruy Publications Inc. |
[2]
have explored the intergenerational effects of trauma experienced by Black populations, particularly through the lens of PTSS
| [13] | Presumey-Leblanc, G & Sandel, M. (2022, March 4). Perpetuating Commodification of Suffering: How Social Determinants Framing Prolongs Historical Racial Inequities. Women’s Health Reports, 2(1), 116-122. https://doi.org/10.1089/whr.2021.0019 |
| [14] | Presumey-Leblanc, G. & Sandel, M. (2024). The Legacy of Slavery and the Socialization of Black Female Health and Human Services Workforce Members in Addressing Social Determinants of Health. Journal of Racial and Ethnic Health Disparities, 11(1), 192-202. https://doi.org/10.1007/s40615-023-01510-y |
[13, 14]
. Contemporary health disparities cannot be understood without considering the legacies of slavery and colonialism, which have created and perpetuated structural inequities. These historical legacies are woven into the fabric of medical-legal institutions and continue to shape health outcomes for marginalized groups.
As both Britain and the U.S. have constructed institutions on racially inequitable foundations, the failure to recognize this shared history only ensures that the past will continue to repeat itself. From redlining to environmental racism, the history of racial oppression is not just a series of isolated events but an ongoing process that shapes the present and the future
. This historical erasure is dangerous, as it allows systemic racism to continue unchecked, leaving minority populations to bear the brunt of its effects.
3.4. Resistant Minority Populations & Reimagining Symbols of Oppression
Presumey-Leblanc and Sandel
| [14] | Presumey-Leblanc, G. & Sandel, M. (2024). The Legacy of Slavery and the Socialization of Black Female Health and Human Services Workforce Members in Addressing Social Determinants of Health. Journal of Racial and Ethnic Health Disparities, 11(1), 192-202. https://doi.org/10.1007/s40615-023-01510-y |
[14]
actively chose not to label their Black female participants resilient, but as resistant warriors, calling attention to issues with the resilience argument, which implies passivity and not intentionality. Resilience praises and applauds Black people for having to struggle without regard or rectification for circumstances out of their control.
Perhaps, this is why Black women, like the study participants, have chosen to engage in system-challenging praxis themselves. For the Black women interviewees, resilience was constantly needed. Rebecca Davis Lee Crumpler worked with opioid-addicted patients at a prominent private Boston hospital, where she was the only dark-skinned woman in the office. For Sophia B. Jones, resilience was necessary in defying societal expectations. While Jocelyn Elders felt she had no other choice, but to be resilient as a Haitian immigrant. Paula A. Johnson certainly needed resilience to survive domestic abuse. These Black women sacrificed their bodies, their time, and their desires, rising above simple resilience. This equated to resistance.
This reimagining makes relevant the ways in which the disadvantaged often take matters into their hands when they realize those in power will never truly understand the struggle. Most white people feel they are not responsible for the horrors of slavery because they do not have to experience or engage with the ongoing repercussions. Their privilege acts as a veil behind which they pretend to not see the suffering of minority populations, while the medical-legal institutions commodify and profit from that suffering. This is why any discussion related to minority health disparities and negative SDOH must look past the pain, suffering, and oppression to examine the joy, celebration, and resistance. There is so much to learn from how minority populations turn their agony into jubilation. It is no wonder the study’s Black women felt they must burden and exhaust themselves to find superior ways to erase past pains, manage present consequences, and revolutionize future possibilities to ensure the patient populations with which they identified thrived.
3.5. Historical Inclusion in Health Education
There is a lack of literature on how American involvement in slavery and colonialism has shaped contemporary health outcomes and Black PTSS embodiment. While DeGruy’s work focused solely on Black men, the gendered experiences of Black women are just as important. How can the HHS workforce operationalize all Black experiences and historical inclusion?
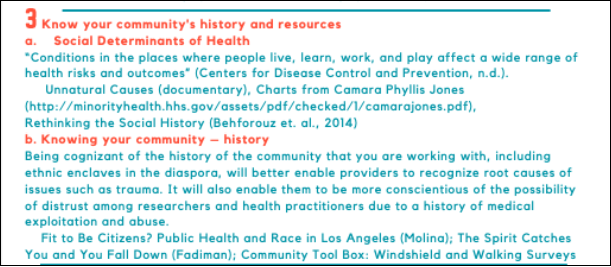
Figure 2. The Southern Jamaica Plains Health Center (SJPHC) Racial Justice and Health Equity Training. (Courtesy of Joycelyn Elders).
SJPHC Racial Justice and Health Equity training’s goal is to promote equitable treatment and health outcomes, which requires a deeper understanding of structural discrimination and how the HHS workforce can incorporate racial justice into health education and practice. There are five main operational principles:
1) Knowing the history of structural racism and white supremacy in medicine and public health,
2) Knowing and training yourself on the concepts of racial identity, racism, implicit bias, cultural competence versus cultural humility, and class distinctions,
3) Knowing your community’s history and resources,
4) Knowing the people on your team and acknowledging that critique of a system is not a personalized attack and that everyone is an expert on their own experiences,
5) Making the implicit explicit in the exam room to empower the patient and maximize the provider role.
Figure 3. The Southern Jamaica Plains Health Center (SJPHC) Racial Justice and Health Equity Training (Courtesy of Joycelyn Elders).
The third bullet point emphasizes the role history plays in the health of disadvantaged and underserved populations. Further information highlights the importance of knowing a community’s history, resources, and conceptions of SDOH.
Think Tuskegee Syphilis Study and Henrietta Lacks…
The SJPHC training is unique. Most people do not realize history and SDOH are inextricably linked. Health systems, centers like SJPHC, and public health organizations might consider adapting their current trainings to include education dedicated to historical legacies and its health impacts, ensuring instructors are community representatives with both clinical knowledge and lived experience.
The challenges of teaching elementary American history at the professional level necessitates what Presumey-Leblanc and Sandel call historical competency trainings, tailored to target specific communities. Hindered by time constraints, organizations are struggling to fit centuries of American history into short SDOH trainings.
3.6. Lessons from Black Women
The ethnographic study revealed Black women are both messages and messengers
| [12] | Presumey-Leblanc, G. (2020, November 23). Rewriting the Present: Post Traumatic Slave Syndrome as a Foundation for Social Determinants of Health. OpenBU. https://open.bu.edu/handle/2144/41716 |
[12]
. Based on their responses, it was clear the Black female study participants embodied PTSS and seemed to exhibit all the symptoms
| [14] | Presumey-Leblanc, G. & Sandel, M. (2024). The Legacy of Slavery and the Socialization of Black Female Health and Human Services Workforce Members in Addressing Social Determinants of Health. Journal of Racial and Ethnic Health Disparities, 11(1), 192-202. https://doi.org/10.1007/s40615-023-01510-y |
[14]
. They had all experienced negative SDOH. Their PTSS embodiments turn their Black bodies into historical time-capsules of racism and discrimination. The Black female study participants’ bodies and experiences act as reminders of the disadvantages and vulnerability of Black populations.
On the other hand, the women were also messengers. In their various HHS positions and leadership roles, they used their upbringings to make known the struggles of the patient populations with which they identified. They spoke out and operationalized their roles to make a difference, even if their work went unnoticed. These women make the best messengers because of their first-hand accounts and solo efforts — implementing new policies and creating novel strategies to challenge systems and improve population health
| [12] | Presumey-Leblanc, G. (2020, November 23). Rewriting the Present: Post Traumatic Slave Syndrome as a Foundation for Social Determinants of Health. OpenBU. https://open.bu.edu/handle/2144/41716 |
[12]
.
HHS policy makers and implementers could learn from Black female HHS workforce members. Black women have been championing strategies to increase racial and ethnic representation at both the personnel and administrative levels, creating a workforce so diverse the medical-legal institutions would be revolutionized and patients better served. Black female-led strategies are actionable and generalizable. Perhaps, with these potential solutions, the suffering of vulnerable populations will no longer be commodified for profit. The workforce should seek to remedy population suffering, so all people might achieve an attainable standard of health. HHS workforce members need to be more than simply color-blind.
In a separate dissent of the 2023 affirmative action case, Justice Katanji Brown Jackson wrote exactly what this article argues:
Our country has never been colorblind…Given the lengthy history of state-sponsored race-based preferences in America, to say that anyone is now victimized if a college considers whether that legacy of discrimination has unequally advantaged its applicants fails to acknowledge the well-documented intergenerational transmission of inequality that still plagues our citizenry
.
National Education Association President Becky Pringle said in a statement, “racism and discrimination are not just artifacts of American history but continue to persist in our society, including our schools, colleges, and universities”
. Medical-legal institutions are included as Justice Jackson states when history speaks, the impact of its words can be heard forever
. HHS workforce members must act as though they are abolitionists to dismantle and transform an oppressive system.
4. Conclusion: A Right to Knowing Our Health History
The acknowledgment of PTSS as the foundation for understanding minority SDOH experiences is a wonderful start. Some Black scholars and academics would call for monetary reparations, as Evanston, Illinois (the first U.S. city) and California (the first U.S. state) did in 2021, establishing reparation task forces
. However, the best apology is changed behavior. Nationally, this would call for an adoption of a right to health. The Universal Declaration of Human Rights (UDHR) details a right to health in Article 25
.
Although the USA is a country which boasts a language and bill of rights, they are negative — meaning the rights are meant to prohibit government interference, not encourage government obligation. The right to health in America only ensures the bare minimum is provided and that medical professionals do not act with deliberate indifference
. Should the federal government adopt more of a positive rights stance, there would be a transformative cultural overhaul in how population health is understood.
However, the right to health is not isolated. This right is inextricably linked to the right to education. Article 26 of the UDHR states,
2. Education should be directed to the full development of the human personality and to the strengthening of respect for human rights and fundamental freedoms. It shall promote understanding, tolerance and friendship among all nations, racial, or religious groups, and shall further the activities for the United Nations for the maintenance of peace.
Americans have long believed through hard work and grit any citizen can accomplish the American Dream. However, it is only through education one comes to understand how vulnerable populations have been unable to achieve the highest attainable standard of health. With this comprehension, the US government would not only recognize the right to health, but respect (refrain from denying or limiting equal access), protect (claim obligation for ensuring its citizens can use their right), and fulfill (provide adequate resources) this right. The highest attainable standard of health necessitates the equitable access and distribution of resources. Currently, what is missing from American education is certain populations have not had equitable social, educational, and economic capital access or distribution.
As it stands now, there is no way to ensure disadvantaged populations achieve an optimal standard of health. Health is tied to more than individual behaviors; it is related to primary goods — food and shelter, range of opportunities — education, and the unpredictable and uneven distribution of resources. In a country afraid of centralized federal government, federalism limits the ways in which those in power might act in the benefit of the most disadvantaged. This was only made worse by trickle-down economics and neoliberalism, which individualized health and welfare. Former President Ronald Reagan promoted the notion that by facilitating and consolidating resources at the top, the wealthy would use the extra “earned” money to create jobs, boost the economy, and spread the riches. It was then the duty of the poor to take advantage of the provided wealth. But it would seem they are still waiting for prosperity to make its way to the bottom.
The Trump administration attempted to dismantle programs like the Affordable Care Act (ACA), Social Security Income (SSI), Medicaid, Medicare, Supplemental Nutrition Assistance (SNAP), meant to help the indigent. Trump’s 2020 budget proposal called for a significant tax break to the top one percent by cutting from Medicaid, Medicare, and SSI. The efforts to cut SSI failed due to its popularity, which might show current social services are appreciated and utilized. For a bill like the ACA to be passed without challenge, Americans would need to recognize there exists a class distinction and notable wealth gap. Unfortunately, the government has invariably enacted policies which have worsened this divide. For example, the Federal-Aid Highway Act of 1956 used federal dollars to build transnational highways. While meant to benefit all citizens, it further separated minority urban neighborhoods from new white suburbs [2018]. The building of I-40 through Nashville was rerouted through the predominantly African-American North Nashville. Despite the continuing legal opposition, North Nashville has yet to recover from the economic devastation of I-40’s completion and remains one of the most medically underserved areas in the city
| [19] | Karas, D. (2015). Highway to Inequity: The Disparate Impact of the Interstate Highway System on Poor and Minority Communities in American Cities. New Visions for Public Affairs, 7(April), 9-21. |
[19]
.
Legally, racial minorities are a protected class, yet discrimination continues to occur at the institutional level. With the adoption of a right to health, Black Americans need not live in systemically encouraged poverty with few educational and economic opportunities. Under the premises of health and human rights, to improve health and minimize health inequities, Eric Friedman and Lawrence Fostin propose a four-part approach:
1) Incorporating right-to-health obligations and principles into national laws and policies,
2) Using Creative strategies to increase the impact of national right-to-health litigation,
3) Empowering communities to claim their right to health and building civil society’s health and human rights advocacy capacity, and
4) Bringing the right to health to the center of global governance for health
| [20] | Grodin, M. A. (2013). Health and Human Rights in a Changing World. Routledge. |
[20]
.
A right to health would ensure the government takes responsibility for systematically disadvantaged minority populations, like those who have been impacted by PTSS and historical trauma. The right to health would guarantee the liberation of the Black population from chains of the past, give them a pathway to climb social ladders, and actualize the American dream.
As Bradley and Taylor
| [21] | Bradley, E. H. & Taylor, L. A. (2013). The American Health Care Paradox: Why Spending More is Getting Us Less. (1st Ed.). Public Affairs. |
[21]
make clear in their book,
The American Health Care Paradox: Why Spending More Is Getting Us Less, while the United States is unlikely to invest in social services and the human services sector, there is still hope — a belief onto which study participants held. When DeGruy identified PTSS, she understood these adaptive behaviors to be a positive means of survival for the Black population and once identified, these behaviors could be utilized to move forward in healing, hoping, and reimagining better futures. Perhaps, the first step is to stop viewing the issue as a problem and start seeing people as the Full Frame Initiative suggests in their wellbeing framework
. This framework realizes the way to health and hope is by recognizing a universal set of needs, while acknowledging the individual context which drives personal choices. The initiative’s five domains of wellbeing — social connectedness, stability, safety, mastery, and meaningful access to relevant resources — are intertwined and dependent on an individual’s personal background.
The study had several limitations. First, while the concept of PTSS offers valuable insight, its application remains largely qualitative, with limited quantitative evidence to generalize findings on its impact on population health. Additionally, the focus on Black American experiences may overlook other marginalized communities who have faced similar traumas, suggesting the need for more inclusive research across different racial, ethnic, and generational groups. Methodologically, challenges arise from sampling bias, reliance on self-reported data, and the difficulty in established causal links between historical trauma and health outcomes, as many studies cannot fully separate the effects of PTSS from other social determinants of health. Furthermore, the measurement of PTSS is complicated by cultural differences, and existing tools may not fully capture its unique manifestation in diverse populations. The study also failed to address how structural inequities, such as income inequality and racial segregation, contribute to the perpetuation of trauma and health disparities. Additionally, translating theoretical frameworks, like the right to health, into actionable policies remains a significant hurdle in addressing systemic issues. Finally, long-term studies are necessary to understand the generational impact of PTSS and to evaluate the effectiveness of interventions in mitigating its effects over time. These limitations highlight the need for multifaceted approach, combining longitudinal research, diverse sampling, and structural reforms to better address the health consequences of historical trauma.
Future research should focus on examining the long-term health impacts of PTSS, including mental health, chronic illness, and other SDOH. Studies should further explore how healthcare systems can be restructured to support healing for populations suffering from historical trauma. Furthermore, there needs to be more robust advocacy for the integration of health as a fundamental human right, not just in policy but also in practice, ensuring that Black Americans and other marginalized groups have the resources, education, and support needed to thrive.
This model is dedicated to seeing both individuals and communities move from surviving to thriving. For too long, HHS has been okay with allowing marginalized populations to survive. But there are organizations already doing the work and reframing narratives of wellbeing, wholeness, and prosperity for populations that have been chasing healing and hope. Perhaps, these are the places best suited to begin the process of PTSS integration and institutional transformation. To successfully achieve healing and hope, the injustices of the past must be acknowledged and rectified, a positive right to health respected, protected, and fulfilled, and the adaptive behaviors of PTSS and historical trauma recognized, so all individuals may gain equitable access to the tools and resources needed to do more than just survive. Then, and only then, will the most vulnerable of society hope to thrive in the future. Knowing one’s history is paramount in understanding present population health and future thriving.
Abbreviations
AP | Advanced Placement |
HHS | Health and Human Services |
MLP | Medical-Legal Partnership |
PTSS | Post Traumatic Slave Syndrome |
SDOH | Social Determinants of Health |
SJPHC | The Southern Jamaica Plains Health Center |
Acknowledgments
Not Applicable.
Ethics Approval & Consent to Participate
This study was performed in line with the principles of the Declaration of Helsinki. Approval was granted by the Ethics Committee of Boston University and by the Boston University Medical Campus and Boston Medical Center Institutional Review Board. (Date: 4-29-2019/IRB Number: H-38535).
Verbal informed consent was obtained from all individual participants included in the study at the beginning of each recorded interview. Due to the limited harm of the qualitative study, the Ethics Committees of Boston University and Boston Medical Center Institutional Review Board only necessitated verbal consent. Research was conducted from April 2019 to October 2019.
Consent for Publication
The authors affirm that human research participants provided informed consent for publication of all images or figures.
Author Contributions
All authors contributed to the study's conception and design. Material preparation, data collection and analysis were performed by Garssandra Presumey-Leblanc and Dr. Megan Sandel. The first draft of the manuscript was written by Garssandra Presumey-Leblanc and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Funding
The authors declare that no funds, grants, or other support were received during the preparation of this manuscript.
Conflicts of Interest
The authors declare no conflicts of interest.
References
| [1] |
Yousif, N. (2023, January 20). Ron DeSantis Government Bans New Advanced African American History Course. BBC News.
https://www.bbc.com/news/world-us-canada-64348902
|
| [2] |
DeGruy, J. (2005). Post Traumatic Slave Syndrome: America’s Legacy of Enduring Injury and Healing (Newly Rev.). Joy DeGruy Publications Inc.
|
| [3] |
Hanks, A., Solomon, D. & Weller, C. E. (2018, February 21). Systemic Inequality: How America’s Structural Racism Helped Create the Black-White Wealth Gap. Center for American Progress.
http://www.americanprogress.org/issues/race/reports/2018/02/21/1447051/systenic-inequaity/
|
| [4] |
Bailey, M. (2010). The Intersectional Invisibility of Black Women: Misogynoir and the Multiple Marginalization of African American women. Journal of Black Studies, 41(3), 327-353.
https://doi.org/10/1177/0021934709357882
|
| [5] |
Crenshaw, K. (1991). Mapping the Margins: intersectionality, Identity Politics, and Violence Against Women of Color. Stanford Law Review (43(6), 1241-1299.
https://doi.org/10.2307.1229039
|
| [6] |
Rosenthal, L. & Lobel, M. (20110, Explaining Disparities in Adverse Birth Outcomes: The Contributions of Maternal Stress and Coping. In S. K. M. K. S. McNaughton, L. L. G. Engle, & P. W. G. Shaw (Eds.), Psychology of Stress and Coping in Health (pp. 125-147). Cambridge University Press.
https://doi.org/10/1017/CBO9780511976763.010
|
| [7] |
Charmaz, Kathy. 2008. “Grounded Theory as an Emergent Method.” In Handbook of Emergent Methods, edited by S. N. Hesse-Biber and P. Leavy, 155–72. New York: The Guilford Press.
https://doi.org/10.5172/conu.2010.37.1.092.
|
| [8] |
Atwell, A. (2020, February 5). Video: Black Professor Unleashes Flood of White Tears After On-Air Clash Ensues When Guest says the British Empire ‘Wasn’t All Bad’. Atlanta Black Star.
https://atlantablackstar.com/2020/02/05/video-black-professor-unleashes-flood-of-white-tears-after-on-air-clash-ensues-when-guest-says-the-british-empire-wasnt-all-bad/
|
| [9] |
Bouie, J. (2019, November 22). Opinion: The Racism Right Before Our Eyes. The New York Times.
http://www.nytinmes.com/2019/11/22/opinion/racism-housing-jobs.html?auth=login-google
|
| [10] |
Editors of Encyclopaedia Britannica. (2023, August 23). Three-Fifths Compromise. Encyclopaedia Britannica.
https://www.britannica.com/topic/three-fifths-compromise
|
| [11] |
Totenberg, N. (2023, June 29). Supreme Court Guts Affirmative Action, Effectively Ending Race-Conscious Admissions. NPR.
https://www.npr.org/2023/06/29/1181138066/affrmative-action-supreme-court-decision
|
| [12] |
Presumey-Leblanc, G. (2020, November 23). Rewriting the Present: Post Traumatic Slave Syndrome as a Foundation for Social Determinants of Health. OpenBU.
https://open.bu.edu/handle/2144/41716
|
| [13] |
Presumey-Leblanc, G & Sandel, M. (2022, March 4). Perpetuating Commodification of Suffering: How Social Determinants Framing Prolongs Historical Racial Inequities. Women’s Health Reports, 2(1), 116-122.
https://doi.org/10.1089/whr.2021.0019
|
| [14] |
Presumey-Leblanc, G. & Sandel, M. (2024). The Legacy of Slavery and the Socialization of Black Female Health and Human Services Workforce Members in Addressing Social Determinants of Health. Journal of Racial and Ethnic Health Disparities, 11(1), 192-202.
https://doi.org/10.1007/s40615-023-01510-y
|
| [15] |
Walsh, M. “(2023, July 29). Supreme Court Ends Affirmative Action in College Admissions in Decision Watched by K-12. Education Week.
https://www.edweek.org/policy-politics/supreme-court-ends-affirmative-action-in-college-admissions-in-decision-wwatched-by-k-12/2023/06
|
| [16] |
Blazina, C. & Cox, K. (2022, November 28). Black and White Americans Are Fast Apart in Their Views of Reparations for Slavery. Pew Research Center.
https://www.pewresearch.org/short-reads/2022/11/28/black-and-white-americans-are-far-apart-in-their-views-of-reparations-for-slavery/
|
| [17] |
UN General Assembly. (1948). Universal Declaration of Human Rights. The United Nations.
https://doi.org/10.5195/rt.2019.591
|
| [18] |
Estelle v. Gamble, 429 U.S. 97 (1976). Justia Law. Retrieved January 14, 2023, from
https://supreme.justia.com/cases/federal/us/429/97/
|
| [19] |
Karas, D. (2015). Highway to Inequity: The Disparate Impact of the Interstate Highway System on Poor and Minority Communities in American Cities. New Visions for Public Affairs, 7(April), 9-21.
|
| [20] |
Grodin, M. A. (2013). Health and Human Rights in a Changing World. Routledge.
|
| [21] |
Bradley, E. H. & Taylor, L. A. (2013). The American Health Care Paradox: Why Spending More is Getting Us Less. (1st Ed.). Public Affairs.
|
| [22] |
The Full Frame Initiative. (2020). The Full Frame Approach and the Five Domains of Wellbeing. The Full Frame Initiative.
https://fullframeinitiative.org/resources/about-the-full-frame-approach-and-five-domains/#video
|
Cite This Article
-
APA Style
Presumey-Leblanc, G., Sandel, M. (2025). Black History Matters: Integrating Post Traumatic Slave Syndrome into SDOH Trainings to Enhance Health Equity. American Journal of Health Research, 13(1), 47-56. https://doi.org/10.11648/j.ajhr.20251301.14
 Copy
|
Copy
|
 Download
Download
ACS Style
Presumey-Leblanc, G.; Sandel, M. Black History Matters: Integrating Post Traumatic Slave Syndrome into SDOH Trainings to Enhance Health Equity. Am. J. Health Res. 2025, 13(1), 47-56. doi: 10.11648/j.ajhr.20251301.14
Copy
|
Download
AMA Style
Presumey-Leblanc G, Sandel M. Black History Matters: Integrating Post Traumatic Slave Syndrome into SDOH Trainings to Enhance Health Equity. Am J Health Res. 2025;13(1):47-56. doi: 10.11648/j.ajhr.20251301.14
Copy
|
Download
-
@article{10.11648/j.ajhr.20251301.14,
author = {Garssandra Presumey-Leblanc and Megan Sandel},
title = {Black History Matters: Integrating Post Traumatic Slave Syndrome into SDOH Trainings to Enhance Health Equity
},
journal = {American Journal of Health Research},
volume = {13},
number = {1},
pages = {47-56},
doi = {10.11648/j.ajhr.20251301.14},
url = {https://doi.org/10.11648/j.ajhr.20251301.14},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ajhr.20251301.14},
abstract = {This study aimed to examine the integration of Post-Traumatic Slave Syndrome (PTSS) into Social Determinants of Health (SDOH) trainings as a means to enhance the understanding and addressing of health disparities, particularly among Black populations. Given the growing emphasis on SDOH in health education, the study sought to explore how historical trauma, specifically PTSS, contributes to ongoing health inequities and to evaluate whether its inclusion in training could lead to more culturally informed approaches in health and human services (HHS). Through ethnographic interviews with six Black female professionals in Massachusetts and Rhode Island, who had participated in SDOH trainings organized by a medical-legal partnership (MLP), the research aimed to uncover the connections between historical trauma and health disparities in the context of contemporary healthcare. By highlighting the lived experiences of professionals and their perspectives on PTSS, the study also sought to propose methods for incorporating these historical dimensions into current SDOH frameworks to foster deeper, more systemic change. The findings suggest that integrating PTSS within SDOH education is essential for developing comprehensive strategies to promote health equity and advance social justice in medical-legal collaborations.
},
year = {2025}
}
Copy
|
Download
-
TY - JOUR
T1 - Black History Matters: Integrating Post Traumatic Slave Syndrome into SDOH Trainings to Enhance Health Equity
AU - Garssandra Presumey-Leblanc
AU - Megan Sandel
Y1 - 2025/02/17
PY - 2025
N1 - https://doi.org/10.11648/j.ajhr.20251301.14
DO - 10.11648/j.ajhr.20251301.14
T2 - American Journal of Health Research
JF - American Journal of Health Research
JO - American Journal of Health Research
SP - 47
EP - 56
PB - Science Publishing Group
SN - 2330-8796
UR - https://doi.org/10.11648/j.ajhr.20251301.14
AB - This study aimed to examine the integration of Post-Traumatic Slave Syndrome (PTSS) into Social Determinants of Health (SDOH) trainings as a means to enhance the understanding and addressing of health disparities, particularly among Black populations. Given the growing emphasis on SDOH in health education, the study sought to explore how historical trauma, specifically PTSS, contributes to ongoing health inequities and to evaluate whether its inclusion in training could lead to more culturally informed approaches in health and human services (HHS). Through ethnographic interviews with six Black female professionals in Massachusetts and Rhode Island, who had participated in SDOH trainings organized by a medical-legal partnership (MLP), the research aimed to uncover the connections between historical trauma and health disparities in the context of contemporary healthcare. By highlighting the lived experiences of professionals and their perspectives on PTSS, the study also sought to propose methods for incorporating these historical dimensions into current SDOH frameworks to foster deeper, more systemic change. The findings suggest that integrating PTSS within SDOH education is essential for developing comprehensive strategies to promote health equity and advance social justice in medical-legal collaborations.
VL - 13
IS - 1
ER -
Copy
|
Download