Abstract
Non-communicable diseases (NCDs) pose a significant public health challenge in Sub-Saharan Africa, where traditional healthcare systems in Sub-Saharan Africa often grapple with limited infrastructure, healthcare worker shortages, and accessibility challenges. Mobile health (mHealth) interventions have emerged as promising tools to enhance health promotion and literacy, providing innovative solutions to these challenges. This study evaluates the feasibility and effectiveness of cross-country mHealth interventions through a secondary analysis of the NCD 365 project, which utilized outcome data from January to December 2020. A multi-stage sampling technique was employed to select participants from five countries, and data were collected via an online Google form. The analysis focused on platform usage, literacy distribution, and the relationship between health literacy levels and the platforms used. Descriptive statistics and the Kruskal-Wallis test were used to evaluate the data. Results indicated that WhatsApp was the most widely used platform in four of the five countries, while Twitter predominated in Uganda. Adjusted literacy levels varied slightly, with Kenya and Nigeria showing higher levels compared to Cameroon, Zimbabwe, and Uganda. Gender differences in literacy were minimal, with males displaying marginally higher literacy scores. The Kruskal-Wallis test revealed no significant differences in literacy levels across platforms or countries, reinforcing the feasibility and effectiveness of cross-country mHealth interventions. These findings suggest that initiatives like the NCD 365 project can effectively promote health literacy and healthcare delivery across diverse settings in Sub-Saharan Africa. While regional differences in platform preferences exist, the overall success of the project highlights the potential for scalable and adaptable mHealth strategies. Future research should focus on the long-term impacts and platform-specific effectiveness to further optimize mHealth interventions.
|
Published in
|
American Journal of Health Research (Volume 13, Issue 1)
|
|
DOI
|
10.11648/j.ajhr.20251301.12
|
|
Page(s)
|
28-42 |
|
Creative Commons
|

This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited.
|
|
Copyright
|
Copyright © The Author(s), 2025. Published by Science Publishing Group
|
Keywords
Non-communicable Diseases (NCDs), Mobile Health (mHealth), Health Promotion, Health Literacy, Cross-Country Interventions, Digital Health Platforms, Sub-Saharan Africa
1. Introduction
1.1. Health Promotion
Health promotion involves enabling individuals to gain control over their health and its determinants, thereby enhancing their health.
| [1] | Kidanemariam, A. (2011). RETHINKING HEALTH PROMOTION AND DISEASE PREVENTION IN AFRICA: THE QUEST FOR AN INTEGRATED MODEL. [online] Available at: https://www.jstor.org/stable/45198650 |
[1]
Various strategies are employed in health promotion, including education and awareness campaigns that educate people about healthy lifestyles and the importance of maintaining good health
| [2] | Kumar, S. and Preetha, G. (2022). Health promotion: an Effective Tool for Global Health. Indian Journal of Community Medicine, [online] 37(1), pp. 5–12. https://doi.org/10.4103/0970-0218.94009 |
[2]
. Additionally, policies and legislation that support structural health determinants and environments play a crucial role. For instance, laws mandating restaurants to provide nutritional information on menus or prohibiting smoking in public places promote healthy behaviors
| [3] | Seppälä, T., Hankonen, N., Korkiakangas, E., Ruusuvuori, J. and Laitinen, J. (2017). National policies for the promotion of physical activity and healthy nutrition in the workplace context: a behaviour change wheel guided content analysis of policy papers in Finland. BMC Public Health, 18(1). https://doi.org/10.1186/s12889-017-4574-3 |
[3]
.
In Sub-Saharan Africa, the area and regions of the continent of Africa that lie south of the Sahara, poor infrastructure, such as inadequate roads, transportation, and communication systems, hinders the reach of health promotion programs, especially in rural or remote areas. Political instability and conflict further complicate these efforts
| [4] | Azevedo, M. J. (2019). The State of Health System(s) in Africa: Challenges and Opportunities. Historical Perspectives on the State of Health and Health Systems in Africa, Volume II, [online] 2, pp. 1–73. https://doi.org/10.1007/978-3-319-32564-4_1 |
[4]
. Despite these obstacles, health promotion remains a vital component in improving health literacy and overall population health.
1.2. Health Literacy
Health literacy refers to the capacity of individuals to obtain, process, and understand basic health information and services needed to make appropriate health decisions
. It is crucial for health promotion, as higher levels of health literacy lead to improved self-health behaviors and utilization of healthcare services.
In Sub-Saharan Africa, health literacy poses significant challenges. Barriers include language difficulties, poor infrastructure, limited education, and cultural differences
| [4] | Azevedo, M. J. (2019). The State of Health System(s) in Africa: Challenges and Opportunities. Historical Perspectives on the State of Health and Health Systems in Africa, Volume II, [online] 2, pp. 1–73. https://doi.org/10.1007/978-3-319-32564-4_1 |
[4]
. These barriers hinder individuals' ability to comprehend and use health information effectively, impacting their health outcomes. Cross-country mHealth interventions involve the use of mobile and digital technologies to deliver health promotion, education, and services across multiple countries or regions. These initiatives leverage platforms such as apps, social media, and messaging services to address shared health challenges, like non-communicable diseases, in diverse settings. By facilitating collaboration and resource sharing, cross-country mHealth interventions aim to enhance health outcomes and bridge gaps in health literacy across borders.
1.3. eHealth and mHealth
eHealth involves using digital technologies to support health and healthcare, encompassing websites, apps, telemedicine, and electronic health records. These technologies improve healthcare efficiency, effectiveness, and accessibility
. eHealth enhances communication, provides access to health information, and supports self-management. For example, telemedicine enables virtual consultations, and electronic health records facilitate easier sharing of patient information
| [6] | Sanders, M., Tobin, J. N., Cassells, A., Carroll, J., Holder, T., Thomas, M., Luque, A. and Fiscella, K. (2020). Can a brief peer-led group training intervention improve health literacy in persons living with HIV? Results from a randomized controlled trial. Patient Education and Counseling. https://doi.org/10.1016/j.pec.2020.10.031 |
[6]
.
mHealth, or mobile health, leverages portable electronic devices like smartphones or wearable technology to deliver healthcare services and information. Unlike eHealth, mHealth focuses specifically on mobile technology to enhance healthcare delivery, particularly in resource-limited settings. Applications include mobile health monitoring, disease management apps, and mobile-based patient-provider communication. mHealth has the potential to revolutionize healthcare delivery in low- and middle-income countries
.
mHealth is closely linked to health literacy, as users must have the skills to access and interpret information correctly. Evaluations of various mHealth applications indicate that these technologies can enhance health literacy by providing accessible, easy-to-understand health information and supporting chronic condition self-management
| [6] | Sanders, M., Tobin, J. N., Cassells, A., Carroll, J., Holder, T., Thomas, M., Luque, A. and Fiscella, K. (2020). Can a brief peer-led group training intervention improve health literacy in persons living with HIV? Results from a randomized controlled trial. Patient Education and Counseling. https://doi.org/10.1016/j.pec.2020.10.031 |
[6]
.
1.4. Non-Communicable Diseases
Non-communicable diseases (NCDs), such as diabetes, cardiovascular disease, and cancer, are a major global health burden, responsible for 74% of deaths worldwide and leading to significant disability
. In Sub-Saharan Africa, the burden of NCDs is particularly high due to prevalent risk factors like tobacco use, unhealthy diet, and physical inactivity, coupled with limited capacity to prevent, diagnose, and treat these diseases
| [9] | Gouda, H. N., Charlson, F., Sorsdahl, K., Ahmadzada, S., Ferrari, A. J., Erskine, H., Leung, J., Santamauro, D., Lund, C., Aminde, L. N., Mayosi, B. M., Kengne, A. P., Harris, M., Achoki, T., Wiysonge, C.S., Stein, D. J. and Whiteford, H. (2019). Burden of non-communicable diseases in sub-Saharan Africa, 1990–2017: results from the Global Burden of Disease Study 2017. The Lancet Global Health, 7(10), pp.e1375–e1387. https://doi.org/10.1016/s2214-109x(19)30374-2 |
[9]
.
Addressing the high burden of NCDs in Sub-Saharan Africa requires increased awareness, improved access to prevention, diagnosis, and treatment services, and addressing underlying social, economic, and environmental determinants
. Health literacy plays a crucial role in this comprehensive approach, enabling individuals to access and utilize healthcare services effectively and maintain good health.
1.5. Research Context
In 2020, a project named NCDs 365 was established in Sub-Saharan Africa, involving eight partner countries: Kenya, Uganda, Tanzania, Ethiopia, Cameroon, Senegal, Zimbabwe, and Malawi.
1.5.1. The NCDs 365 Project Phase 1: 2020
The project involved daily dissemination of 366 posters and text messages on various NCDs, each month focusing on a unique them as indicated in
table 1:
Table 1. NCDs 365 thematic focus areas.
Month | Thematic Focus |
January | Introduction to NCDS. Learning the basics |
February | Cancer, coinciding with the World Cancer Day Celebration |
March | Drugs and Substance Abuse and NCDS |
April | NCDS and COVID 19. Educating on the link between NCDs and COVID |
May | Cardiovascular Diseases in line with May is May Measurement Month. |
June | Diabetes and exploring its link to COVID 19 |
July | Mental Health with focus on the depression, anxiety among people. |
August | Chronic Kidney Diseases. |
September | Sickle Cell Disease. |
October | Childhood Obesity. |
November | Less talked about NCDs |
December | NCDs prevention tips. |
Initially, five countries participated, with implementing partners being membership organizations like community-based organizations (CBOs) and civil society organizations (CSOs). These organizations shared content daily on social media platforms and reported monthly reach. A survey conducted at the end of the year among the implementing partners provided the basis for this study.
1.5.2. Study Setting
The study was conducted in five African countries: Kenya, Uganda, Nigeria, Cameroon, and Zimbabwe, selected for having implemented the project for the entire calendar year 2020. These countries represent major regions within Sub-Saharan Africa and are significant contributors to the region's health landscape.
1.6. Aim and Objectives
This study aims to investigate the impact of a specific mHealth intervention on improving health literacy levels with a focus on non-communicable diseases. The objective was to assess the feasibility and effectiveness of implementing cross-country mHealth interventions for health promotion in Sub-Saharan Africa.
2. Literature Review
2.1. mHealth and Health Literacy: Global to Local Perspective
The World Health Organization (WHO) defines mHealth as "medical and public health practice supported by mobile devices, such as mobile phones, patient monitoring devices, personal digital assistants (PDAs), and other wireless devices"
. Health literacy, on the other hand, is described as “the achievement of a level of knowledge, personal skills, and confidence to take action to improve personal and community health by changing personal lifestyles and living conditions”
| [10] | Agner, J., KathArine Elizabeth Bau and Bruland, D. (2024). An Introduction to Health Literacy and Social Contexts with Recommendations for Health Professionals and Researchers. International Journal of Environmental Research and Public Health, 21(2), pp.240–240. https://doi.org/10.3390/ijerph21020240 |
[10]
.
The effectiveness of mHealth interventions is closely linked to health literacy. For mHealth applications to be effective, the information conveyed through mobile media must align with the unique health communication needs, orientations, and skills of the intended audience
| [11] | Kreps GL (2017). The Relevance of Health Literacy to mHealth. Studies in health technology and informatics, [online] 240. Available at: https://pubmed.ncbi.nlm.nih.gov/28972527/ [Accessed 6 Aug. 2024]. |
[11]
. Studies have shown that health literacy levels significantly influence an individual's ability to properly take medications, understand labels and health messages, and overall health status
| [12] | Berkman, N., Sheridan, S., Donahue, K., Halpern, D. and Crotty, K. (2011). Low health literacy and health outcomes: An updated systematic review. [online] Annals of Internal Medicine. Available at: https://pubmed.ncbi.nlm.nih.gov/21768583/ |
| [13] | Kim, H. and Xie, B. (2017). Health literacy in the eHealth era: A systematic review of the literature. Patient Education and Counseling, 100(6), pp. 1073–1082. https://doi.org/10.1016/j.pec.2017.01.015 |
[12, 13]
. Implementing mHealth interventions can enhance health literacy, subsequently improving associated health outcomes
| [14] | Lin, YH and Lou, MF eds., (2016). Effects of mHealth-based interventions on health literacy and related factors: A systematic review. [online] Europepmc.org. Available at: https://europepmc.org/article/med/33040429 [Accessed 6 Aug. 2024]. |
[14]
.
In recent years, mHealth has emerged as a powerful tool for global health communication, showing its potential to enhance healthcare delivery, broaden access to information and services, and reduce costs in both developed and developing nations
| [15] | Iribarren, S. J., Cato, K., Falzon, L. and Stone, P.W. (2017). What is the economic evidence for mHealth? A systematic review of economic evaluations of mHealth solutions. PLOS ONE, 12(2), p.e0170581. https://doi.org/10.1371/journal.pone.0170581 |
| [16] | Marcolino, M. S., Oliveira, J. A. Q., D’Agostino, M., Ribeiro, A. L., Alkmim, M. B. M. and Novillo-Ortiz, D. (2018). The Impact of mHealth Interventions: Systematic Review of Systematic Reviews. JMIR mHealth and uHealth, [online] 6(1), p.e23. https://doi.org/10.2196/mhealth.8873 |
[15, 16]
. mHealth is particularly promising in low- and middle-income countries, such as those in Sub-Saharan Africa, where traditional healthcare infrastructure may be limited
| [15] | Iribarren, S. J., Cato, K., Falzon, L. and Stone, P.W. (2017). What is the economic evidence for mHealth? A systematic review of economic evaluations of mHealth solutions. PLOS ONE, 12(2), p.e0170581. https://doi.org/10.1371/journal.pone.0170581 |
[15]
. The widespread adoption of mobile technology in Sub-Saharan Africa presents opportunities to leverage mHealth solutions to improve healthcare delivery, disease management, and health promotion. A summary of studies showing use of mhealth in low- to middle-income countries can be seen in
table 4 below:
Table 4. Studies Showing Use of mHealth in Low- to Middle-Income Countries.
Author | Study Type | Country | Intervention | Outcome |
Ali & Prins (2020) | [17] | Ali, A. O. A. and Prins, M. H. (2020). Patient Characteristics Associated with Non-Adherence to Tuberculosis Treatment: A Systematic Review. Journal of Tuberculosis Research, [online] 08(02), pp. 73–92. https://doi.org/10.4236/jtr.2020.82008 |
[17] | RCT | Sudan | SMS to remind TB patients to adhere to treatment vs. control group | Intervention group showed reduced default rate (6.8% vs. 10.8%, P=0.563) and higher cure rate (78.4% vs. 59.5%, P=0.020). |
Murthy et al. (2019) | [18] | Murthy, N., Chandrasekharan, S., Prakash, M. P., Ganju, A., Peter, J., Kaonga, N. and Mechael, P. (2020). Effects of an mHealth voice message service (mMitra) on maternal health knowledge and practices of low-income women in India: findings from a pseudo-randomized controlled trial. BMC Public Health, 20(1). https://doi.org/10.1186/s12889-020-08965-2 |
[18] | Pseudo RCT | India | Voice messaging to pregnant women to improve infant care practices | Improved feeding practices at 6 months (OR 1.4, 95% CI 1.08–1.82, p=0.009) and immunization status (OR 1.531, 95% CI 1.141–2.055, p=0.005). |
Jahan et al. (2020) | [19] | Jahan, Y., Rahman, M. M., Faruque, A. S. G., Chisti, M. J., Kazawa, K., Matsuyama, R. and Moriyama, M. (2020). Awareness Development and Usage of Mobile Health Technology Among Individuals With Hypertension in a Rural Community of Bangladesh: Randomized Controlled Trial. Journal of Medical Internet Research, 22(12), p.e19137. https://doi.org/10.2196/19137 |
[19] | RCT | Bangladesh | SMS messages and health education on lifestyle for hypertension patients | Greater adherence in salt intake (P=0.04) and physical activity (P<0.03) in control group, significant improvement in primary outcome of salt intake (P<0.001). |
Ben-Zeev et al. (2021) | [20] | Ben-Zeev, D., Chander, A., Tauscher, J., Buck, B., Nepal, S., Campbell, A. and Doron, G. (2021). A Smartphone Intervention for People With Serious Mental Illness: Fully Remote Randomized Controlled Trial of CORE. Journal of Medical Internet Research, 23(11), p.e29201. https://doi.org/10.2196/29201 |
[20] | RCT | Nepal | Smartphone app promoting daily exercise for psychiatric patients | Significant treatment×time interactions for BDI-II, GAD-7, RAS, RSES, and SDS, with patients finding the app highly usable and acceptable. |
2.2. Cross-Country mHealth Interventions
One of the primary advantages of mHealth interventions is their ability to be implemented across different countries and regions, providing a cost-effective method of delivering healthcare services to populations in need. mHealth interventions have the potential to reduce costs associated with traditional healthcare delivery methods, such as infrastructure, personnel, and equipment. This makes mHealth increasingly popular among global health organizations and governments aiming to improve healthcare access and outcomes.
The COVID-19 pandemic underscored the importance of mHealth in promoting health and preventing the spread of infectious diseases. Regional bodies like WHO's African Region (WHO AFRO) and the Centers for Disease Control and Prevention (CDC) implemented mHealth campaigns to promote health and prevent COVID-19 spread
. For instance, Africa's response included using mobile technology for contact tracing, case management, and community engagement
| [22] | Nachega, Jean B et al. “Contact Tracing and the COVID-19 Response in Africa: Best Practices, Key Challenges, and Lessons Learned from Nigeria, Rwanda, South Africa, and Uganda.” The American journal of tropical medicine and hygiene vol. 104, 4 1179-1187. 11 Feb. 2021, https://doi.org/10.4269/ajtmh.21-0033 |
[22]
. Similarly, the CDC's mHealth campaign in Nigeria promoted HIV testing and counseling services
| [23] | Jahun, I., Said, I., El-Imam, I., Ehoche, A., Dalhatu, I., Yakubu, A., Greby, S., Bronson, M., Brown, K., Bamidele, M., Boyd, A.T., Bachanas, P., Dirlikov, E., Agbakwuru, C., Abutu, A., Williams-Sherlock, M., Onotu, D., Odafe, S., Williams, D.B. and Bassey, O. (2021). Optimizing community linkage to care and antiretroviral therapy Initiation: Lessons from the Nigeria HIV/AIDS Indicator and Impact Survey (NAIIS) and their adaptation in Nigeria ART Surge. PloS One, [online] 16(9), p.e0257476. https://doi.org/10.1371/journal.pone.0257476 |
[23]
. During the 2014 Ebola outbreak, mobile phone apps were launched to combat the epidemic and train frontline health workers
| [24] | Tom-Aba, D., Nguku, P. M., Arinze, C. C. and Krause, G. (2018). Assessing the Concepts and Designs of 58 Mobile Apps for the Management of the 2014-2015 West Africa Ebola Outbreak: Systematic Review. JMIR Public Health and Surveillance, 4(4), p.e68. https://doi.org/10.2196/publichealth.9015 |
[24]
2.3. Research Gaps on mHealth Interventions in NCD Health Promotion in Africa
Several research gaps exist regarding mHealth interventions in NCD health promotion in Africa:
Effectiveness of mHealth Interventions: Current evidence on the effectiveness of mHealth interventions in promoting health literacy and NCD prevention and control in Africa is insufficient
| [25] | Betjeman, T.J., Soghoian, S.E. and Foran, M. P. (2013). mHealth in Sub-Saharan Africa. International Journal of Telemedicine and Applications, [online] 2013. https://doi.org/10.1155/2013/482324 |
[25]
. More research is needed to assess the impact of mHealth interventions on health promotion and literacy, and to identify the most effective interventions for different populations and contexts.
Diverse mHealth Platforms: Research in Sub-Saharan Africa predominantly focuses on SMS as the primary channel for mHealth interventions. There is a lack of comprehensive research comparing the effectiveness of different platforms in promoting health literacy in the region
.
Cross-Country Interventions: Cross-country mHealth interventions for health promotion in Sub-Saharan Africa are underexplored. Limited evidence exists on their feasibility and effectiveness. Comparative studies examining the implementation and impact of such interventions across different countries would provide valuable insights into their potential for addressing health literacy disparities in the region
| [26] | Kruse, C., Betancourt, J., Ortiz, S., Valdes Luna, S. M., Bamrah, I. K. and Segovia, N. (2019). Barriers to the Use of Mobile Health in Improving Health Outcomes in Developing Countries: Systematic Review. Journal of Medical Internet Research, [online] 21(10), p.e13263. https://doi.org/10.2196/13263 |
| [27] | Aranda-Jan, C. B., Mohutsiwa-Dibe, N. and Loukanova, S. (2014). Systematic review on what works, what does not work and why of implementation of mobile health (mHealth) projects in Africa. BMC Public Health, [online] 14(1). https://doi.org/10.1186/1471-2458-14-188 |
[26, 27]
To address these research gaps, investment in research is necessary to inform the development and implementation of effective, sustainable, and ethically sound mHealth interventions.
3. Research Methodology and Design
This study is a secondary analysis of outcome data from phase 1 of the NCD 365 project conducted by the Stowelink Foundation in Nairobi, Kenya, from January to December 2020. The study aims to:
Assess the feasibility and effectiveness of implementing cross-country mHealth interventions for health promotion in Sub-Saharan Africa.
3.1. Search Strategy
The search strategy involved finding articles from several databases by using specific key terms in combinations such as “eHealth”, “mHealth”, and “NCD” with the conjunctions ‘OR’ and ‘AND’. The timeframe of the articles was kept expansive to include the maximum number of studies. At this point, screening of the titles and abstracts was initiated to ensure only relevant studies were kept. After this the accepted articles were then analyzed thoroughly for data pertaining to the topic.
Database: Ovid MEDLINE(R) and Epub Ahead of Print, In-Process, In-Data-Review & Other Non-Indexed Citations, Daily and Versions <1946 to January 03, 2023>
Search Date: 04 January 2023
Search Question: The Impact of m-health Technologies on Improving Literacy on Non-Communicable Diseases in Africa.
Table 2. PICOS Framework.
S/N | PICOS concepts | Possible Search Terms |
1 | Population | Africa |
2 | Intervention | mHealth technologies |
3 | Comparator | N/A |
4 | Outcome | Literacy on noncommunicable diseases |
5 | Study design | Any study design |
The terms generated using the PICOS framework in
Table 2 above were used to identify the most appropriate MeSH terms and free text search terms for each concept as seen in
Table 3.
Table 3. Search Strategy.
Search Line (#) | Search Terms | Number of Results |
1 | exp Africa/ | 311756 |
2 | Telemedicine/ | 35433 |
3 | mobile health.ab,kf,ti. | 7781 |
4 | mHealth.ab,kf,ti. | 8353 |
5 | “mobile health solution*”.ab,kf,ti. | 69 |
6 | “mHealth solution*”.ab,kf,ti. | 181 |
7 | “mobile health technolog*”.ab,kf,ti. | 660 |
8 | “mHealthtechnolog*”.ab,kf,ti. | 708 |
9 | TelmHealth.ab,kf,ti. | 11877 |
10 | “TelmHealth solution*”.ab,kf,ti. | 103 |
11 | “TelmHealthtechnolog*”.ab,kf,ti. | 513 |
12 | digital health.ab,kf,ti. | 6170 |
13 | “digital health solution*”.ab,kf,ti. | 223 |
14 | “digital health technolog*”.ab,kf,ti. | 699 |
15 | 2 or 3 or 4 or 5 or 6 or 7 or 8 or 9 or 10 or 11 or 12 or 13 or 14 | 52658 |
16 | *Noncommunicable Diseases/ | 2363 |
17 | chronic noncommunicable diseases.ab,kf,ti. | 394 |
18 | “NCD*”.ab,kf,ti. | 9697 |
19 | “Chronic NCD*”.ab,kf,ti. | 86 |
20 | *Literacy/ | 789 |
21 | *Health Literacy/ | 6691 |
22 | (improv* adj2 health literacy).ab,kf,ti. | 1234 |
23 | 17 or 18 or 19 or 20 or 21 or 22 | 18105 |
24 | 1 and 15 and 23 | 22 |
3.2. Study Setting
The study was conducted in five African countries: Kenya, Uganda, Nigeria, Cameroon, and Zimbabwe. These countries were selected based on their participation in the NCDs 365 project and the presence of implementing partner organizations that coordinated the data collection process throughout the full calendar year of 2020.
3.3. Inclusion and Exclusion Criteria
3.3.1. Inclusion Criteria
Members of an implementing partner organization that executed the project for the entire year of 2020.
Members of each participating organization who were 18 years of age or older.
Participants who accessed the online resources at least once.
Individuals with basic English comprehension to complete the online questionnaire.
Participants who provided written informed consent.
3.3.2. Exclusion Criteria
Members from implementing partner organizations that did not execute the project for the full year of 2020.
Individuals unable to read, write, and respond in English.
Non-participants of the NCDs 365 project.
Individuals under the age of 18.
Non-residents or individuals residing outside the selected countries.
Individuals unable or unwilling to provide informed consent.
Inclusion and exclusion criteria were provided as a checklist to respondents in the online questionnaire, which was a prerequisite for completing the rest of the questionnaire.
3.4. Sampling
A multi-stage sampling technique was used to select study participants from the 8 participating countries, which included a total of 5186 participants in the project.
Stage One: Purposive Sampling Five countries were selected out of the eight participating countries in Sub-Saharan Africa. The selected countries were Cameroon, Kenya, Nigeria, Zimbabwe, and Uganda. The selection criteria included active local partner organizations involved in the on-ground implementation of the project and having commenced the implementation and monitoring of the NCDs 365 project from January 1, 2020, to December 31, 2020.
Stage Two: Convenience Sampling A questionnaire was distributed to 400 individuals who signed up for and actively participated in the NCDs 365 project across the five selected countries.
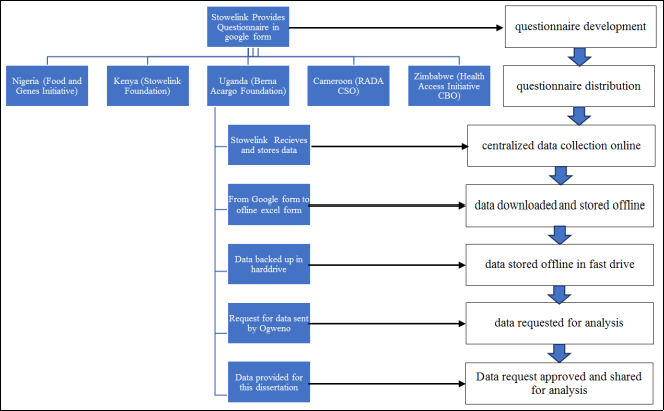
3.5. Data Collection Management and Storage
Data collection was conducted using an online Google form distributed through local organizations responsible for implementing the project. The Stowelink Foundation managed the form, ensuring centralized data collection, efficient data management, and secure data storage as shown in
figure 1 below.
Figure 1. Data Collection Management and Storage.
The online questionnaire consisted of 40 questions divided into two parts:
Part 1: Five questions on general characteristics (age, education, sex, country, employment status), duration of project exposure, and social media platforms accessed for project information.
Part 2: Questions assessing knowledge on NCDs, including overall knowledge, smoking and alcohol use, cardiovascular diseases, diabetes, chronic lung diseases, and mental health. The response categories included Likert scales, yes/no, true/false, and open-ended/free text responses. Questions were adopted from the WHO stepWISE survey questionnaires
.
3.6. Data Analysis
A thorough quality check was performed before data analysis to ensure reliability. Only participants who completed the entire questionnaire were included in the analysis. Descriptive statistics (mean, median, standard deviation) and inferential statistics (ANOVA) were used, with a significance level of p < 0.05 and a confidence level of 95%.
Scores were analyzed alongside control variables such as project exposure, participant country, social media platform engagement, and education levels, providing a comprehensive understanding of the research.
3.7. Hypothesis Testing
The research tested the following hypothesis:
It is feasible and effective to implement cross-country mHealth interventions for health promotion in sub-Saharan Africa.
A descriptive analysis was conducted to examine the implementation and outcomes of the cross-country mHealth intervention, summarizing key findings and outcomes across different countries to provide insights into its feasibility and effectiveness.
3.8. Ethical Considerations
The University Research Ethics Committees (URECs) in the United kingdom reviewed this research project under the number 10811457 which was presented from the University of Manchester and ensured that the research ethics for the research project were adhered to. Ethical considerations were of utmost importance in this research study, and measures were implemented to ensure the protection and confidentiality of the participants in accordance with the Helsinki Declaration. The study began by obtaining informed consent from the participants. To safeguard the privacy and confidentiality of the participants, the questionnaire deliberately avoided collecting personal identifying information such as names, emails, ID numbers, or phone numbers. Furthermore, the research study obtained written permission from the Stowelink Foundation, the primary custodian of the data, to use the secondary data for the study.
4. Results
4.1. Use of Different Online Communication Channels Across the 5 Countries
In Cameroon, WhatsApp emerged as the most widely used platform, selected by the majority of participants (58.7%), followed by Facebook (14.3%). Instagram, Twitter, Websites, and LinkedIn had lower usage rates. Similarly, in Kenya and Nigeria, WhatsApp was the dominant platform, chosen by a significant percentage of participants (71.8% and 69.6%, respectively).
However, in Uganda, the platform utilization pattern differed compared to other countries, with lower adoption rates for WhatsApp (20.0%) and higher adoption rates for Twitter (72.9%). Facebook, Instagram, Websites, and LinkedIn had minimal usage in Uganda. The results are indicated in
table 5 below:
Table 5. Online communication platform use per country.
Platform | Country |
Cameroon | Kenya | Nigeria | Zimbabwe | Uganda | cumulative |
Count | % | Count | % | Count | % | Count | % | Count | % | Count | % |
WhatsApp | 37 | 58.7% | 51 | 71.8% | 48 | 69.6% | 47 | 74.6% | 14 | 20.0% | 197 | 58.6 |
Twitter | 6 | 9.5% | 8 | 11.3% | 1 | 1.4% | 4 | 6.3% | 51 | 72.9% | 70 | 20.8 |
Facebook | 9 | 14.3% | 6 | 8.5% | 3 | 4.3% | 2 | 3.2% | 3 | 4.3% | 23 | 6.8 |
Instagram | 3 | 4.8% | 2 | 2.8% | 11 | 15.9% | 4 | 6.3% | 0 | 0.0% | 20 | 6.0 |
Websites | 6 | 9.5% | 1 | 1.4% | 5 | 7.2% | 4 | 6.3% | 2 | 2.9% | 18 | 5.4 |
LinkedIn | 2 | 3.2% | 3 | 4.2% | 1 | 1.4% | 2 | 3.2% | 0 | 0.0% | 8 | 2.4 |
Total | 63 | 100% | 71 | 100% | 69 | 100% | 63 | 100% | 70 | 100% | 336 | 100% |
Overall, WhatsApp consistently emerged as the popular platform across all countries, serving as the primary means for individuals to access health promotion communication. Twitter showed varying levels of popularity, ranging from 1.4% to 72.9%, depending on the country. Facebook, Instagram, Websites, and LinkedIn had relatively lower usage rates overall.
4.2. Literacy Distribution Across the 5 Countries
The
table 6 presents the adjusted literacy levels per country based on the original literacy levels in Cameroon, Kenya, Nigeria, Zimbabwe, and Uganda. The adjusted literacy levels provide a standardized measure that takes into account the distribution of literacy levels within the dataset.
From the
table 6 below, it can be observed that all five countries have similar original literacy levels, ranging from 76% to 80%. However, when considering the adjusted literacy levels, there are slight variations. Cameroon, Zimbabwe, and Uganda have relatively lower adjusted literacy levels, ranging from 15.17% to 15.75%. On the other hand, Kenya and Nigeria have slightly higher adjusted literacy levels, with Kenya at 15.75% and Nigeria at 15.39%.
Table 6. Literacy levels per country.
Country | Original Literacy Level | Adjusted Literacy Level |
Cameroon | 77% | 15.17% |
Kenya | 80% | 15.75% |
Nigeria | 78% | 15.39% |
Zimbabwe | 77% | 15.17% |
Uganda | 76% | 15.52% |
Mean | 77.57 | 15.24% |
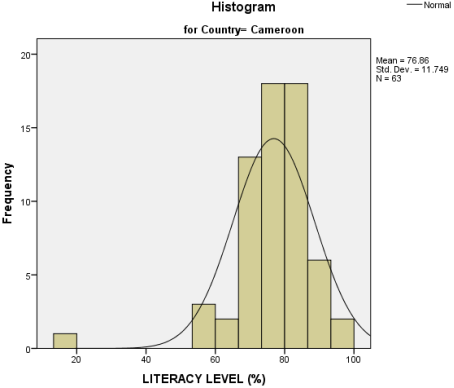
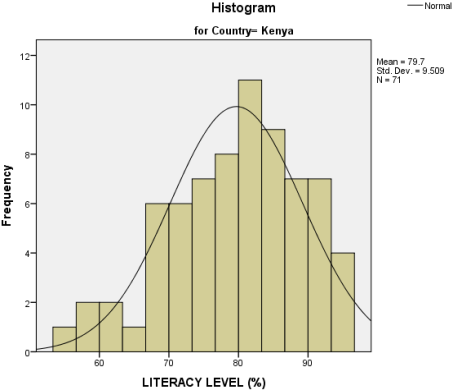
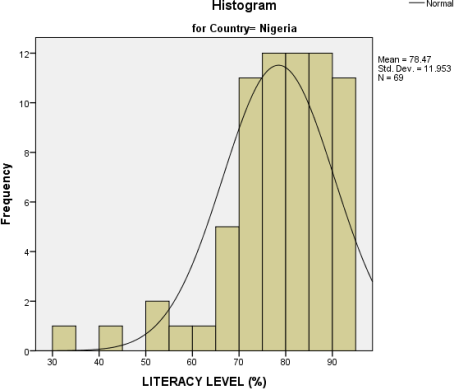
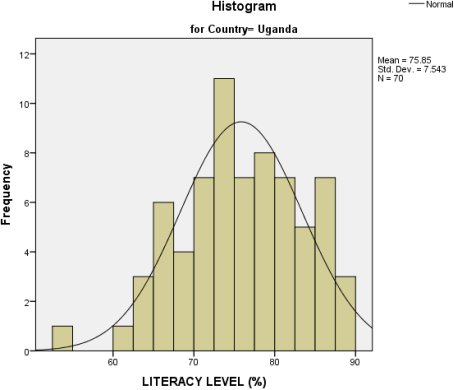
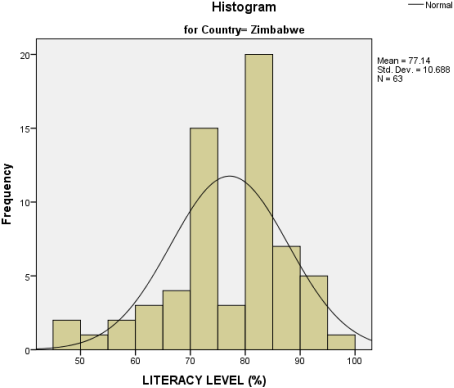
The analysis of literacy levels across the five countries revealed distinct patterns. Kenya, Cameroon, and Uganda showed a normal distribution of literacy levels, with most individuals clustered around the mean, but with a positive skewness indicating more individuals with higher literacy scores. In contrast, Nigeria and Zimbabwe had flatter, more dispersed literacy distributions, indicating a wider range of literacy levels, though these countries also exhibited positive skewness with a higher concentration of individuals scoring higher on literacy.
Figures 2-6 visually represents these distributions, illustrating the differences in kurtosis and skewness for each country.
Figure 2. Country wise literacy level in percentage – Cameroon.
Figure 3. Country wise literacy level in percentage – Kenya.
Figure 4. Country wise literacy level in percentage – Nigeria.
Figure 5. Country wise literacy level in percentage – Uganda.
Figure 6. Country wise literacy level in percentage – Zimbabwe.
4.3. Adjusted Average Literacy Levels for Each Country Disaggregated by Gender
Table 7 provides the adjusted average literacy levels for each country, categorized by gender. The overall adjusted average literacy levels range from 72.95 to 77.35 across the five countries. There is a consistent trend where males tend to have slightly higher literacy levels than females within each country. However, the differences in literacy levels between genders are relatively small, ranging from 0.07 to 0.11. Overall, the data suggests that the literacy levels are relatively similar between males and females in these countries.
Table 7. Adjusted average literacy levels for each country disaggregated by gender.
Country | Adjusted Average Literacy (Female) | Adjusted Average Literacy (Male) | Adjusted Average Literacy |
Cameroon | 73.97 | 74.05 | 74.02 |
Kenya | 77.32 | 77.37 | 77.35 |
Nigeria | 75.71 | 75.76 | 75.74 |
Zimbabwe | 73.08 | 73.16 | 73.12 |
Uganda | 72.91 | 72.98 | 72.95 |
4.4. Comparison of Average Health Literacy Levels Against Country and Platforms
The results presented in
Table 8 highlight the relationship between average health literacy levels and the platforms through which individuals accessed health promotion information and material in the NCDs 365 project, segmented by country.
Table 8. Comparison of average health literacy levels against countries and platforms.
Dependent Variable: LITERACY LEVEL (%) |
Platform | Country | Mean | Std. Deviation | N |
WhatsApp | Cameroon | 76.90 | 13.636 | 37 |
Kenya | 80.45 | 9.618 | 51 |
Nigeria | 76.84 | 11.182 | 48 |
Uganda | 72.70 | 9.430 | 14 |
Zimbabwe | 77.29 | 10.263 | 47 |
Total | 77.60 | 11.065 | 197 |
Facebook | Cameroon | 71.34 | 9.382 | 9 |
Kenya | 71.05 | 4.009 | 6 |
Nigeria | 82.82 | 7.173 | 3 |
Uganda | 83.41 | 8.540 | 3 |
Zimbabwe | 83.07 | 1.052 | 2 |
Total | 75.36 | 8.973 | 23 |
Instagram | Cameroon | 85.97 | 3.368 | 3 |
Kenya | 79.43 | 3.325 | 2 |
Nigeria | 79.81 | 17.378 | 11 |
Zimbabwe | 76.79 | 18.975 | 4 |
Total | 80.09 | 15.014 | 20 |
Twitter | Cameroon | 77.53 | 9.288 | 6 |
Kenya | 78.53 | 8.724 | 8 |
Nigeria | 89.76 | . | 1 |
Uganda | 76.16 | 6.581 | 51 |
Zimbabwe | 75.77 | 5.193 | 4 |
Total | 76.72 | 7.051 | 70 |
Websites | Cameroon | 78.47 | 5.227 | 6 |
Kenya | 87.80 | . | 1 |
Nigeria | 85.20 | 5.687 | 5 |
Uganda | 78.66 | 11.322 | 2 |
Zimbabwe | 78.29 | 11.728 | 4 |
Total | 80.84 | 7.744 | 18 |
LinkedIn | Cameroon | 80.45 | 1.557 | 2 |
Kenya | 84.86 | 14.953 | 3 |
Nigeria | 83.81 | . | 1 |
Zimbabwe | 68.84 | 21.003 | 2 |
Total | 79.62 | 13.226 | 8 |
Total | Cameroon | 76.86 | 11.749 | 63 |
Kenya | 79.70 | 9.509 | 71 |
Nigeria | 78.47 | 11.953 | 69 |
Uganda | 75.85 | 7.543 | 70 |
Zimbabwe | 77.14 | 10.688 | 63 |
Total | 77.57 | 10.401 | 336 |
In Cameroon, Instagram users had the highest average literacy rate at 86%, followed by LinkedIn at 80%, though both platforms were used by less than 10% of participants. WhatsApp was the most popular platform, used by 58.7% of participants with a 77% average literacy rate, while Facebook was used by 14.3%. In Kenya, websites had the highest literacy rate at 88%, followed by LinkedIn at 85%, both accounting for less than 10% of users. WhatsApp had a 71.8% usage rate with an 80% literacy rate, and Twitter was the second most popular platform. In Nigeria, Twitter users had the highest literacy at 90%, followed by LinkedIn at 84%, both with less than 10% usage. WhatsApp was the most used platform at 69.6%, with a 77% literacy rate, and Instagram was the second most popular. In Zimbabwe, Facebook led with an 83% literacy rate, followed by websites at 78%, both used by less than 10% of users. WhatsApp was used by 74.6% of participants. In Uganda, Facebook users had the highest literacy at 83%, followed by websites at 79%. Twitter was the most used platform at 72.9%, followed by WhatsApp at 20%.
4.5. Hypothesis Testing
In order to test hypothesis which states that it is feasible and effective to implement cross-country mHealth interventions for health promotion in sub-Saharan Africa, a descriptive analysis was conducted which involved comparing the differences on various countries where the project was implemented and summarizing key findings. The descriptive statistics above have not established any significant differences between the countries in terms of literacy and use of the various social media platforms. To analyze this further the Kruskal-Wallis test was carried out to assess whether there are significant differences in literacy rates and use of various online communication platforms among the countries of Cameroon, Kenya, Nigeria, Zimbabwe, and Uganda. The results are highlighted in the
table 9 below:
Table 9. Kruskal-Wallis test.
Test Statisticsa,b |
| Platform | Country |
Chi-Square | 41.582 | 44.703 |
df | 49 | 49 |
Asymp. Sig. | .765 | .648 |
a. Kruskal Wallis Test |
b. Grouping Variable: LITERACY LEVEL (%) |
The Kruskal-Wallis test results for "Platform" (χ² = 41.582, df = 49, p = 0.765) and "Country" (χ² = 44.703, df = 49, p = 0.648) show p-values greater than 0.05, indicating no significant differences in literacy levels across platforms or countries. Thus, the null hypothesis that there are no significant differences in literacy levels between platforms and countries cannot be rejected. These findings, along with the descriptive results, support the feasibility and effectiveness of implementing cross-country mHealth interventions like the NCDs 365 project for health promotion in Sub-Saharan Africa, as they can be conducted successfully despite regional differences.
5. Discussion
5.1. Summary of Key Findings
This study aimed to assess the feasibility and effectiveness of implementing cross-country mHealth interventions for health promotion in Sub-Saharan Africa, focusing on the NCD 365 project conducted by the Stowelink Foundation. The study spanned five countries: Cameroon, Kenya, Nigeria, Zimbabwe, and Uganda. Key findings are summarized as follows:
Platform Utilization: WhatsApp was the most widely used platform across most countries, except Uganda, where Twitter had the highest usage.
Literacy Distribution: While the original literacy levels were similar across countries, the adjusted literacy levels showed slight variations, with Kenya and Nigeria having slightly higher adjusted literacy levels compared to Cameroon, Zimbabwe, and Uganda.
Gender Differences: Males generally had marginally higher literacy levels than females, though the differences were not substantial.
Platform and Literacy Correlation: WhatsApp users demonstrated consistent literacy levels across countries, while platforms like Facebook, Twitter, and Instagram showed higher literacy levels but had lower overall usage rates.
Hypothesis Testing: The Kruskal-Wallis test indicated no significant differences in literacy levels across different platforms and countries, supporting the hypothesis that cross-country mHealth interventions are feasible and effective.
5.2. Discussion of Results
5.2.1. Use of Different Online Communication Channels
The predominance of WhatsApp as the primary communication platform for health promotion in Cameroon, Kenya, Nigeria, and Zimbabwe highlights its effectiveness and accessibility. WhatsApp's widespread usage is likely due to its ease of use, low cost, and high penetration rate in these countries. This aligns with previous studies that have identified WhatsApp as a critical tool for health communication in resource-limited settings
| [15] | Iribarren, S. J., Cato, K., Falzon, L. and Stone, P.W. (2017). What is the economic evidence for mHealth? A systematic review of economic evaluations of mHealth solutions. PLOS ONE, 12(2), p.e0170581. https://doi.org/10.1371/journal.pone.0170581 |
[15]
.
In contrast, Uganda's preference for Twitter underscores the variability in platform popularity and highlights the need for tailored mHealth strategies. The significant use of Twitter in Uganda may be attributed to specific demographic or regional preferences, indicating that mHealth interventions must consider local context and user preferences to maximize engagement and effectiveness
.
5.2.2. Literacy Distribution Across Countries
The adjusted literacy levels provide a nuanced understanding of health literacy across different countries. Kenya and Nigeria's slightly higher literacy levels suggest that these countries may have better educational infrastructure or more effective health promotion programs. Conversely, the lower adjusted literacy levels in Cameroon, Zimbabwe, and Uganda highlight areas that may require targeted interventions to boost health literacy.
The normal distribution of literacy levels in Kenya, Cameroon, and Uganda indicates a balanced spread of health literacy, while the flatter curves in Nigeria and Zimbabwe suggest more significant disparities in literacy levels. These findings emphasize the importance of customized interventions that address specific literacy needs within each country
| [12] | Berkman, N., Sheridan, S., Donahue, K., Halpern, D. and Crotty, K. (2011). Low health literacy and health outcomes: An updated systematic review. [online] Annals of Internal Medicine. Available at: https://pubmed.ncbi.nlm.nih.gov/21768583/ |
[12]
.
5.2.3. Gender Differences in Literacy Levels
The minimal differences in literacy levels between males and females suggest a relatively equitable distribution of health literacy across genders in the study countries. However, the slightly higher literacy levels among males may reflect broader socio-economic factors that influence educational opportunities and access to health information. This aligns with global trends where gender disparities in health literacy persist, albeit in varying degrees
| [13] | Kim, H. and Xie, B. (2017). Health literacy in the eHealth era: A systematic review of the literature. Patient Education and Counseling, 100(6), pp. 1073–1082. https://doi.org/10.1016/j.pec.2017.01.015 |
[13]
.
5.2.4. Correlation Between Platform Usage and Literacy Levels
The correlation between platform usage and literacy levels reveals interesting insights. While WhatsApp was the most popular platform, other platforms like Facebook, Twitter, and Instagram showed higher average literacy levels among their users. This suggests that individuals with higher literacy levels may prefer more diverse or specialized platforms for accessing health information.
These findings indicate that mHealth interventions should leverage multiple platforms to reach a broader audience and cater to different literacy levels and preferences. By doing so, health promotion efforts can be more inclusive and effective
| [14] | Lin, YH and Lou, MF eds., (2016). Effects of mHealth-based interventions on health literacy and related factors: A systematic review. [online] Europepmc.org. Available at: https://europepmc.org/article/med/33040429 [Accessed 6 Aug. 2024]. |
[14]
.
5.2.5. Feasibility and Effectiveness of Cross-Country mHealth Interventions
The hypothesis testing using the Kruskal-Wallis test did not find significant differences in literacy levels across different platforms and countries, supporting the feasibility and effectiveness of cross-country mHealth interventions. This suggests that standardized mHealth interventions like the NCDs 365 project can be successfully implemented across diverse settings, contributing to improved health literacy and promotion.
The consistent results across countries, despite their differences, demonstrate that mHealth interventions can be a powerful tool for health promotion in Sub-Saharan Africa. The success of the NCDs 365 project underscores the potential for scalability and adaptation of similar interventions to other regions and health issues
| [25] | Betjeman, T.J., Soghoian, S.E. and Foran, M. P. (2013). mHealth in Sub-Saharan Africa. International Journal of Telemedicine and Applications, [online] 2013. https://doi.org/10.1155/2013/482324 |
[25]
.
5.3. Implications for Practice and Policy
5.3.1. Leveraging Popular Platforms
Given the high usage rates of WhatsApp, health promotion programs should prioritize this platform while also incorporating other platforms like Twitter and Facebook to reach different segments of the population. Tailoring messages to suit the communication styles and preferences of each platform can enhance engagement and effectiveness.
5.3.2. Addressing Literacy Disparities
To address literacy disparities, targeted interventions should be developed to improve health literacy in countries with lower adjusted literacy levels. Educational programs, community outreach, and localized content can help bridge these gaps and ensure more equitable health outcomes.
5.3.3. Gender-Sensitive Approaches
While gender differences in literacy levels were minimal, efforts should continue to ensure that both males and females have equal access to health information. Gender-sensitive approaches that consider the unique needs and challenges faced by different genders can promote inclusivity and equity in health promotion.
5.3.4. Comprehensive mHealth Strategies
Developing comprehensive mHealth strategies that leverage multiple platforms can enhance the reach and impact of health promotion efforts. These strategies should consider local contexts, preferences, and literacy levels to maximize engagement and effectiveness.
5.3.5. Policy Support
Policy makers should support the integration of mHealth interventions into national health strategies. By providing the necessary infrastructure, funding, and regulatory frameworks, governments can facilitate the successful implementation and scaling of mHealth programs.
5.4. Future Research Directions
5.4.1. Longitudinal Studies
Future research should conduct longitudinal studies to assess the long-term impact of mHealth interventions on health literacy and outcomes. This can provide deeper insights into the sustainability and effectiveness of such interventions over time.
5.4.2. Platform-Specific Studies
Further studies should explore the effectiveness of different mHealth platforms in various contexts. Understanding platform-specific impacts can help tailor interventions more precisely and improve overall outcomes.
5.4.3. Cross-Regional Comparisons
Comparative studies across different regions within Sub-Saharan Africa can highlight regional differences and best practices. This can inform more contextually appropriate mHealth strategies and promote knowledge sharing among countries.
5.4.4. Impact on Health Outcomes
Future research should also examine the direct impact of improved health literacy through mHealth interventions on specific health outcomes. This can provide concrete evidence of the benefits and justify further investments in mHealth initiatives.
5.5. Conclusion
This research evaluated the feasibility and effectiveness of implementing cross-country mHealth interventions for health promotion in Sub-Saharan Africa through the NCD 365 project. The study, conducted across Cameroon, Kenya, Nigeria, Zimbabwe, and Uganda, demonstrated that WhatsApp was the most widely used platform for health communication.
The analysis revealed that mHealth interventions could effectively reach diverse populations and improve health literacy across different platforms and countries. Despite some disparities, the findings support the hypothesis that cross-country mHealth interventions are both feasible and effective in promoting health literacy in Sub-Saharan Africa. These insights underscore the potential of mHealth strategies to enhance healthcare delivery, especially in resource-limited settings. Future research should focus on long-term impacts and platform-specific studies to further refine and optimize mHealth interventions for broader and more effective health promotion.
Abbreviations
CBOS | Community Based Organizations |
CDC | Center For Disease Control |
EHEALTH | Electronic Health |
HIV | Human Immunodeficiency Virus |
MHEALTH | Mobile Health |
NCDS | Non-Communicable Diseases |
RCT | Random Control Trials |
WHO | World Health Organization |
Author Contributions
Ogweno Stephen: Conceptualization, Data curation, Formal Analysis, Investigation, Methodology, Project administration, Validation, Writing – original draft
Harrison Roger: Formal Analysis, Methodology, Project administration, Supervision, Writing – review & editing
Murithi Bernard: Formal Analysis, Software, Visualization
Otieno Bonface: Formal Analysis, Software, Visualization
Conflicts of Interest
The authors declare no conflicts of interest in relation to this study. The research was conducted independently, and there were no financial, personal, or professional influences that could have affected the study design, data collection, analysis, or interpretation. The NCD 365 project was implemented with transparency and ethical considerations, and the authors affirm that there are no competing interests that may have influenced the outcomes or conclusions presented in this paper.
References
| [1] |
Kidanemariam, A. (2011). RETHINKING HEALTH PROMOTION AND DISEASE PREVENTION IN AFRICA: THE QUEST FOR AN INTEGRATED MODEL. [online] Available at:
https://www.jstor.org/stable/45198650
|
| [2] |
Kumar, S. and Preetha, G. (2022). Health promotion: an Effective Tool for Global Health. Indian Journal of Community Medicine, [online] 37(1), pp. 5–12.
https://doi.org/10.4103/0970-0218.94009
|
| [3] |
Seppälä, T., Hankonen, N., Korkiakangas, E., Ruusuvuori, J. and Laitinen, J. (2017). National policies for the promotion of physical activity and healthy nutrition in the workplace context: a behaviour change wheel guided content analysis of policy papers in Finland. BMC Public Health, 18(1).
https://doi.org/10.1186/s12889-017-4574-3
|
| [4] |
Azevedo, M. J. (2019). The State of Health System(s) in Africa: Challenges and Opportunities. Historical Perspectives on the State of Health and Health Systems in Africa, Volume II, [online] 2, pp. 1–73.
https://doi.org/10.1007/978-3-319-32564-4_1
|
| [5] |
World Health Organisation (2023). WHO EMRO | eHealth | Health topics. [online] World Health Organization - Regional Office for the Eastern Mediterranean. Available at:
https://www.emro.who.int/health-topics/ehealth/
|
| [6] |
Sanders, M., Tobin, J. N., Cassells, A., Carroll, J., Holder, T., Thomas, M., Luque, A. and Fiscella, K. (2020). Can a brief peer-led group training intervention improve health literacy in persons living with HIV? Results from a randomized controlled trial. Patient Education and Counseling.
https://doi.org/10.1016/j.pec.2020.10.031
|
| [7] |
McCool, J., Dobson, R., Whittaker, R. and Paton, C. (2021). Mobile Health (mHealth) in Low- and Middle-Income Countries. Annual Review of Public Health, 43(1).
https://doi.org/10.1146/annurev-publhealth-052620-093850
|
| [8] |
Bigna, J. J. and Noubiap, J. J. (2019). The rising burden of non-communicable diseases in sub-Saharan Africa. The Lancet Global Health, [online] 7(10), pp.e1295–e1296.
https://doi.org/10.1016/s2214-109x(19)30370-5
|
| [9] |
Gouda, H. N., Charlson, F., Sorsdahl, K., Ahmadzada, S., Ferrari, A. J., Erskine, H., Leung, J., Santamauro, D., Lund, C., Aminde, L. N., Mayosi, B. M., Kengne, A. P., Harris, M., Achoki, T., Wiysonge, C.S., Stein, D. J. and Whiteford, H. (2019). Burden of non-communicable diseases in sub-Saharan Africa, 1990–2017: results from the Global Burden of Disease Study 2017. The Lancet Global Health, 7(10), pp.e1375–e1387.
https://doi.org/10.1016/s2214-109x(19)30374-2
|
| [10] |
Agner, J., KathArine Elizabeth Bau and Bruland, D. (2024). An Introduction to Health Literacy and Social Contexts with Recommendations for Health Professionals and Researchers. International Journal of Environmental Research and Public Health, 21(2), pp.240–240.
https://doi.org/10.3390/ijerph21020240
|
| [11] |
Kreps GL (2017). The Relevance of Health Literacy to mHealth. Studies in health technology and informatics, [online] 240. Available at:
https://pubmed.ncbi.nlm.nih.gov/28972527/
[Accessed 6 Aug. 2024].
|
| [12] |
Berkman, N., Sheridan, S., Donahue, K., Halpern, D. and Crotty, K. (2011). Low health literacy and health outcomes: An updated systematic review. [online] Annals of Internal Medicine. Available at:
https://pubmed.ncbi.nlm.nih.gov/21768583/
|
| [13] |
Kim, H. and Xie, B. (2017). Health literacy in the eHealth era: A systematic review of the literature. Patient Education and Counseling, 100(6), pp. 1073–1082.
https://doi.org/10.1016/j.pec.2017.01.015
|
| [14] |
Lin, YH and Lou, MF eds., (2016). Effects of mHealth-based interventions on health literacy and related factors: A systematic review. [online] Europepmc.org. Available at:
https://europepmc.org/article/med/33040429
[Accessed 6 Aug. 2024].
|
| [15] |
Iribarren, S. J., Cato, K., Falzon, L. and Stone, P.W. (2017). What is the economic evidence for mHealth? A systematic review of economic evaluations of mHealth solutions. PLOS ONE, 12(2), p.e0170581.
https://doi.org/10.1371/journal.pone.0170581
|
| [16] |
Marcolino, M. S., Oliveira, J. A. Q., D’Agostino, M., Ribeiro, A. L., Alkmim, M. B. M. and Novillo-Ortiz, D. (2018). The Impact of mHealth Interventions: Systematic Review of Systematic Reviews. JMIR mHealth and uHealth, [online] 6(1), p.e23.
https://doi.org/10.2196/mhealth.8873
|
| [17] |
Ali, A. O. A. and Prins, M. H. (2020). Patient Characteristics Associated with Non-Adherence to Tuberculosis Treatment: A Systematic Review. Journal of Tuberculosis Research, [online] 08(02), pp. 73–92.
https://doi.org/10.4236/jtr.2020.82008
|
| [18] |
Murthy, N., Chandrasekharan, S., Prakash, M. P., Ganju, A., Peter, J., Kaonga, N. and Mechael, P. (2020). Effects of an mHealth voice message service (mMitra) on maternal health knowledge and practices of low-income women in India: findings from a pseudo-randomized controlled trial. BMC Public Health, 20(1).
https://doi.org/10.1186/s12889-020-08965-2
|
| [19] |
Jahan, Y., Rahman, M. M., Faruque, A. S. G., Chisti, M. J., Kazawa, K., Matsuyama, R. and Moriyama, M. (2020). Awareness Development and Usage of Mobile Health Technology Among Individuals With Hypertension in a Rural Community of Bangladesh: Randomized Controlled Trial. Journal of Medical Internet Research, 22(12), p.e19137.
https://doi.org/10.2196/19137
|
| [20] |
Ben-Zeev, D., Chander, A., Tauscher, J., Buck, B., Nepal, S., Campbell, A. and Doron, G. (2021). A Smartphone Intervention for People With Serious Mental Illness: Fully Remote Randomized Controlled Trial of CORE. Journal of Medical Internet Research, 23(11), p.e29201.
https://doi.org/10.2196/29201
|
| [21] |
Ihekweazu, C. and Agogo, E. (2020). Africa’s response to COVID-19. BMC Medicine, [online] 18(1).
https://doi.org/10.1186/s12916-020-01622-w
|
| [22] |
Nachega, Jean B et al. “Contact Tracing and the COVID-19 Response in Africa: Best Practices, Key Challenges, and Lessons Learned from Nigeria, Rwanda, South Africa, and Uganda.” The American journal of tropical medicine and hygiene vol. 104, 4 1179-1187. 11 Feb. 2021,
https://doi.org/10.4269/ajtmh.21-0033
|
| [23] |
Jahun, I., Said, I., El-Imam, I., Ehoche, A., Dalhatu, I., Yakubu, A., Greby, S., Bronson, M., Brown, K., Bamidele, M., Boyd, A.T., Bachanas, P., Dirlikov, E., Agbakwuru, C., Abutu, A., Williams-Sherlock, M., Onotu, D., Odafe, S., Williams, D.B. and Bassey, O. (2021). Optimizing community linkage to care and antiretroviral therapy Initiation: Lessons from the Nigeria HIV/AIDS Indicator and Impact Survey (NAIIS) and their adaptation in Nigeria ART Surge. PloS One, [online] 16(9), p.e0257476.
https://doi.org/10.1371/journal.pone.0257476
|
| [24] |
Tom-Aba, D., Nguku, P. M., Arinze, C. C. and Krause, G. (2018). Assessing the Concepts and Designs of 58 Mobile Apps for the Management of the 2014-2015 West Africa Ebola Outbreak: Systematic Review. JMIR Public Health and Surveillance, 4(4), p.e68.
https://doi.org/10.2196/publichealth.9015
|
| [25] |
Betjeman, T.J., Soghoian, S.E. and Foran, M. P. (2013). mHealth in Sub-Saharan Africa. International Journal of Telemedicine and Applications, [online] 2013.
https://doi.org/10.1155/2013/482324
|
| [26] |
Kruse, C., Betancourt, J., Ortiz, S., Valdes Luna, S. M., Bamrah, I. K. and Segovia, N. (2019). Barriers to the Use of Mobile Health in Improving Health Outcomes in Developing Countries: Systematic Review. Journal of Medical Internet Research, [online] 21(10), p.e13263.
https://doi.org/10.2196/13263
|
| [27] |
Aranda-Jan, C. B., Mohutsiwa-Dibe, N. and Loukanova, S. (2014). Systematic review on what works, what does not work and why of implementation of mobile health (mHealth) projects in Africa. BMC Public Health, [online] 14(1).
https://doi.org/10.1186/1471-2458-14-188
|
| [28] |
WHO (n.d.). STEPwise Approach to NCD Risk Factor Surveillance (STEPS). [online] Available at:
https://www.who.int/teams/noncommunicable-diseases/surveillance/systems-tools/steps
|
Cite This Article
-
APA Style
Stephen, O., Roger, H., Bernard, M., Bonface, O. (2025). Evaluating Feasibility and Effectiveness of Implementing Cross-Country Mhealth Interventions in Sub-Saharan Africa. American Journal of Health Research, 13(1), 28-42. https://doi.org/10.11648/j.ajhr.20251301.12
 Copy
|
Copy
|
 Download
Download
ACS Style
Stephen, O.; Roger, H.; Bernard, M.; Bonface, O. Evaluating Feasibility and Effectiveness of Implementing Cross-Country Mhealth Interventions in Sub-Saharan Africa. Am. J. Health Res. 2025, 13(1), 28-42. doi: 10.11648/j.ajhr.20251301.12
Copy
|
Download
AMA Style
Stephen O, Roger H, Bernard M, Bonface O. Evaluating Feasibility and Effectiveness of Implementing Cross-Country Mhealth Interventions in Sub-Saharan Africa. Am J Health Res. 2025;13(1):28-42. doi: 10.11648/j.ajhr.20251301.12
Copy
|
Download
-
@article{10.11648/j.ajhr.20251301.12,
author = {Ogweno Stephen and Harrison Roger and Murithi Bernard and Otieno Bonface},
title = {Evaluating Feasibility and Effectiveness of Implementing Cross-Country Mhealth Interventions in Sub-Saharan Africa},
journal = {American Journal of Health Research},
volume = {13},
number = {1},
pages = {28-42},
doi = {10.11648/j.ajhr.20251301.12},
url = {https://doi.org/10.11648/j.ajhr.20251301.12},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ajhr.20251301.12},
abstract = {Non-communicable diseases (NCDs) pose a significant public health challenge in Sub-Saharan Africa, where traditional healthcare systems in Sub-Saharan Africa often grapple with limited infrastructure, healthcare worker shortages, and accessibility challenges. Mobile health (mHealth) interventions have emerged as promising tools to enhance health promotion and literacy, providing innovative solutions to these challenges. This study evaluates the feasibility and effectiveness of cross-country mHealth interventions through a secondary analysis of the NCD 365 project, which utilized outcome data from January to December 2020. A multi-stage sampling technique was employed to select participants from five countries, and data were collected via an online Google form. The analysis focused on platform usage, literacy distribution, and the relationship between health literacy levels and the platforms used. Descriptive statistics and the Kruskal-Wallis test were used to evaluate the data. Results indicated that WhatsApp was the most widely used platform in four of the five countries, while Twitter predominated in Uganda. Adjusted literacy levels varied slightly, with Kenya and Nigeria showing higher levels compared to Cameroon, Zimbabwe, and Uganda. Gender differences in literacy were minimal, with males displaying marginally higher literacy scores. The Kruskal-Wallis test revealed no significant differences in literacy levels across platforms or countries, reinforcing the feasibility and effectiveness of cross-country mHealth interventions. These findings suggest that initiatives like the NCD 365 project can effectively promote health literacy and healthcare delivery across diverse settings in Sub-Saharan Africa. While regional differences in platform preferences exist, the overall success of the project highlights the potential for scalable and adaptable mHealth strategies. Future research should focus on the long-term impacts and platform-specific effectiveness to further optimize mHealth interventions.},
year = {2025}
}
Copy
|
Download
-
TY - JOUR
T1 - Evaluating Feasibility and Effectiveness of Implementing Cross-Country Mhealth Interventions in Sub-Saharan Africa
AU - Ogweno Stephen
AU - Harrison Roger
AU - Murithi Bernard
AU - Otieno Bonface
Y1 - 2025/01/22
PY - 2025
N1 - https://doi.org/10.11648/j.ajhr.20251301.12
DO - 10.11648/j.ajhr.20251301.12
T2 - American Journal of Health Research
JF - American Journal of Health Research
JO - American Journal of Health Research
SP - 28
EP - 42
PB - Science Publishing Group
SN - 2330-8796
UR - https://doi.org/10.11648/j.ajhr.20251301.12
AB - Non-communicable diseases (NCDs) pose a significant public health challenge in Sub-Saharan Africa, where traditional healthcare systems in Sub-Saharan Africa often grapple with limited infrastructure, healthcare worker shortages, and accessibility challenges. Mobile health (mHealth) interventions have emerged as promising tools to enhance health promotion and literacy, providing innovative solutions to these challenges. This study evaluates the feasibility and effectiveness of cross-country mHealth interventions through a secondary analysis of the NCD 365 project, which utilized outcome data from January to December 2020. A multi-stage sampling technique was employed to select participants from five countries, and data were collected via an online Google form. The analysis focused on platform usage, literacy distribution, and the relationship between health literacy levels and the platforms used. Descriptive statistics and the Kruskal-Wallis test were used to evaluate the data. Results indicated that WhatsApp was the most widely used platform in four of the five countries, while Twitter predominated in Uganda. Adjusted literacy levels varied slightly, with Kenya and Nigeria showing higher levels compared to Cameroon, Zimbabwe, and Uganda. Gender differences in literacy were minimal, with males displaying marginally higher literacy scores. The Kruskal-Wallis test revealed no significant differences in literacy levels across platforms or countries, reinforcing the feasibility and effectiveness of cross-country mHealth interventions. These findings suggest that initiatives like the NCD 365 project can effectively promote health literacy and healthcare delivery across diverse settings in Sub-Saharan Africa. While regional differences in platform preferences exist, the overall success of the project highlights the potential for scalable and adaptable mHealth strategies. Future research should focus on the long-term impacts and platform-specific effectiveness to further optimize mHealth interventions.
VL - 13
IS - 1
ER -
Copy
|
Download